Breech Presentation: Types, Diagnosis, & Management
advertisement

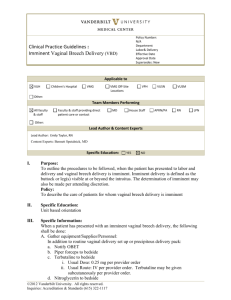
Breech presentation Commonest malpresentation The lie is longitudinal The podalic pole presents at the pelvic brim Varieties Frank breech Flexed breech Footling presentation Etiology Prematurity Twins Oligohydramnios Congenital uterine malformations IUD Placenta praevia Hydrocephalus Contracted pelvis Multipara Diagnosis P/A head at the upper pole of the uterus. FHS are heard at a higher level round about the umbilicus P/V soft and irregular parts are felt U/S X-ray abdomen MANAGEMENT OF VAGINAL BREECH DELIVERY First Stage P/V for the detection of cord prolapse Pt to be kept in the bed to preserve membranes Only water is given orally and i/v fluid to maintain hydration Careful watch for uterine contractions SECOND STAGE OF LABOUR THREE METHODS SPONTANEOUS 10% Very little assistance other than support of the baby usually in Multigravida and small babies ASSISTED BREECH Delivery is assisted from the beginning to the end this method should be employed Breech Extraction Entire body is extracted with minimum aid by the mother Assisted Breech Delivery STEPS Pt In lithotomy position when posterior buttock distends the perineum Episiotomy Pt encouraged to bear down No touch policy is adopted till the buttocks are delivered with the legs in flexed breech and the trunk slips upto the umblicus Contd Extended legs are disengaged Umbilical cord mobilized to minimize compression Keep the feta back anterior Baby is wrapped Delivery of the arms if extended by Loveset’s maneuver Delivery of the after coming head Forceps delivery Jaw flexion and shoulder traction (Mauriceau – Smellie – Veit technique) Third stage of labour Resuscitation of the baby Third stage Uneventful Ergometrine is given i/v at crowning of the head Indications of caesarean section Other obstetric reasons of caesarean Poor progress of labour Cord prolapse or cord presentation Appearance of fetal or maternal distress Thank You