Cholangiocarcinoma
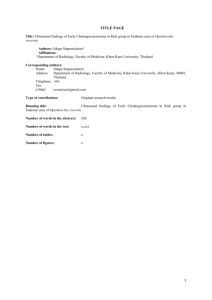
Clin Liver Dis 12 (2008) 131–150 Cholangiocarcinoma Boris R.A. Blechacz, MD, PhD, Gregory J. Gores, MD* Division of Gastroenterology and Hepatology, Miles and Shirley Fiterman Center for Digestive Diseases, Mayo Clinic College of Medicine, 200 First Street SW, Rochester, MN 55905, USA Cholangiocarcinoma is a neoplasm originating from the intra- or extrahepatic bile duct epithelium [1]. Historically, it was first described by Durand-Fardel in 1840 [2]. It was not until 1911 that primary liver neoplasias were distinguished based on their cellular origin into ‘‘hepatomas’’ and ‘‘cholangiomas’’ or ‘‘hepatocellular carcinomas’’ and ‘‘cholangiocarcinomas’’ [3,4]. Hilar cholangiocarcinoma as a specific entity was first described by Klatskin in 1965, and cholangiocarcinomas arising at this anatomic site are often referred to as Klatskin tumors [5]. Cholangiocarcinomas may be considered rare tumors comprising only 3% of gastrointestinal tumors; however, they are the second most common primary hepatic tumors, and their incidence is increasing. Surgical resection or liver transplantation is the only potentially curative therapeutic option. Photodynamic therapy can be palliative for unresectable but localized cancer. In the future, targeted therapies have the potential to extend life for patients with advanced metastatic disease. Classification Cholangiocarcinomas are classified according to their anatomic location as intrahepatic and extrahepatic (Fig. 1A). The extrahepatic type including cancers involving the confluence of the right and left hepatic ducts accounts for 80% to 90% and the intrahepatic type for 5% to 10% of all cholangiocarcinomas. The anatomic margins for distinguishing intra- and extrahepatic cholangiocarcinomas are the second order bile ducts. Extrahepatic cholangiocarcinomas can further be subdivided according to the Bismuth classification into types I to IV (type I, tumor involves the common hepatic * Corresponding author. E-mail address: gores.gregory@mayo.edu (G.J. Gores). 1089-3261/08/$ - see front matter Ó 2008 Elsevier Inc. All rights reserved. doi:10.1016/j.cld.2007.11.003 liver.theclinics.com 132 BLECHACZ & GORES Fig. 1. Anatomic classification of cholangiocarcinoma. (A) The anatomic classification of cholangiocarcinoma in intrahepatic, hilar, and distal ductal cholangiocarcinoma is depicted. Extrahepatic cholangiocarcinoma includes hilar and distal ductal cancers. (B) The Bismuth classification of hilar cholangiocarcinoma into type I to IV stages is illustrated. Yellow areas represent tumor and green areas normal bile duct. (Modified from de Groen PC, Gores GJ, LaRusso NF, et al. Biliary tract cancers. N Engl J Med 1999;341:1369; with permission. Copyright Ó 1999, Massachusetts Medical Society.) duct distal to the biliary confluence; type II, tumor involves the biliary confluence; type IIIa, tumor involves the biliary confluence plus the right hepatic duct; type IIIb, tumor involves the biliary confluence plus the left hepatic duct; type IV, multifocal or tumor involves the confluence and both the right and left hepatic ducts) (Fig. 1B). Further subclassification of extra- and intrahepatic cholangiocarcinomas has been defined based on their macroscopic appearance. Extrahepatic cholangiocarcinomas display a sclerosing, nodular, and papillary phenotype of which the sclerosing or periductal infiltrating type is the most common. It is characterized by annular bile duct thickening due to infiltration and fibrosis of periductal tissues. Intrahepatic cholangiocarcinomas are subclassified into mass forming, periductal infiltrating, mass forming plus periductal infiltrating, and intraductal; this classification has been shown to correlate with prognosis [6]. Histologically, adenocarcinoma is the most common pathologic form, comprising 90% of cases. Other histologic types include papillary adenocarcinoma, intestinal type adenocarcinoma, clear cell adenocarcinoma, signet-ring cell carcinoma, adenosquamous carcinoma, squamous cell carcinoma, and oat cell carcinoma [7]. Epidemiology Cholangiocarcinoma accounts for less than 2% of all human malignancies [8]; however, it is the second most common primary hepatic malignancy CHOLANGIOCARCINOMA 133 after hepatocellular carcinoma, accounting for 10% to 15% of primary hepatic malignancies. Its prevalence is geographically heterogeneous, with the highest rates in Asia, especially Southeast Asia [9]. In Western Europe and the Unites States, the incidence and mortality have increased over the last 4 decades. Incidence In the United States, the age-adjusted incidence of intrahepatic cholangiocarcinoma has increased by 165% from 0.32/100,000 in 1975 to 1979 to 0.85/100,000 in 1995 to 1999; between 1985 and 1993, the incidence rate increased dramatically [10,11]. An increasing incidence has also been observed in other regions around the globe. Estimated incidence