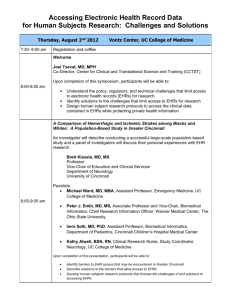
System acquisition refers to the process that
occurs from the time the decision is made to
select a new system until the time a contract
has been negotiated and signed.
System implementation begins once the
organization has acquired the system and
continues through the early stages following
the go-live date
Support &
Evaluation
Planning &
Analysis
Implementation
Design
Panning & Analysis
Examine current systems and problems to identify
opportunities for improvement (independent of
technology)
If new IS is needed, what are the information needs of the
users and what are the functional requirements?
Design
In-house, outside developer? Or purchase from a vendor
or contract with an Application Service Provider (ASP)
“the cloud”
All the alternatives are considered, cost-benefit is done
and a system is selected
Implementation
Support & Evaluation
Workflow and process analyses
Installing new system
Training, converting data
Longest phase in the life cycle
The first two states are referred to as the
acquisition process the second two
implementation
Health care executive team should
Engage in strategic information systems
planning
Identify goals and strategies and how IT will
be employed to aid the organization in
achieving them
Establish IT priorities
Gain budgetary approval and institutional
support
Establish Project Steering Committee
Primary function is to plan, organize, coordinate,
and manage all aspects of the acquisition process.
Project manager Is critical
Often clinicians with training in informatics
Chief medical informatics officers or nursing
informatics officers
Size of the committee
Define Project Objectives and Scope of Analysis
What does the committee expect to achieve?
What process will be used to ensure success?
How will milestones be acknowledged?
How will committee communicate progress?
What resources are needed?
Screen the Marketplace and review Vendor
Profiles
Determine System Goals
The system goals should be aligned with the strategic
goals of the organization and should serve as measures of
success throughout the system acquisition process.
Determine and Prioritize System Requirements
Focus groups/interviews/written surveys/product
demonstrations
Software
Technical infrastructure
Training and support
Develop and Distribute RFP or RFI
RFP tend to be highly detailed and are costly and time
consuming to develop
RFI is considerably shorter
Some may send RFI and then RFP to screened vendors
Explore Other Acquisition Options
Contract with an ASP
On a subscription basis to deliver an application and
provide the support. Buy vs. lease
Benefits
Requires less IT staff
Fewer up-front costs and less capital
Rapid deployment
Disadvantages
Off the shelf
Technical support will not be site specific
Data ownership, security and privacy worries
Explore Other Acquisition Options
Evaluate Vendor Proposals
Contract with a system developer or build in-house
Develop evaluation criteria
Vendor demonstrations
Make Site visits/check references
Conduct Cost-Benefit Analysis
Prepare Summary Report and
Recommendations
Conduct Contract Negotiations
Organize the Implementation Team and
Identify a Champion
May contain some of the members of the selection
team, but also others
System champion is someone who is well respected
in the organization, sees the new system as necessary
to the organization and is passionate about
implementing it.
EG:
Physician (system champion), nurse manager, lab
manager, radiology director, CIO, IT analysis, business
manager
Determine Project Scope and Expectations
Should be consistent with the system goals
established in the system selection process
Establish and Institute a Project Plan
Major tasks and milestones
Estimated duration of each task
Dependencies among tasks
Resources and budget
Individuals responsible for completing each task
Target dates
Measures for evaluating completion and success
Workflow and Process Analysis
Analyze current process and procedures
Identify opportunities for improvement
Identify sources of data
Determine location and number of workstations
Redesign physical location as needed
Involving users at this stage is critical
System installation
Determine system configuration
Order and install hardware
Upgrade or implement IT infrastructure
Install software and interfaces
Test, rest, and test again
Staff training and procedure manuals
How much training? Do different groups have different
training needs?
Who should conduct the training?
When should the training occur? What intervals of
training are ideal?
What training format is best (classroom, one-on-one,
small group, computer-based?)
What is the role of the vendor?
Who in the organization will manage or oversee the
training? How is it documented?
What criteria and methods will be used to monitor
training and ensured that staff are adequately trained?
Will staff be tested?
Conversion
Communications
Data should be complete, accurate, and current before being
converted
Testing
Establish communication mechanisms for identifying and
addressing problems and concerns
Communicate regularly with various constituent groups
Preparation for Go-Live Date
Select date when patient volume is relatively low
Ensure sufficient staff are on hand
Set up mechanism for reporting and correcting problems and
issues
Review and effect process reengineering
Create an appropriate environment
Expectations are defined, met and managed
CFO – financial return
CMO – physician’s time/quality of care
Nursing staff – workload, patient satisfaction
IT staff – help desk calls
Do not underestimate user resistance
One of the biggest managerial challenges
Allocate sufficient resources
Provide adequate training
Manage unintended consequences
More work or new work
Workflow (workarounds)
System demands
Opportunity cost of time
Communication
Emotions
New kinds of errors
Upcoding
Juxtaposition errors
Power shifts
Dependence on the system (what happens when the
system is down?)
American College of Physicians and AmericanEHR Partners
The following are 10 mistakes that physicians commonly
make with EHRs:
Thinking a site visit to a practice that is using the same EHR
product isn't worth the effort.
2.
Signing an unvetted contract with a vendor.
3.
Neglecting to perform a workflow analysis before implementing
EHRs.
4.
Undertraining other physicians and staff on EHR use.
5.
Refusing to purchase a laboratory or device interface.
6.
Entering too much data into the EHR.
7.
Doing EHR-related work staffers should be doing.
8.
Using shortcuts and workarounds while using EHRs.
9.
Creating "shadow" paper documents and believing they are more
accurate than EHR information.
10. Accepting inefficiency as the new status quo.
1.
 0
0