Toxicité hématologique des
chimiothérapies
Pr Jean Trédaniel
Unité de cancérologie thoracique
Hôpital Saint-Louis
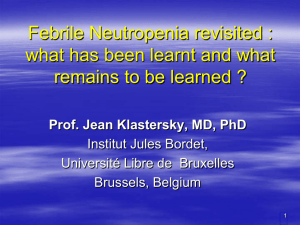
Chimiothérapie
ADN
Système réplicatif
cellulaire
Tissus à renouvellement
rapide, dont le système
hématopoïétique
Cinétique des cellules
sanguines périphériques
• Granulocytes: 6 heures
• Plaquettes: 10 jours
• Hématies: 120 jours
leucopénie
thrombopénie
anémie
temps
Physiopathologie
Chemotherapy agents
Antimetabolites
Alkylating agents
more toxic to mature
not cell cycle dependent;
but still dividing progenitor cells
than to more primitive and less
mitotically active cells
active to primitive stem cells
that have minimal mitotic
activity
earlier and less
severe myelosuppression
delayed and profound
myelosuppression
Pharmacogenetics
• Pharmacogenetics may influence the
development of hematologic toxicity
• Metabolic processes for drug
inactivation are polymorphic
• Ex: polymorphic deficiency of
dihydropyrimidine dehydrogenase
results in increased toxicity of 5-FU,
including hematologic toxicity
A few chemotherapeuty agents result
in virtually no myelosuppression
•
•
•
•
Bleomycin
L-asparaginase
Vincristine
streptozotocine
Modifying the drug administration schedule
can reduce the bone marrow toxicity (1)
5-FU
IV bolus injection:
dose-limiting toxicity:
bone marrow suppression
IV protracted infusion:
dose-limiting toxicities:
mucositis & hand-and-foot
syndrome; myelosuppression
occurs rarely
Modifying the drug administration schedule
can reduce the bone marrow toxicity (2)
• The myelosuppressive effects of paclitaxel
consist primarily of granulocytopenia, with an
increase in the incidence and severity of
neutropenia observed with increasing doses,
• Identical doses of paclitaxel are markedly less
myelosuppressive when delivered by 3-hr than
by 24-hr infusion,
• Neutropenia is not related to paclitaxel’s peak
concentration or to the AUC but rather to the
duration that the plasma concentration is
aboce a certain threshold (>=0,05 µmol/L).
• Neutropénie
– Risque infectieux
• Anémie
– Asthénie, dyspnée
• Thrombopénie
– Hémorragie
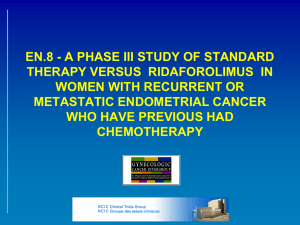
PNN
Leucocytes
Lymphocytes
Grade
Hb (gr/dl)
(103/mm3) (103/mm3) (103/mm3)
Plaquettes
(103/mm3)
0
>= 4,0
>= 2,0
>= 2,0
N
N
1
3,0 - 3,9
1,5 - 1,9
1,5 - 1,9
10,0 - N
75,0 - N
2
2,0 - 2,9
1,0 - 1,4
1,0 - 1,4
8,0 - 9,9
50,0 - 74,9
3
1,0 - 1,9
0,5 - 0,9
0,5 - 0,9
6,5 - 7,9
25,0 - 49,9
4
< 1,0
<0,5
<0,5
< 6,5
< 25,0
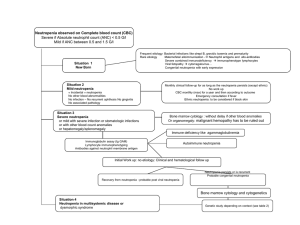
Neutropénie
• la neutropénie compromet la réponse
inflammatoire à l’infection,
• en réduisant les signes et symptômes de
l’infection (« pas de PNN = pas de pus =
pas de foyer ») elle atténue la
présentation clinique (« simple fièvre),
• malgré le risque de choc septique !
