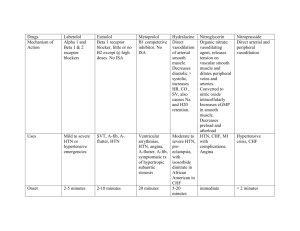
High Yield - - What organ systems/body parts do PNS dominate/affect? What about SNS? Left-sided HF VS right-sided HF Common side effects of loop diuretics, ACE inhibitors, CCBs, BBs What is endocarditis? Digoxin - MOA - Side effects - What to do before administering meds? - Relationship with potassium? Beta blockers and the different generations – which receptors they each affect? What do those receptors affect in the body? General anatomy of the heart (pericardium, veins, arteries, atrium, ventricle, SA node, valves, etc) Stable VS unstable anginas + STEMI VS NSTEMI, how to differentiate from each other? Angina medications and MOA Atherosclerosis pathophysiology + what are foam cells? Heparin toxicity antidote? Muscarinic agonist toxicity antidote? Muscarinic antagonist toxicity antidote? Warfarin toxicity antidote? Different classes of dysarrthymic medications Veins VS arteries function Diastolic failure VS systolic failure Warfarin and what is important to know – SE, labs, etc Statins and what side effects to look out for? What is Frank-Starling law? Anticoagulants MOA HDL = good, LDL = bad – relation with atherosclerosis Risk factors of HTN Why are beta blockers taken with nifidepine? Neurotransmitters of PNS and SNS Peripheral VS arterial vascular disease Valve issues (stenosis, prolapse, regurgitation) Know CO = HR x SV and BP = CO x SVR HTN medications Autonomic Nervous System PNS/Parasympathomimetic (cholinergic) PREDOMINATES Function ● Decrease HR SNS/Parasympatholytic (adrenergic) ● Increase HR ● ● Vasodilation + glands Increase GI activity (saliva, gastric, bowel, bladder) Constrict pupils Contract bronchi ● ● ● ● Vasoconstriction + glands, esp sweat Decrease GI activity Dilate pupils Dilate bronchi ● ACh ● ● ACh Epinephrine – all alpha/beta but no dopamine Norepinephrine – A1, A2, B1, but not B2, dopamine Dopamine – A1, B1, dopamine ● ● Neuro transmitters ● ● Receptors ● ● ● ● Baroreceptors NicotinicN - nerve NicotinicM - skeletal muscle contraction Muscarinic - to all PNS ● ● ● ● ● ● Pathway Long preganglionic → ACh → short postganglionic with Nicotinic receptors → ACh → target effector with Muscarinic receptors Baroreceptors Alpha1 – eyes, vessels, genitals Alpha2 – inhibition of transmitter release Beta1 – increase chronotropic/inotropic/dromotropic + release renin from kidney Beta2 – dilated bronchi, glycogenesis of liver and skeletal muscle, relax uterus Dopamine – dilation of kidney Short preganglionic → ACh → long postganglionic with Nicotinic receptors → NE → target effector with Alpha/Beta receptors Postganglionic → ACh → sweat gland with Muscrinic receptor Preganglionic → ACh → adrenal gland with Nicotinic receptor to release E What is Beers Criteria? → List of drugs that are potentially dangerous for >65 y/o as it increase risk for AE; especially ANTICHOLINERGIC DRUGS ANS Drugs (blue: PNS, red: SNS) Drug Class Prototype MOA + Use Side Effects Good to Know Muscarinic Agonist Bethanechol (Urecholine) Bind reversibly to muscarinic receptors to cause activation hypotension, bradycardia, diarrhea, salivation, abd cramps, bronchoconstriction, sweat Treatment for OD = atropine Xerostomia (dry mouth, tooth decay), blurred vision, photophobia, increased intraocular pressure, urinary retention, constipation, anhydrosis, Treatment for OD = physostigmine For urinary retention Muscarinic Antagonist Atropine Competitive blockage @ muscarinic receptors to prevention activation by ACh For prevent/treat bradycardia, decrease Caution for pts with asthma, hyperthyroidism, GI obstruction, urinary tract blockage secretion during preanesthesia, treat GI hypermotility, reverse OD for bethanechol Cholinestera se Inhibitors Oxybutynin (Ditropan) & Tolterodine (Detrol) For OAB: oxybutynin selective for M3 and tolerodine non-selective Neostigmine (prostigmin) Decreases activity of cholinesterase; leads to increased amounts of ACh available –stigmine Physostigmine Neuromuscul ar Blocking Agent Turbocurarine, vecuronium Myasthenia gravis (autoimmune destruction of ACh receptors); reverse atropine poisoning (physostigmine preferred) Nondepolarizing binding to nicotinicM receptor-ACh cannot bind, → paralysis of muscles by blocking action at the nicotinicM receptor site For surgery, intubation, mechanical ventilation Succinylcholin e Depolarizing binding to nicotinicM and initiate a contraction, then stays bound so the membrane remains depolarized → paralysis of muscles by blocking action at the nicotinicM receptor site constipation, tachycardia Same as muscarinic agonist > hypotension, bradycardia, diarrhea, salivation, abd cramps, bronchoconstriction, sweat positive charge CANNOT cross membrane resp arrest, hypotension Keep in mind: must be given thru IV, CANNOT pass thru BBB + placenta, DOES NOT alter pain perception + consciousness Specific to Succinylcholine: Malignant hyperthermia (increase in body temp due to hypercatabolic state); post-op muscle pain; hyperkalemia (due to promotion of release of K+ from tissues) no charge CAN cross membranes For surgery, intubation, mechanical ventilation Adrenergic Antagonist ALPHA Prazosin (Minipress) for HTN -sin Tamsulosin (Flomax) for BPH enlarged prostate Adrenergic Antagonist BETA Propranolol (Inderal): 1st gen, nonselective -lol Metoprolol HTN, BPH, Raynaud’s disease, pheochromocytoma Orthostatic hypotension, relfex tachycardia, congestion, ejaculation inhibition For heart and vessels: angina, HTN, MI, heart failure, dysrhythmia SE for B1: bradycardia/reduce CO/AV block/rebound excitation SE for B2: bronchoconstriction, glycogenolysis inhibition (Lopressor): 2nd gen, beta1 selective Carvedilol (Coreg): 3rd gen, B1, B2, A1 for vasodilation Adrenergic Agonists = -cholamines = directly stimulating adrenergic receptors + can promote NE release, inhibit NE reuptake, or inhibit NE inactivation Catecholamine = non-oral, no cross BBB, short ½ life Noncatecholamine = oral, cross BBB, long ½ life Receptor Use SE Alpha 1 Promotion of hemostasis, nasal decongestion, combined with/adjunct with local anesthesia, treatment of decreased BP, pupil dilation hypertension, necrosis, bradycardia Alpha 2: Clonidine (Catapress) for HTN, pain, ADHD by activating α2 receptors in the CNS; decreases sympathetic outflow to vessel and heart to decrease HR + BP drowsiness, xerostomia, rebound HTN, abuse potential/euphoria, teratogenic Alpha 2: Methyldopa HTN by convert methylnorepinephrine neurons + activate α2, only decrease BP Beta 1 treatment of cardiac arrest, heart failure/shock, AV block dysrhythmias, angina Beta 2 for asthma, delay preterm labor Hyperglycemia, tremor Dopamine treatment for shock/heart failure tachycardia/dysrhythmia, angina, renal damage Atherosclerosis: Thickening and hardening of vessel walls, caused by accumulation of lipid-laded macrophages within the arterial wall, leading to formation of a lesion = plaque, important to consider cholesterol level 1. Injury 2. Inflammation 3. adhesion m’c with macrophages - damage endothelium = free radicals 4. engulf oxidized LDL = fatty streak/foam cell = more free radicals 5. smooth muscle cell proliferation = fibrous plaque 6. plaque rupture = complicated plaque = ischemia or infarction Total cholesterol level = <100 ● LDL = < 100 ● HDL = > 60 ● TG = < 150 Metabolic syndrome = increases triglyceride levels in pts, often those who are inactive, smokers, alcoholic, genetic hx, high cholesterol diet; Cluster of conditions that increase the risk of heart disease, stroke, DM (has to meet 3 parameters) Anti-Hyperlipidemia (Statins & NFE) Drug Class Prototype MOA + Use Side Effects Good to Know Statins Atorvastatin (Lipitor), Rosuvastatin (Crestor), Simvastatin (Zocor) Inhibits enzyme critical in the cholesterol biosynthesis pathway = decreased cholesterol production ‒> liver to take up cholesterol from bloodstream = reduces LDL (MOST IMPORTANT) and triglycerides, increases HDL muscle pain, rhabdomyolysis SO LOOK FOR COKE COLA URINE (look out for muscle pain and coke urine, discontinue + report to provider immediately), liver damage, increased risk for diabetes (CI for pregnancy and muscle disorder) Given at night -statin Promote plaque stability, reduce inflammation at plaque site, slow progressing of coronary artery calcification, enhance vasodilation, reduced risk for thrombosis and platelet deosition, suppress produpction of thrombin Exercise to