Care of Patients with Inflammatory
Intestinal Disorders
Chapter 60
Mrs. Kreisel MSN, RN
NU130 Adult Health
Summer 2011
Appendicitis
• Acute inflammation of the vermiform
appendix—the blind pouch attached to the
cecum of the colon
• Abdominal pain in the epigastric or
periumbilical area is the initial symptom of
classic appendicitis
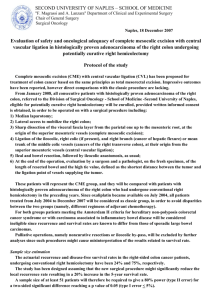
• McBurney’s point: In accute appendicitis
tenderness situated between the unbilicus
and the right anteriosuperior iliac crest
• Perforation: Puncuture or holes
• Rebound tenderness
McBurney’s
Point
Interventions
• Nonsurgical management includes:
• NPO
• IV fluids
• Semi-Fowler’s position
• Analgesics
• No laxatives or enemas
• No heat
• PROVIDE COMFORT TOUCH AND
REASSURANCE!
Surgical Management
• Laparoscopy or laparotomy to rule out
appendicitis
• Preoperative care as for general
anesthesia surgeries
• Operative procedure—appendectomy
• Postoperative care
Peritonitis
• Life-threatening acute inflammation of
visceral/parietal peritoneum and
endothelial lining of abdominal cavity, or
peritoneum
• Primary or secondary peritonitis
• Rigid, boardlike abdomen, abdominal pain,
distended abdomen, high fever,
tachycardia, dehydration, low urine output,
hiccups, compromised respiratory status,
nausea and vomiting
• ASSESS FOR BOWEL SOUNDS
FREQUENTLY
Peritonitis
(Cont.)
Nonsurgical Management
•
•
•
•
•
•
•
•
IV fluids
Broad-spectrum antibiotics
Daily weight monitored
Fluid volume assessed
Nasogastric suctioning
NPO status
Oxygen
Pain management
Surgical Management
• Exploratory laparotomy
• Semi-Fowler's position
• Wound care:
• Care of the incisions and drains
• Peritoneal irrigation
• IV fluid replacement
Gastroenteritis
• Increase in the frequency and water
content of stools or vomiting as a result of
inflammation of the mucous membranes of
the stomach and intestinal tract
• Differs from food poisoning
• Bacterial form—Campylobacter, Shigella,
Escherichia coli
• Viral form—Norwalk virus
Interventions
•
•
•
•
•
Fluid replacement
Nutrition therapy
Drug therapy
Skin care
Health teaching
Inflammatory Bowel Disease (IBD)
• Several disorders of the GI tract with no
known etiology
• Ulcerative colitis
• Crohn’s disease
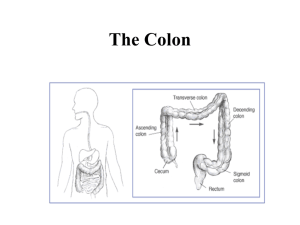
Ulcerative Colitis
• Widespread inflammation of mainly the
rectum and rectosigmoid colon; can
extend to the entire colon
• Associated with periodic remissions and
exacerbations
• Tenesmus
• Loose stools containing blood and mucus,
poor absorption of vital nutrients, and
thickening of the colon wall can result
• Increased risk for colon cancer
Assessment
•
•
•
•
•
Physical assessment
Clinical manifestations
Psychosocial assessment
Laboratory assessment
Other diagnostic tests
Drug Therapy
•
•
•
•
•
Aminosalicylates
Glucocorticoids
Immunomodulators
Antidiarrheal drugs
Other drugs
Other Therapies
• Nutrition therapy
• Rest
• Complementary and alternative therapies
Surgical Management
• Colectomy
• Total proctocolectomy with a permanent
ileostomy
• Preoperative care
• Operative procedure
• Postoperative care:
• Loose, dark green liquid, with some
blood in stool
• Pouch system worn at all times
• Skin care
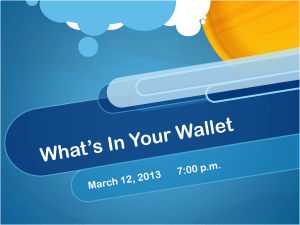
Total Colectomy with a Continent
(Kock’s) Ileostomy
• Internal ileal reservoir
• Intra-abdominal pouch created from the
terminal ileum by the surgeon
• Stool stored in the pouch drained by
catheter
• Care of pouch
• Effluent, or drainage, monitored
Kock’s
Ileostomy
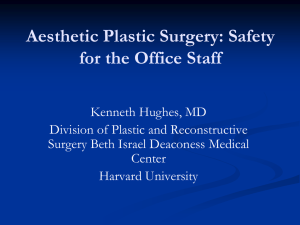
Total Colectomy with Ileoanal
Anastomosis (J Pouch)
• Removal of the colon and the rectum with
the ileum sutured into the anal canal
• Spares the rectal sphincter and need for
an ostomy
• Preoperative care
• Operative procedure
• Postoperative care
Ileoanal
Reservoir
Crohn’s Disease
• Inflammatory disease of the small intestine and the
colon, or both.
• It can affect the GI tract from mouth to anus but mostly
the terminal ileum.
• Transmural inflammation causing thickening of the
bowel wall with strictures and deep ulcerations with
bowel fistulas commonly developing.
• Rarely, cancer of the small bowel and colon develop.
• Malabsorption of vitamins and nutrients due to
diarrhea. It can lead to signs and symptoms of
anemia!
Fistulas
Assessment
•
•
•
•
Physical assessment
Clinical manifestations
Psychosocial assessment
Diagnostic assessment
Nonsurgical Management
•
•
•
•
•
•
•
•
Drug therapy
Nutritional therapy
Fistula management
Complication management
Fluid and electrolyte therapy
Skin care
Prevention of infection
Complementary and alternative therapies
Skin
Barriers
Surgical Management
• Laparoscopy
• Small bowel resection and ileocecal
resections
• Stricturoplasty
• Preoperative care
• Operative procedure
• Postoperative care
Diverticular Disease
• Diverticulosis is the presence of many
abnormal pouchlike herniations in the wall
of the intestine.
• Diverticulitis is inflammation of one or
more of the diverticula.
Diverticula
Assessments
•
•
•
•
History
Physical assessment
Clinical manifestations
Diagnostic assessment
Nonsurgical Management
•
•
•
•
•
•
•
Drug therapy
Nutrition therapy
Rest
IV fluids to correct dehydration
IV antibiotics
Anticholinergics
Analgesics
Nonsurgical Management (Cont’d)
• Avoid laxatives and enemas
• Rest
• NPO in the hospital
Surgical Management
• Preoperative care
• Operative procedure
• Postoperative care:
• Drain care
• Care of the ostomy
• NPO followed by clear liquids
Anorectal Abscess
• Localized induration and pus caused by
inflammation of the soft tissue near the
rectum or anus
• Rectal pain first symptom
• Surgical incision and drainage
• Nursing interventions focused on helping
the patient maintain comfort and optimal
perineal hygiene
• High-fiber diet
Anal Fissure
•
•
•
•
•
Tear in the anal lining
Acute and chronic forms
Assessment
Management
Patient teaching
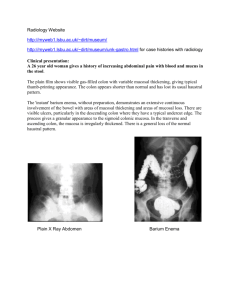
Anal Fistula
• Abnormal tract leading from the anal canal
to the perianal skin
• Most anal fistulas result from anorectal
abscesses
• Proctoscopy
• Surgery
Anal
Fistula
Parasitic Infection
•
•
•
•
•
•
Pathophysiology
Entamoeba histolytica
Giardia lamblia
Cryptosporidium
Assessment
Interventions
Helminthic (worms) Infestation
• ROUND WORMS: cause the most infections
worldwide
• Enterobiasis: pinworm most common in the
USA. Oral intake
• Trichinosis: very low in the USA roundworm.
Get from under cooked meat
• Hookworms: roundworm enter body through
the skin
• Tapeworms: From undercooked meat, eating
bugs, contaminated water
• WHAT NURSING CONSIDERATIONS ARE
IMPORTANT?
Food Poisoning
•
•
•
•
Salmonellosis
Staphylococcal infection
Escherichia coli infection
Botulism
•NCLEX TIME
Question 1
Ulcerative colitis is most commonly seen in
individuals
belonging to which ethnic group?
A.
B.
C.
D.
Hispanic
Sephardic Jews
Portuguese Romani
Ashkenazi Jews
Question 2
An older patient diagnosed with bacterial
gastroenteritis is complaining of abdominal
cramping, diarrhea, nausea and vomiting,
and fatigue for the past 24 hours. The nurse
should monitor the patient for what priority
assessment?
A. Dehydration
B. Hypokalemia
C. Hypernatremia
D. Perineal skin breakdown
Question 3
What is an expected outcome of a patient
taking
sulfasalazine (Azulfidine) for treatment of
ulcerative
colitis?
A.
B.
C.
D.
Anorexia
Anemia
Diarrhea
Dermatitis
Question 4
The patient has recently been placed on
corticosteroids as treatment for ulcerative
colitis. The nurse should monitor his
laboratory results for evidence of:
A. Hypernatremia
B. Hypercalcemia
C. Hyperglycemia
D. Hyperkalemia
Question 5
How many people are infected with
Salmonella organism each year in the United
States?
A. 10,000
B. 20,000
C. 40,000
D. 50,000