Neutropénie: facteurs de risque
dépendants du patient
• Hémopathie maligne (atteinte intrinsèque
du système hématopoïétique + intensité
des chimiothérapies) > tumeur solide
• Âge physiologique élevé
• Taux de LDH élevé
• Fièvre élevée, hypotension à l’admission
• Lymphopénie, hypoalbuminémie
• Conséquence hématologique de la
première cure de chimiothérapie
Crawford et al. Cancer 2004;100:228-37.
Early lymphopenia after cytotoxic chemotherapy as a risk
factor for febrile neutropenia.
• Cohorte rétrospective de 112 patients traités
consécutivement, avec des régimes divers de
chimiothérapie
– 2 facteurs de risque identifiés
• taux de lymphocytes < = 700/µl à J5
• type de la chimiothérapie (forte dose versus
autres)
– Modèle avec 0,1 ou 2 facteurs de risque
• Validation du modèle
– Série du Centre Léon Bérard (Lyon): 3%, 19 %, 67%
– Série de l’IGR: 6%, 19%, 75%
– Patients traités par ACVBP (= un facteur de risque)
au CLB 1988-92: 33%, 72%.
Blay et al. J Clin Oncol 1996;14:636-43.
Incidence of Life-Threatening Neutropenia, Neutropenic Infection, and Death in Older
Individuals With Large-Cell Non-Hodgkin’s Lymphomas Treated With CHOP-Like Regimens
Febrile
neutropenia
(%)
Treatment
related
deaths (%)
Author
n
regimen
age
Neutropenia
(%)
Zinzani
161
VNCOP-B
60+
44
32
1,3
Sonneveld
148
CHOP
CNOP
60+
60+
-
-
14
13
Gomez
267
CHOP
60+
70+
-
-
12
14
Tirelli
120
VMP
CHOP
70+
70+
50
48
21
21
7
5
Bastion
444
CVP
CTVP
70+
70+
9
29
7
13
12
15
O’Reilly
63
POCE
65+
50
20
8
Bjorkholm
104
CHOP
60
91
47
-
Bertini
57
P-VEBEC
65+
46
18
2
Armitage
20
CHOP
70+
-
-
30
Balducci. J Clin Oncol 2001;19:1583-5.
Risk-models for predicting chemotherapy-induced neutropenia.
Lyman et al. Oncologist 2005;10:427-37.
Risk factors for chemotherapy induced neutropenia
• Disease specific
– Tumor type
– Advanced disease & uncontrolled cancer
• Patient specific
– Age
– PS
– Comorbidities
– Laboratory abnormalities
• Treatment specific
– Chemotherapy regimen
– CSF use
Lyman et al. Oncologist 2005;10:427-37.
Risk of first episode of febrile neutropenia in patients with
non-Hodgkin’s lymphoma treated with CHOP chemotherapy.
Lyman et al. Oncologist 2005;10:427-37.
Risk of Febrile Neutropenia Among Patients with Intermediategrade Non-Hodgkin's Lymphoma Receiving CHOP Chemotherapy.
•
•
•
577 intermediate grade NHL patients who received CHOP chemotherapy
160 patients experienced 224 febrile neutropenia events
The risk of febrile neutropenia was significantly associated with:
•
First febrile neutropenic events occurred by day 14 of cycle 1 in one-half of
patients experiencing febrile neutropenia.
In multivariate analysis, the risk of febrile neutropenia remained
significantly associated with:
•
–
–
–
–
–
–
age ≥65 years (p=0.001),
cardiovascular disease (p=0.020),
renal disease (p=0.006),
baseline hemoglobin <12 g/dl (p=0.018),
>80% planned average relative dose intensity (ARDI; p=0.018),
and no prophylactic colony-stimulating factor (CSF) use (p=0.046).