increase HDL Other antihyperl ipemics Niacin (nicotinic acid) Reduce LDL & triglycerides + increase HDL Flushing, GI upset Used in conjuncti on with statins No longer a recommendation since not as effective as statins and no evidence of CV risk reduction ONLY used when statins cannot be used Fibrates Reduce triglycerides, no effect on LDL FIBER REDUCE FAT Ezetimibe (Zetia) - bile acid EXCLUDE CHOLESTERO L GI upset, highly protein boundinteract with warfarin Inhibit dietary absorption/reabsorptio n of cholesterol in intestines - increase excretion in feces Anti-HTN (Red: diuretic, orange: sympatholytics, green: CCBs, blue: RAAS) due to excessive activation of RAAS Drug Class Prototype MOA + Use Side Effects Good to Know Thiazide diuretics Hydrochlorot hiazide block reabsorption of Na+ and Cl- at distal CT; not useful in severe renal impairment similar to loop diuretics but less severe and no ototoxicity first line for HTN, edema Loop Diuretic K+-sparing diuretics: Aldosterone antagonist Furosemide (Lasix) Spironolacto ne (Aldactone) Blocks reabsorption of Na+ and Cl- in the thick segment of ascending loop of henle. 20% of filtered sodium and chloride is reabsorbed here, so diuresis is profound-strongest diuretics require rapid or massive mobilization of fluid; should be avoided when other diuretics will suffice as it has more severe SE, for severe renal impairment hypokalemia, ototoxicity, hyponatremia, hypochloremia, dehydration, hypotension Blocks aldosterone @ distal nephron = retention of K+ and increased excretion of Na+; minimal diuretics hyperkalemia, similar to hormones (affect menstrual cycle, deepen voice, hirsutism) Drug interaction: combined with thiazide and loop diuretics, careful with agents that increase K+ levels hyperkalemia, GI upset careful with agents that increase K+ levels Eplerenone -one HTN + edema (used with loop or thiazide) heart failure Disrupt Na+ and K exchange @ distal nephron by inhibit mechanism; minimal diuretics Drug interactions: Digoxin (increased toxicity for those w/ hypokalemia), ototoxic drugs, potassium-sparing drugs (to counteract K+ wasting) Dose: LAst 6 hrs (Lasix), BID K+-sparing diuretics: Non-aldostero ne antagonist Triameterne (Dyrenium) Osmotic diuretics .. not important Mannitol (Osmoitrol) given thru IV, filtered at glomerulus, undergo minimal reabsorption + metabolism, pharmacologically inert Beta blocker Prototypes Propranolol (Inderal) decrease HR, CO, contractility bradycardia, hypotension, insomnia Alpha 1 blocker Prototype Prazosin (Minipress) prevent stimulation of A1 receptors = prevent vasoconstriction Orthostatic hypotension so not first line for HTN Alpha/Beta Blockers Carvedilol (Coreg) Blocks B1, B2, A1 for decrease HR, RR, and BP so bradycardia, hypotension = Alone or combined w/ other diuretics to treat HTN and edema Caution with diabetics, you can mask S&S of hypoglycemia and ability to raise blood glucose + less effect in blacks than whites Prototype CAUTION with resp disease heart block Central Active Alpha2 Agonist Prototype Clonidine (Catapress) A2 inhibit neurotransmitter release so it suppress sympathetic outflow from brain stem to heart and vessels = vasodilation and reduced CO dry mouth, sedation, rebound HTN, orthostatic hypotension Direct vasodilators Hydralazine (Apresoline) Dilates arterioles, given frequently for HTN crisis for HTN, angina, heart failure to decrease afterload (resistance) in arterioles and preload (stretch) in veins = decrease workload, CO, perfusion Minoxidil (Lonitan) Very potent, also dilates arterioles Topical: Rogaine for hair growth Nitrates (nitroglycerin e, isosorbide dinitrate) Dilates veins and coronary arteries expansion of blood volume by body attempt to restore BP, reflex tachycardia because baroreceptors sense drop and trigger SNS, orthostatic hypotension Dihydropyridin es Nifedipine (Procardia) For HTN and angina, selective calcium channels in arterioles to decreased BP and increase coronary perfusion, HR, contractility toxic dose can lead to non-selectivity + cardiac suppression, ankle edema, reflex tachycardia (combine with beta blocker to prevent this) Why would a beta blocker be given with a CCB?: to prevent reflex tachycardia Verapamil For HTN, arrhythmias, angina; block calcium channel in vascular smooth muscle + heart to cause negative chronotrope, inotrope, dromotrope, and vasodilation constipation, hypotension, can exerbate dysfunction with cardiac disease, caution with heart failure and hypotension because can AV block Drug/food interactions: Digoxin + beta-adrenergic blocker (cardiac suppression), grapefruit juice (decrease metabolism = toxicity = can lead to hypotension/cardio toxicity) Enalapril (Vasotex), Lisinopril (Zestril) reduce levels of angiotensin II and increase levels of bradykinin thru inhibition of ACE and kinase II, prevents cardiac remodeling/myocytes changes ACE: Angioedema (should not use med again), cough from bradykinin, elevated K+ (hyperkalemia), first-dose hypotension, vasodilation, fetal Drug interaction: diuretics (first-dose hypotension), antihypertensive agents, agents that increase K+ -pine Acts on arterioles for HTN Orphans Acts on arterioles + heart for HTN and dysrhythmias Angiotensin-C onvertng Enzyme Inhibitors (ACEIs) -pril HTN, heart failure, MI, Caution: pts with renal Angiotensin II Receptor Blockers (ARBs) Valsartan (Diovan) -sartan diabetic/nondiabetic nephropathy, prevent diabetic neuropathy, prevent MI/stroke/death injury, decrease remodeling and blood volume insufficiency given low dosage since its excreted by kidneys, pregnant women block action of angiotensin II at receptor; only for decrease cardiac morbidity and mortality Angioedema, fetal injury, similar to ACEIs but lower cough and hyperkalemia Drug interaction: antihypertensives HTN, heart failure, diabetic nephropathy, MI, stroke, diabetic retinopathy Caution: pts with renal insufficiency given low dosage since its excreted by kidneys, pregnant women Renin Inhibitor Aliskiren (Tekturna, Rasilez) bind to renin to inhibit production of angiotensin I, only for HTN less cough + angioedema but fetal injury Caution with pregnant women Aldosterone Antagonists Eplerenone (Inspra) block aldosterone receptor hyperkalemia Drug interactions: Drugs that increase K+ HTN, heart failure Common Dysrhythmias Atrial fibrillation most common dysrhythmia caused by multiple atrial impulses firing randomly = stroke, clot; treated by cardioversion, drugs to control rate/rhythm (beta blocker/CCB or antiarrhythmics, anticoagulant, ablation Atrial flutter fast atrial rate with a fixed or variable ventricular rate; similar treatment as Afib Supraventric ular tachycardia (SVT) AV node affected; HR of 150-250 bpm = increase CO but can get too fast to have enough blood filled up in heart eventually decrease CO; treated with Valsalva maneuver/bearing down to slow rate down when rapid or dump baby head in ice water Ventricular tachycardia (VT) 150-250 bpm; emergency need cardioversion ASAP, Amiodarone IV, defibrillator implant Ventricular fibrillation (Vfib) No meaningful CO = emergency with async discharge of ventricules, localized twitching around ventricles, will eventually stop pumping; treatment with defibrillation, ICD placement, Amiodarone Premature ventricular contractions (PVCs) common like from caffeine but can lead to decrease of CO; ventricle fires prematurely without atrial stimulation Torsades de Pointes tachydysrhythmia, form of VT, caused by prolonged QT interval as SE of drug, fatal if not treated by cardioversion IV Mg+ Atrioventricu lar (AV) block impaired transmission from atria to ventricles has 3 degrees 1. First degree: P wave normal but QRS complex is late but regular 2. 3. 4. Second degree Type I: P wave normal but QRS complex gradually is late until it is gone Second degree Type II: P wave normal but QRS complex sometimes does not occur and sometimes occurs but when it does its regular – requires pacemaker Third degree: P wave and QRS complex no longer in sync – requires pacemaker Antidysrhythmic (SBPC, O) Drug Class Prototype MOA + Use Side Effects Good to Know Class I: Sodium Channel Blockers Lidocaine short-term treatment of ventricular dysrhythmias by slow atrial/ventricular conduction and accelerate repolarization drowsiness, confusion rapidly metabolized by liver Class II: Betablockers Propranolol non-selective beta blocker to slow ventricular rate & decrease contractility hypotension, AV block, bronchospasm Caution with pt with resp issue Class III: Potassium Channel Blockers Amiodarone HIGHLY effective short-term against atrial + ventricular dysrhythmias by delay repolarization has SERIOUS toxicity (lung damage, impaired visual, thyroid/liver toxic, teratogenic, photosensitivity) Class IV: CCBs Verapamil & Diltiazem cause negative chronotrope, inotrope, dromotrope, and vasodilation constipation, hypotension, can exerbate dysfunction with cardiac disease, caution with heart failure and hypotension because can AV block Drug/food interactions: Digoxin + beta-adrenergic blocker (cardiac suppression), grapefruit juice Others Adenosine & Digoxin slow conduction thru AV node dysrhythmias risk for digoxin and increase risk for it with hypokalemia Adenosine has rapid half-life + terminate SVT Digoxin leads to positive inotrope, negative chronotrope and dromotrope + suppress renin and SNS Must count HR before admin digoxin Left VS Right HF Left sided HF More common, can lead to right sided Forward effects = decreased tissue perfusion + RAAS activation Backward effects = pulmonary congestion symptoms: dyspnea on exertion, orthopnea, cough, paroxysmal nocturnal dyspnea, cyanosis, crackles at base of lungs Right Most likely caused by left sided HF sided HF Forward effects = decreased tissue perfusion + RAAS activation Backward effects = systemic congestion symptoms: hepatomegaly, ascites (fluid in abdomen), splenomegaly, anorexia, subcutaneous edema, jugular vein distention Anti-Heart Failure (DRAASBS) Drug Class Prototype MOA Good to Know Diuretics thiazide, loop, spironolactone, caution with k-spring diuretic decrease venous pressure, afterload, pulmonary/peripheral edema, cardiac dilation decrease symptoms BUT NOT survival time Agents that inhibit RAAS: ACE inhibitors —pril suppress production of angiotensin II improve symptoms and survival time Agents that inhibit RAAS: Aldosterone antagonist spirolactone/epler enone blocks aldosterone receptors improve symptoms and survival time Agents that inhibit RAAS: Arnis Sacubitril + Valsartan inhibit neprilysin to vasodilation and reduce volume SE: similar to ARBs and dementia Beta blockers Propranolol, Metoprolol, Carvedilol blocks beta receptors depending on generation to decrease HR and BP start with LOW does because can suppress cardiac function with SE of bradycardia, hypotension, another HF SGLT-2 inhibtors Canagliflozin (Invokana) inhibit SGLT-2 in kidney to inhibit RAAS, promote excretion, reduce SNS, reduce preload/afterload SE: vaginal fungal infection, UTIs SE: hyperkalemia Anginas Acute Coronary Syndrome = complete occlusion of coronary artery by thrombosis Angina pain beneath sternum and radiate to left jaw, shoulder, arm because decrease O2 flow to heart caused by atherosclerosis treated with BB, nitrates, CCB Chronic stable angina (exertional angina) caused by coronary artery disease (CAD) + atherosclerosis = decrease blood supply, triggered by exertion, emotional stress, cold, but no pain at rest; treated by increase supply/decrease demand, stop smoking, exercise, treat hyperlipidemia Variant angina (Prinzmetal’s) rare, caused by coronary artery spasm from cold, stress, substance use Unstable angina EMERGENCY! Unstable plaque! Unpredictable pain! Acute coronary syndrome, may have normal, undetermined, or abnormal EKG (but NOT ST-segment elevation) + no troponin rise STEMI (ST-Elevation persistent ST-segment elevation indicating blockage of coronary artery and imbalance of O2 supply and demand = cell death within 20 MONA (morphine, O2, nitroglycerine, aspirin CHEWED) Myocardial Infarction) min if no intervention crushing radiating pain, last 20-30 min, can look different for women like crushing, stabbing, cold sweat, dizziness, nausea, fatigue, SOB, EKG change, elevated serum cardiac marker NSTEMI (Non-ST-Elevati on Myocardial Infarction) may have normal, undetermined, or abnormal EKG (but NOT ST-segment elevation) + Troponin rise Antianginals (NBC) Drug Class Prototype MOA + Use Side Effects Good to Know Nitrates NTG (Nitroglycerine), Imdur (Isosorbide) decrease O2 demand/preload by vasodilation in VENOUS system primarily and