B. anthracis
advertisement

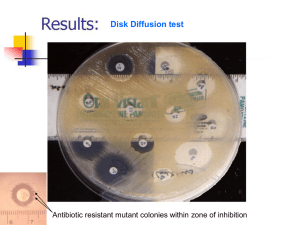
Gram-positive bacilli A. Bacillus sp. 1. Characteristics a. Aerobic, spore-forming, gram-positive rod 2. Epidemiology a. B. anthracis found in soil; causes anthrax i. transmission through inhalation of spores, breaks in skin/mucous membranes, or ingestion b. B. cereus found in nature i. transmission through traumatic introduction, contaminated medical equipment, or ingestion of contaminated food c. Many other sp. found in the environment; generally considered non-pathogens 3. Pathogenesis a. B. anthracis i. capsule: antiphagocytic ii. toxins: edema toxin and lethal toxin that mediate tissue destruction iii. cutaneous, pulmonary (“wool sorters”), and GI b. B. cereus i. enterotoxins and pyogenic toxins ii. diarrheal and emetic food poisoning iii. post-traumatic eye infections, endocarditis, bacteremia. B. Listeria monocytogenes 1. Characteristics a. Small, thin, catalase-positive GPR 2. Epidemiology a. Can be normal GI flora, found in the environment, as well as animals b. transmission through ingestion of contaminated food (meat and dairy); also mother to fetus in colonized moms 3. Pathogenesis a. Listeriolysin: hemolysin and cytotoxin permitting survival within macrophages b. bacteremia and meningitis, usually in neonates or immunosuppressed C. Corynebacterium sp. 1. Characteristics a. pleomorphic, catalase + GPR 2. Epidemiology a. normal URT and skin flora; also NF of animals b. person to person or endogenous 3. Pathogenesis a. C. diphtheriae i. diphtheria toxin: exotoxin that destroys cells Respiratory dipth: pseudomembrane exudates; respir compromise; toxin affects organs Cutaneous: non-healing ulcers b. C. jeikeium i. resistance to multiple antibiotics ii. septicemia, wound infections D. Laboratory diagnosis 1. Specimen collection, transport, processing a. In general, no special requirements b. Bacillus cereus from suspected food poisoning i. Heat or alcohol shock specimen; only spores will survive c. Listeria from placenta i. difficult to isolate from this source; cold enrichment at 4C for several weeks-months 2. Direct detection a. Bacillus: gram positive rods; size varies with species i. Spore stain: Malachite green stains spores, safranin stains vegetative cells ii. location of spores helps in ID if required b. Listeria: small GPR; may form short chains and be confused with streptococci c. Corynebacterium: palisading GPR; Chinese letters 3. Culture and identification a. Bacillus i. grow well on BAP; CAP ii. various colony morphologies and colors: large, flat, spready, wrinkly; white, gray, green iii. some are beta-hemolytic iv. Gram stain and colony morphology are usually sufficient; full ID not warranted v. commonly considered a contaminant Bacillus sp. on Gram stain http://textbookofbacteriology.net/Anthrax.html Left: B. cereus Right: B. anthracis http://textbookofbacteriology.net/Anthrax.html 3. Culture and identification b. Listeria i. grow well on BAP and CAP ii. small white or translucent colonies; beta hemolytic iii. CAMP positive iv. Motile; umbrella motility Listeria sp. on Gram stain http://www.geocities.com/CapeCanaveral/3504/gallery.htm 3. Culture and identification c. Corynebacterium i. most grow well on BAP and CAP ii. C. diphtheriae requires selective and differential media (freshly prepared) Cystine-tellurite: black or gray colonies Tinsdale’s: black with dk brown halos iii. others are infrequently ID’d, common contaminants iv. Listeria and Coryne ID’d by API strip if required Corynebacterium sp. on Gram stain http://www.life.umd.edu/classroom/bsci424/PathogenDescriptions/Corynebacterium.htm C. diphtheriae on Tellurite agar 4. Susceptibility testing and therapy a. MIC guidelines exist, but only test in severe disease b. Bacillus: Vanco, cipro c. Listeria: Pen, Amp d. C. diptheriae: anti-toxin plus pen or erythro i. vaccine DPT to toxoid e. Other corynes: all suscep to vanco Aerobic actinomycetes Branching, filamentous, gram-positive rods Some are partially acid-fast Difficult to recognize clinically and difficult to isolate Nocardia, Streptomyces, Rhodococcus, Tsukamurella A. Nocardia 1. Characteristics a. beaded, gram-positive, variably acid-fast (depends on media), catalase positive, strict aerobe b. Form substrate hyphae (filaments along agar surface) and aerial hyphae (in air) c. 11 species, N. asteroids, N. brasiliensis are most common 2. Epidemiology and Pathogenesis a. World-wide inhabitants of soil and water, responsible for decomposition of plant material b. Can be colonizers or cause infection following traumatic inoculation or inhalation c. Intracellular pathogens, prevent destruction in phagocytes, tropism for neural tissue 3. Spectrum of disease a. Immune competent: skin infections i. Mycetoma ii. Lymphocutaneous iii. Skin abscesses or cellulitis b. Immune compromised: pulmonary and disseminated i. pulmonary disease is non-specific, so risk factors add it to differential ii. organism can spread hematogenously from primary site, resulting in brain and/or skin lesions (dissemination = poor prognosis) Nocardia mycetoma http://www.thelancet.com/journals/laninf/article/PIIS1473-3099(09)70347-0/abstract 4. Laboratory diagnosis a. Specimen collection i. No special requirements; multiple specimens may be required to increase sensitivity ii. single isolate is of questionable significance iii. form micro-colonies or granules in tissues b. Direct detection i. characteristic gram-stain, but also may be difficult to see ii. modified acid-fast positive 1% sulfuric acid rather than 3% HCl as decolorizer Gram stain of Nocardia http://home.primus.com.au/royellis/nocast.html a. Culture i. can grow on BAP, CAP, and fungal media ii. may take 48-72 h to grow, so can be overgrown by normal flora Selective media: BCYE contains polymixin, anisomycin and vanco iii. Colony morphology is variable: wrinkled, dry, crumbly; chalky-white to orange-tan b. Identification i. Growth rate, colony morphology, gram stain ii. Urease +: cleaves urea, increases pH pink iii. Lysozyme resistant: can grow in its presence iv. Species id: use of casein, xanthine an tyrosine and starch hydrolysis: Quad plates, hold for 1 month Colonial morphologies of selected Nocardia sp. http://www.toyama-mpu.ac.jp/hp/clla/saikin/senshokuzou/gram_right.html Quad plate for ID of Nocardia sp. http://path.upmc.edu/cases/case315.html 5. Susceptibility testing and antimicrobial therapy a. Standardized method are available; ? in vitro-in vivo correlation; routinely requested for every patient b. Trimethoprim/sulfamethoxazole is primary drug of choice