–
–
–
–
–
–
age ≥65 years (HR=1.65, 95% CI: 1.18-2.32),
renal disease (HR=1.91, 95% CI: 1.10-3.30),
cardiovascular disease (HR=1.54, 95% CI: 1.02-2.33),
baseline hemoglobin <12 g/dl (HR=1.44, 95% CI: 1.04-2.00),
>80% planned CHOP ARDI (HR=2.41, 95% CI: 1.30-4.47),
and no CSF prophylaxis (HR=2.13, 95% CI: 1.20-3.76).
Lyman et al. Leukemia & Lymphoma 2003;44:2069-76.
Risk of Febrile Neutropenia Among Patients with Intermediategrade Non-Hodgkin's Lymphoma Receiving CHOP Chemotherapy.
Cumulative probability of febrile neutropenia, by number of risk factors.
Lyman et al. Leukemia & Lymphoma 2003;44:2069-76.
2000 update of recommendations for the use of hematopoietic colonystimulating factors: evidence-based, clinical practice guidelines.
•
•
•
•
•
•
Routine use of CSFs for primary prophylaxis of FN for any common disease in previously
untreated patients is not justified,
The available data indicate that, with a sufficiently high incidence of FN ( 40%), there is
strong evidence for the primary administration of CSFs to reduce hospitalization for
antibiotic administration.
Secondary prophylaxis: physicians should consider chemotherapy dose reduction after
neutropenic fever or severe or prolonged neutropenia after the previous cycle of
treatment,
CSFs should not be routinely used for patients with neutropenia who are afebrile,
CSFs should not be routinely used as adjunct therapy for the treatment of
uncomplicated fever and neutropenia. Uncomplicated fever and neutropenia are defined
as follows: fever of 10 days in duration; no evidence of pneumonia, cellulitis, abscess,
sinusitis, hypotension, multiorgan dysfunction, or invasive fungal infection; and no
uncontrolled malignancies,
Certain patients with fever and neutropenia are at higher risk for infection-associated
complications and have prognostic factors that are predictive of poor clinical outcome.
The use of a CSF for such high-risk patients may be considered, but the benefits of a
CSF in these circumstances have not been proven. These factors include profound (ANC
< 100/µL) neutropenia, uncontrolled primary disease, pneumonia, hypotension, multiorgan
dysfunction (sepsis syndrome), and invasive fungal infection. Age greater than 65 years
and posttreatment lymphopenia may also be high-risk factors but have not been
consistently confirmed by multicenter trials.
Ozer et al. J Clin Oncol 2000;18:3558-85.
NCCN - National Comprehensive Cancer Network
Myeloid Growth Factors in Cancer Treatment version 1.2005
• The NCCN panel members recommend
the routine use of CSFs for high-risk
(>20%) patients to prevent the
development of FN in patients
receiving treatment with curative
intent, adjuvant therapy, or
treatment expected to prolong
survival or to improve QOL.
(www.NCCN.org)
NCCN - Myeloid growth factors guidelines
Risk of FN
High
> 20 %
Intermediate
10 - 20 %
Low
< 10 %
CSF
Consider CSF
no CSF
NCCN - Myeloid growth factors guidelines
Evaluation of prior
chemotherapy cycle
Febrile neutropenia
or dose-limiting
neutropenic event
Prior use of CSF
No prior use of CSF
Consider dose
reduction or change
in treatment regimen
Consider CSF
No febrile neutropenia
or dose-limiting
neutropenic event
Repeat intervention
for the subsequent cycle
Colony-stimulating factors for chemotherapyinduced febrile neutropenia: a meta-analysis of
randomized controlled trials.
Overall mortality
Clark et al. J Clin Oncol 2005;23:4198-214.
Colony-stimulating factors for chemotherapyinduced febrile neutropenia: a meta-analysis of
randomized controlled trials.
Infection-related mortality
Clark et al. J Clin Oncol 2005;23:4198-214.
Colony-stimulating factors for chemotherapyinduced febrile neutropenia: a meta-analysis of
randomized controlled trials.
Lenght of hospitalisation
Clark et al. J Clin Oncol 2005;23:4198-214.
Colony-stimulating factors for chemotherapyinduced febrile neutropenia: a meta-analysis of
randomized controlled trials.
Time to neutrophil recovery
Clark et al. J Clin Oncol 2005;23:4198-214.
Antibacterial prophylaxis after chemotherapy for
solid tumors and lymphomas.
Patients who were receiving cyclic chemotherapy for solid tumors or lymphoma and who
were at risk for temporary, severe neutropenia (fewer than 500 neutrophils per cubic
millimeter).
Patients were randomly assigned to receive either 500 mg of levofloxacin once daily
or matching placebo for seven days during the expected neutropenic period.
levofloxacin
placebo
p
n
781
784
1st cycle-FN (%)
3,5
7,9
<0,001
at least 1 FN (%)
10,8
15,2
0,01
probable infection (%)
34,2
41,5
0,004
hospitalisation (%)
15,7
21,6
0,004
severe infection (%)
1,0
2,0
0,15
N infection related
deaths
4
4
Cullen et al. NEJM 2005;353:988-98.
Risk model for severe anemia requiring red blood cell transfusion
after cytotoxic conventional chemotherapy regimens.
•
•
•
•
•
One hundred seven of the 1,051 patients of the CLB-1996 cohort (10%) experienced
SARRT.
In univariate analysis:
– female sex,
– performance status greater than 1,
– hemoglobin level less than 12 g/dL before chemotherapy on day 1 (d1),
– d1 lymphocyte count <= 700/µL significantly correlated with the risk of SARRT.
Using logistic regression:
– d1 hemoglobin level less than 12 g/dL (OR = 14.0; 95% CI, 7 to 30),
– performance status greater than 1 (OR = 2.2; 95% CI, 1.4 to 3.5),
– d1 lymphocyte count <= 700/µL (OR = 1.7; 95% CI, 1.1 to 2.6) were identified as
independent risk factors for SARRT.
These three factors were given arbitrary risk coefficients of 3, 1, and 1 respectively,
and a risk score for each individual patient was obtained by adding the coefficients.
The calculated probability of RBC transfusions was 30% for patients with a score 4,
and 11%, 4%, and 1% in patients with a score of 2 or 3, 1, and 0 respectively.
Ray-Coquard et al. J Clin Oncol 1999;17:2840
A risk model for thrombocytopenia requiring platelet
transfusion after cytotoxic chemotherapy.
•
•
•
•
Cohort of the 1,051 patients (CLB 1996) treated with chemotherapy
In univariate analysis:
– performance status (PS) greater than 1,
– platelet count less than 150,000/µL at day 1 (d1) before the initiation of
chemotherapy,
– d1 lymphocyte count <= 700/µL,
– d1 polymorphonuclear leukocyte count less than 1,500/µL,
– and the type of chemotherapy (high risk v others) were significantly associated
(P < .01) with an increased risk of severe thrombocytopenia requiring platelet
transfusions.
Using logistic regression:
– d1 platelet count less than 150,000/µL (OR, 4.3; 95% CI, 1.9 to 9.6),
– d1 lymphocyte counts <= 700/µL (OR, 3.37; 95% CI, 1.77 to 6.4),
– the type of chemotherapy (OR, 3.38; 95% CI, 1.77 to 6.4),
– and PS greater than 1 (OR, 2.23; 95% CI, 1.22 to 4.1) were identified as independent
risk factors for platelet transfusions.
The observed incidences of platelet transfusions were 45%, 13%, 7%, and 1.5% for
patients with 3, 2, 1, or 0 risk factors, respectively. This model was then tested in
3 groups of patients treated with chemotherapy used as validation samples:
Blay et al. Blood 1998;92:405-10.
Chronic bone marrow damage
• Decreased bone marrow reserve,
• Myelodysplastic syndromes and
secondary leukemias.