CORONARY ARTERIES hypotension, tachycardia do not abruptly stop med Beta blockers Metoprolol (Lopressor) + Propranolol decrease O2 demand by decrease HR and contractility Calcium-Channel blocker Verapamil (ORPHAN) + Enalapril decrease O2 demand by vasodilation ORPHAN can decrease afterload, preload, contractility (decrease SV) Anticoagulants (HEF + WDR)= prevent thrombosis in veins and atria by prevent formation of fibrin Drug Class Prototype MOA + Use Good to Know Activating Antithrombin Heparin (IV) (unfractionated binds antithrombin, increase ability to inactivate factor Xa and thrombin; HIGHEST RISK for HIT (Look for PLT counts) to prevent DVT or Afib aPTT= partial thrombosis time = to measure contact activation and common pathways for heparin use with Normal as < 40 sec TR = 60-80 sec we want to 2x their normal = TR (40*2 = 80) BLEEDING + BRUISING RISK rapid onset, enhancing activity of antithrombin and inactivate thrombin and factor Xa to decrease thrombin BUT differ in equal effects on thrombin and If TR too high = hemorrhage Treatment for OD = protamine sulfate Enoxaparin (SubQ) (low-molecularweight (LMW) inactivate Xa, and thrombin to small extent; low risk for HIT factor Xa Vitamin K Antagonists heparin) Fondaparinux (SubQ) only inactivate Xa; no risk for HIT Warfarin (PO) (Coumadin) suppress coagulation by decrease production of vit K-dependent clotting factors to prevent DVT and PE for pts with Afib or cardiac valve replacement; dosing highly variable because of genetics and dietary vit K intake (kept steady) + delayed onset Treatment for OD = vitamin K (phytonadione) If INR too high = vitamin K + fresh frozen plasma If INR too low = continue Caution: drugs that promote bleed, albumin bound, inhibit metabolizing enzymes, increase risk for peptic ulcer formation + pts with liver disease, alcohol, pregnant, vit K deficiency Educate: frequent INR monitoring, keep vit K intake consistent, BLEEDING + BRUISING RISK ensure all prescribers know warfarin use, avoid OTC pain relievers, S&S of hemorrhage, discuss contraception with child bearing age Normal INR = <1.1 (0.8-1.1) (we want to 3x more than normal = TR) TR: 2.0-3.0 or 2.5-3.5 (for higher risk to develop clot) If TR too high = bleeding Direct Thrombin Inhibitors Dabigatran (PO) (Pradaxa) bind to thrombin when free and within clots Direct Factor Xa Inhibitors Rivaroxaban (PO) bind to active center of Xa, which inhibit activation of thrombin Compared to warfarin – Advantages: rapid onset, no monitoring needed, few drug/food interaction, same does for all pts, low risk of bleed Disadvantages: short duration of action (so need to take at prescribed time for sure), no antidote for OD, limited experience, not approved for mechanical valve replacement so still must use warfarin Antiplatelets (ACA) = prevent thrombosis in arteries and platelet aggregation Prototype MOA + Use Side Effects Good to Know Aspirin (COX inhibitor) irreversible inhibition of COX leading to decreased platelet aggregation by decrease TXA2 (thromoxane A2) (for vasoconstriction) to prevent stroke and MI bleeds do not give to anyone under 18 yo Clopidogrel (P2Y12 ADP receptor antagonist) irreversible blockage of P2Y12 ADP receptors leading to decrease platelet aggregation to use as secondary prevention for atherosclerotic events for pts with angina, MI, coronary stents bleed, risk for thrombotic thrombocytop enic purpura usually used with ASA Abciximab (GP IIb/IIIa receptor antagonist) super aspirins, most effective, reversible blockage at receptor = no platelet aggregation; used short term for those undergo cardiac angiography or acute coronary syndrome has 2x risk for bleed Thrombolytics Alteplase (tPA/Activase) = catalyze conversion of plasminogen to plasmin to digest fibrin clots of new thrombi that have already formed which is used acutely for MI, PE, stroke; SERIOUS RISK FOR BLEEDING! Only use after ruling out potential risks What is the biggest risk factor of thrombolytic medications?: hemorrhage when giving thrombolytic and another drug that interfere with clotting; educate pt S&S of increased HR and decreased BP, petichiae/hematoma/excessive bruise, black/red stool, discolored urine, pain and location