rates in Crete, Greece, have increased from 0.998/100,000 in 1992 to 1994 to 3.327/100,000 in 1998 to 2000 [12]. In Japan, the frequency of intrahepatic cholangiocarcinoma diagnosed at autopsy increased from 0.31% to 0.58% between 1976 to 1977 and 1996 to 1997 [13]. Although it was reported that the incidence rates for extrahepatic cholangiocarcinoma decreased by 14% from 1.08/100,000 to 0.82/100,000 in 1998 [9], these numbers are not accurate because the majority of the epidemiologic studies misclassified hilar cholangiocarcinoma as intrahepatic cholangiocarcinoma. This systematic mistake was due to a misclassification of these tumors in the ICD-O coding system derived data form for the Surveillance, Epidemiology, and End Results program. Welzel and colleagues [14] addressed this issue and reevaluated incidence rates of intra- and extrahepatic cholangiocarcinoma after correction of this misclassification. They reported that 91% of hilar tumors were misclassified as intrahepatic, resulting in an overestimation of intrahepatic cholangiocarcinoma by 13% and an underestimation of extrahepatic cholangiocarcinoma by 15%. Nevertheless, reevaluation of incidence rates in the United States between 1978 and 2000 still identified a significant increase of intrahepatic cholangiocarcinomas, while no significant change in the incidence of extrahepatic cholangiocarcinomas was noted. The cause of the global increase in the incidence rates for intrahepatic cholangiocarcinomas is unclear. The etiopathogenesis for most patients with cholangiocarcinoma remains obscure. Gender, age, and other factors Worldwide, the average age at presentation is 50 years. In Western nations, most instances of cholangiocarcinomas are diagnosed at 65 years of age or older and only rarely before the age of 40 years [9]. In the general population, 52% to 54% of cholangiocarcinomas are observed in male patients; however, mortality data show a higher estimated annual percentage change (EAPC) in females when compared with males, with an EAPC of 6.9 1.5 for males and 5.1 1.0 for females [15]. Differences in the prevalence of cholangiocarcinoma have been reported globally as well as 134 BLECHACZ & GORES between different racial and ethnic groups [16]. Globally, the highest prevalence has been described in Southeast Asia. Within the United States, a comparison of the 10-year prevalence between 1990 and 2000 showed a high age-adjusted prevalence of 1.22/100,000 for intrahepatic cholangiocarcinomas in Hispanics. Interestingly, within this group, the prevalence was higher in females. The lowest prevalence was described in African Americans, with a prevalence of 0.5/100,000 for males and 0.17/100,000 for females. Asian Pacific Islanders and Caucasians had prevalence rates ranging between these two groups. Etiology In most patients, cholangiocarcinoma has developed without an identifiable etiology; however, certain risk factors for cholangiocarcinoma have been established. One of the most commonly recognized risk factors is primary sclerosing cholangitis. The prevalence of cholangiocarcinoma in patients who have primary sclerosing cholangitis is 5% to 15% [17]. The annual incidence rate for cholangiocarcinoma in the setting of primary sclerosing cholangitis is 0.6% to 1.5% [17,18]. In most patients, cholangiocarcinomas are diagnosed within the first 2.5 years after the diagnosis of primary sclerosing cholangitis, and prospective studies have reported that 37% of patients developing cholangiocarcinoma will do so within the first year following the diagnosis of primary sclerosing cholangitis [17,18]. Hepatobiliary flukes are another risk factor for cholangiocarcinomas. A strong association has been shown with the species Opisthorchis viverrini and Clonorchis sinensis and the development of cholangiocarcinoma [19]. Especially in East Asia, one of the regions with the highest prevalence of cholangiocarcinoma, these flukes are endemic. They are ingested with undercooked fish and infest the bile ducts and occasionally the gallbladder. Increased incidence rates of cholangiocarcinomas in liver fluke–infected patients have been shown in several case-control studies, and the correlation has been confirmed in animal models [20–22]. Another risk factor for cholangiocarcinoma that is more common in Asian than Western countries is hepatolithiasis. Cholangiocarcinoma incidence rates of 10% in patients who have hepatolithiasis have been reported [23–25]. Additional risk factors for cholangiocarcinoma include Caroli’s syndrome, congenital hepatic fibrosis, and choledochal cysts, all of which carry a 10% to 15% risk for cholangiocarcinoma [26–28]. Pathophysiology The previously described etiologic factors create an environment of chronic inflammation predisposing biliary epithelium to malignant transformation. Chronic inflammation and cholestasis have been linked to carcinogenesis in cholangiocarcinoma. Together, both conditions