Diuretics & Alpha-2 Agonists Cheat Sheet: MOA, Indications, Effects
advertisement

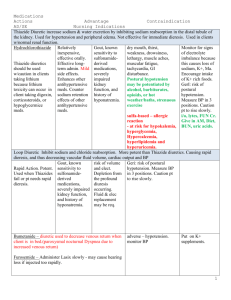
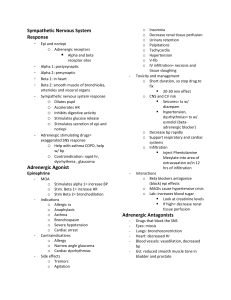
Diuretics (thiazide) Thiazide diuretics – hydrochlorothiazide, chlorothiazide, Indapamide, metolazone MOA: Inhibits reabsorption of Na, K, CI resulting in osmotic water loss. Relaxes arterioles (decreases afterload) Not effective for immediate diuresis Indication: HTN (First line), edema, HF, liver cirrhosis, kidney disease, lowers bp 2-4 weeks Contraindications: Drug allergy, hepatic coma, anuria, kidney failure Adverse effects: Electrolyte disturbance (decreases K, elevated Ca, lipids, glucose, uric acid), dizziness, GI disturbances, thrombocytopenia, pancreatitis, cholecystitis, headache, impotence, metabolic alkalosis, constipation Interaction: NSAIDS may decrease the antihypertensive effect Nursing consideration: Monitor VS, orthostatic hypotension, hypokalemia, taking supplements with rich K+ foods, I&O, weight, renal function Sparing diuretic- Spironolactone, triamterene MOA: Spironolactone acts primarily through competitive binding of receptors at the aldosterone-dependent sodium-potassium exchange site in the distal convoluted renal tubule. Spironolactone causes increased amounts of sodium and water to be excreted, while potassium is retained. Indication: HTN, edema for pt with HF, liver dysfunction Adverse/side effects: Hyperkalemia, hyperglycemia, hyperuricemia, hypotension, renal impairment, hypersensitivity, and gynecomastia increase risk for lithium toxicity Consideration: Monitor I&O(30ml) = report, caution with renal impairment, liver pts. Administer in the morning to avoid nocturia. Cause orthostatic changes. Avoid salt substitutes that have high levels of potassium Loop diuretics- Furosemide MOA: Loop diuretics inhibit absorption of sodium and chloride in the loop of henle and proximal and distal tubules, thus causing fluid loss, along with sodium, potassium, calcium, and magnesium losses. Loop diuretics are very potent diuretics and are used when a patient has an exacerbation of fluid overload. Indication: Edema, HTN(first line) , IV furosemide is used to urgently treat pulmonary edema, Considerations: Onset is 1-hour, peak effect within 1st or 2nd hour. Duration effect 6-8. Should be administered in the morning, evening doses should be avoided Asses: For dehydration electrolyte imbalance, hypotension, tachycardia, arrhythmias GI disturbances. Hypokalemia if used with digoxin (digoxin toxicity) Adverse/side effects: dry mouth, weakness, lethargy, drowsiness, restlessness, muscle pain or cramps, Alpha-2fatigue, agonisthypotension, – Clonidine,oliguria. ctapress MOA: Clonidine stimulates the alpha-adrenergic receptors, resulting in vasodilation and decreased blood pressure, thus decreasing peripheral resistance, increased blood flow to the kidneys, and decreased afterload. Stimulate alphas-2 adrenoceptors in the CNS(brain & spinal cord) SNS the part in the nervous system increases HR, BP, BR, & pupil size. Indication: HTN, ADHD, opioid dependence, alcohol addiction menopause Consideration: Monitor BP, PR, dosage is adjusted to pts BP because it can cause hypotension, bradycardia, sedation. Rebound hypertension if stopped abruptly Adverse effects: Hypotension, bradycardia, sedation, depression, orthostatic hypotension, constipation, dry mouth, impotence