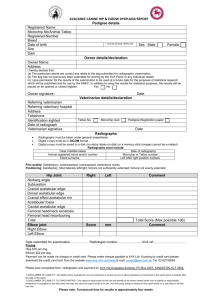
Femoracetabular
Impingement: In Theory
and In Practice
Tom Bradbury, MD
Assistant Professor
Emory Orthopaedics and
Spine Center
March 11, 2011
A delay in non-arthroplasty treatment
options for the hip…….
•
•
•
•
•
Hip pain in the young patient not as common
Hip is “deeper” than knee, shoulder
Hip is more constrained
Hip capsule is very robust
Precarious blood supply to the femoral head
limited an interest in surgical exposure…a fear
of iatrogenic avascular necrosis
What is the etiology of
osteoarthritis of the hip?
“90% of adult cases of osteoarthritis are the
result of a morphologic developmental
abnormality”…..not a intrinsic problem with
articular cartilage
- Murray, 1965
- Harris, 1986
“Structural Pediatric Residuals”
• Developmental Dysplasia
• Slipped Capital Femoral Epiphysis
• Legg-Calve-Perthes Disease
• Multiple Epiphyseal Dysplasia
• Spondyloepiphyseal Dysplasia
Radiography of Hips with FAI
• Normal joint space
• Subtle morphologic aberrations
“Normal” to the untrained eye
• 1991: “cervico-acetabular impingement” secondary
to femoral neck malunion
• 1999: “pincer” type impingement after
periacetabular osteotomy for dysplasia
Evolution of an Understanding
• Reinhold Ganz
•Anatomy
•Perfusion
•Osteotomy
•Dislocation
•Impingement
Ganz’s Observation
“Overcorrection” of hip dysplasia with
periacetabular osteotomy
“Iatrogenic retroversion”
Hip pain with flexion
(Pincer type anterior impingement)
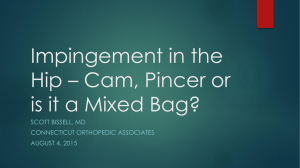
Normal
Cam
Pincer
Hip “History”
•
•
•
•
Arthrosis
Pre-arthrosis
Insidious onset
• Sudden onset
Constant Ache
• Sharp, intermittent
pain
Walking on level
ground
• Pain primarily with
Nocturnal symptoms torsional activities
• Pain with prolonged
flexion
Hip Exam: Gait
• “Antalgic” – shortened stance phase
secondary to pain
• “Trendelenberg” – contralateral hip drops
during stance phase secondary to abductor
dysfunction
• “Abductor Lurch” – torso sways over affected
leg during stance phase secondary to abductor
dysfunction
Hip Specific Tests
•
•
•
•
•
•
•
•
•
•
•
•
•
•
•
Trendelenberg Test
Log Roll
Passive External Rotation in Extension
“C” test
Thomas Test
Stinchfield Test
Ober’s Test
Anterior Impingement Test (FADDIR)
Posterior Impingement Test
DEXTRIT (aka McCarthy)- Dynamic External Rotatory Impingement Test
DIRIT- Dynamic Internal Rotatory Impingement Test
Scour Test
Ober
Abduction internal rotation
FABER
Hypermobility
• Beighton’s Criteria for hypermobility (3 of 5)
– Thumb to forearm
– SF extension > 90
– Elbow hyperextension > 10
– Knee hyperextension > 10
– Palms to floor
Findings
• Drehmann’s Sign- Obligate abduction and
external rotation with forward flexion of the
hip
• Coxa Saltans Interna- Iliopsoas tendon over
the ileopectineal eminence
• Coxa Saltans Externa- Iliotibial band over
greater trochanter
Imaging of the Young Hip
Start with plain films:
1. Supine AP Pelvis Centered Low with Legs
internally rotated 15 degrees
2. Cross table lateral of the hip with the leg 15
internally rotated 15 degrees
3. Dunn 45 of the Hip
Technique:
• AP
– Supine with legs 15 degrees internally rotated
– Film-focus distance: 1.2 meters
– Point of center: midway between ASIS & Pubis
• Cross Table Lateral
– Leg 15 degrees internally rotated
– Perpendicular to long axis of femoral neck
Technique
• Dunn 45
– Hip flexed 45 degree, abducted 20, in neutral rotation
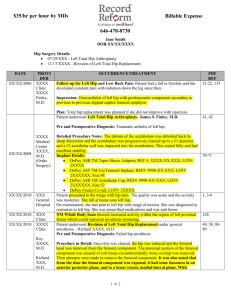
“Diagnosis can only be made from
a technically sound and properly
positioned AP radiograph of the
pelvis”
-Ganz
“Normal”
LEGS EXTERNALLY ROTATED
ROTATION?
MALROTATION
Distance from tip of coccyx to
superior edge of symphasis?
1 – 3 cm
Siebenrock et al.
From Sacrococcygeal junction:
Male = 47.3 mm
Female = 32.3 mm
TILT?
ASIS
PUBIS
POINT OF
CENTER?
Normal Landmarks
Iliopectineal Line
Ilioischial Line
Sourcil
Posterior Wall
Anterior Wall
Physeal Scar
Hip Imaging Lingo
• Acetabular Depth
• Acetabular Extrusion
• Acetabular Inclination
• Femoral Head Coverage
• Acetabular Version
• Head Sphericity
• Head-Neck Offset
• Congruency
Acetabular Depth
• The relationship of the true floor of
the acetabulum to the ilioischial line
•Extrusion Index
Extrusion Index
A
E
E/A+E
Normal = 25%
Cox Profunda
-Floor of fossa medial
to ilioischial line
- Extrusion Index 0
Cox Profunda
-Floor of fossa medial
to ilioischial line
- Extrusion Index 0
Acetabular Protrusio
-Femoral head to ilioischial line
-Negative Extrusion Index
Acetabular Inclination (Tonnis angle)
•Horizontal line between center of femoral heads
•Line connected the medial and lateral edge of the
sourcil
Acetabular Inclination (Tonnis angle)
Negative angle = overcoverage/pincer
Acetabular Inclination (Tonnis angle)
High positive angle = dysplasia
Lateral Center Edge Angle (of Wiberg)
• Normal = 25 - 40
Sphericity
•Measured by
containment of
physeal scar with
circle of femoral head
Acetabular Version
•
•
•
Relationship of walls to one another
Ischial spine within pelvis
Relationship of posterior wall
to center of femoral head
Dysplasia
• Low CE angle (< 25)
• Elevation of acetabular inclination
• Elevation of Extrusion index
Retroverted Acetabulum
• Cross over sign
• Ischial Spine within pelvis
False profile view
Posterior
Anterior
Aspherical head
• Physeal Scar extends beyond
the circle
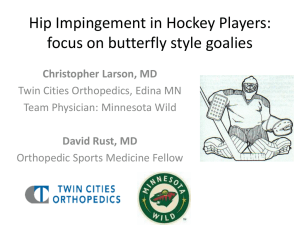
Femoral Cam
•Alpha angle > 50
Dunn 45
 0
0