can promote the CHOLANGIOCARCINOMA 135 four major cancer phenotypes: (1) autonomous cell proliferation; (2) invasion/metastases; (3) escape from senescence; and (4) evasion of cell death [29,30]. A variety of molecular alterations have been described in these carcinogenic phenotypes [29–32]. Chronic inflammation results in the expression of multiple cytokines and chemokines by cholangiocytes and inflammatory cells [29,33]. One of the key cytokines in cholangiocarcinoma carcinogenesis is interleukin-6 (IL-6) [29,34–36]. It mediates cholangiocarcinoma cell survival by up-regulation of the potent anti-apoptotic protein Mcl-1 [37–39]. Cellular Mcl-1 protein levels are further enhanced by bile acid–induced epidermal-derived growth factor receptor activation [40,41]. IL-6 mediates escape from senescence by the induction of telomerase [42]. Further damage is mediated by cytokine induction of inducible nitric oxide synthase (iNOS) in inflammatory cells and epithelial bile duct cells. Increased iNOS expression has been observed in cholangiocytes in primary sclerosing cholangitis and cholangiocarcinoma, and elevated serum nitrate concentrations have been identified in patients with liver fluke infection [43]. Increased expression of iNOS results in increased generation of nitric oxide which inhibits DNA repair proteins and apoptosis by nitrosylation of base excision repair enzymes (eg, OGG1) and caspase-9, respectively [43,44]. Several additional molecular alterations have been reported, resulting in the activation of growth factors and proto-oncogenes as well as inhibition of tumor suppressor genes [29,45]. In addition, alterations in genes coding for adhesion molecules and anti-angiogenic factors have been described, mediating tumor invasion and spread [29,45]. Diagnosis The diagnosis and staging of cholangiocarcinoma require a multimodality approach involving laboratory, radiologic, endoscopic, and pathologic analysis. Despite the variety of techniques used, determining the extent of disease still poses a challenge and is often underestimated. The diagnostic modalities described in the following sections, in combination and in the appropriate clinical context, are useful to help achieve diagnostic accuracy. Clinical, endoscopic, and radiologic diagnosis Extrahepatic and intrahepatic cholangiocarcinomas present with distinct clinical signs that translate into their clinical and radiologic presentation. Clinical presentation Most cholangiocarcinomas remain clinically silent until the advanced stages. Once patients become symptomatic, the clinical presentation is dominated by the anatomic location of the tumor. The predominant clinical feature of extrahepatic cholangiocarcinoma is biliary obstruction resulting in painless jaundice, with which 90% of patients initially present [7,46]. 136 BLECHACZ & GORES Intrahepatic cholangiocarcinoma presents in most cases as an intrahepatic mass causing right upper abdominal quadrant pain and other tumor-related symptoms such as cachexia and malaise. Approximately 10% of patients present with cholangitis [7]. Ultrasonography Ultrasound is one of the first-line imaging modalities chosen for the evaluation of cholestasis or liver dysfunction. For the identification of cholangiocarcinoma, it has only limited value [46]. Findings include unspecific signs such as intrahepatic bile duct dilatation with an abrupt change in bile duct caliber in cases of extrahepatic and hilar cholangiocarcinoma. Extrahepatic cholangiocarcinoma tumor masses are seldom identified by ultrasound [47,48]. Intrahepatic cholangiocarcinomas are identified as a nonspecific intrahepatic mass. Doppler ultrasonography can be helpful for detecting compression and tumor encasement of the portal vein or hepatic artery. Overall, the sensitivity and specificity of ultrasound is poor in the diagnosis of cholangiocarcinoma, and staging generally relies on other imaging modalities [49,50]. Computed tomography CT can be helpful in the staging, preoperative planning, and evaluation of vascular encasement. Intrahepatic cholangiocarcinoma can present as an irregular shaped mass with delayed and peripheral enhancement during the portovenous phase of the study. Hilar and extrahepatic cholangiocarcinomas may present as a mass, ductal thickening, or nonunion of the right and left hepatic duct with or without ductal thickening. As is true for ultrasound, hilar tumor masses are difficult to visualize by CT. Intrahepatic bile duct dilatation in a single small lobe and hypertrophy of the contralateral lobe signify the atrophy-hypertrophy complex seen with lobar duct obstruction frequently plus ipsilateral portal vein encasement [51]. Evaluation of intraductal spread and detection of lymph node and peritoneal metastases by CT are also suboptimal. The sensitivity for N2 metastases detection by CT has been reported to be 50% and the overall accuracy in the assessment of resectability 60% to 75%. