View Poster - Clinical Audit Support Centre
advertisement

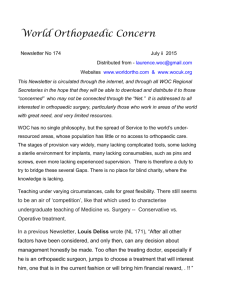
Surviving Major Trauma in the U.K : Are we prepared? V Teoh , M Khan, K Sindali, R Alamouti, N Cavale Department of Plastic Surgery, St Thomas’ Hospital, London victoriasteoh@gmail.com INTRODUCTION INTERVENTION Trauma is the leading cause of death across age groups and is responsible for 16,000 deaths in the U.K. annually. On reviewing the data from the first audit cycle, the Trust improved funding for trauma services with the establishment of dedicated trauma operating lists and the appointment of a dedicated cross-site Orthoplastic consultant. Following a national review in 2011, Regional Trauma Networks were established to reform and replace the ad hoc, unstructured trauma service. Comprehensive, evidence-based (BOAST-4) guidelines were produced. They are now the standard to which all practitioners involved in major trauma should adhere to. Collaboration between Orthopaedic and Plastic surgery has proved central to re-defining care, particularly in the management of open lower limb fractures with extensive soft tissue damage. Referral pathways between the 2 specialties were improved at local and regional level. The audit cycle was repeated with prospective data collection from January to December 2012. RESULTS The time taken from point of injury to transfer to a Major Trauma Centre improved from 17.5 to 6.2 days. 20 17.5 AIM To evaluate performance of the South East London Kent & Medway Trauma Network in the management of open lower limb fractures, against parameters set by the BOAST guidelines. 10 All patients with high energy, open fractures of the lower limb should have : The time taken for definitive skeletal stabilization and soft tissue reconstruction improved from 9.47 to 5.43 days. “Early referral and transfer of care to a Major Trauma Centre unless the patient is unstable” “Definitive skeletal stabilization and soft tissue reconstruction achieved within 72 hours and not exceed 7 days.” ‘Clear documentation of a combined orthopaedic and plastic surgical plan.” METHODS Retrospective data was collected on all open lower limb fractures admitted to Kings College Hospital with off-site plastic surgery cover at St Thomas’ Hospital (Jan-Dec 2011). 6.2 0 10 9.47 5.43 5 0 Documentation improved from 0 to 100% from 2011 to 2012. CONCLUSIONS Collaboration between Orthopaedic and Plastic surgery is key in managing Major Trauma. Unstructured management of this patient group has been associated with avoidable death and significant disability. A further study is underway to determine the impact of our audit on patient outcomes. Reference 1. BOA/ BAPRAS BOAST-4 Guidelines: The management of severe open lower limb fractures.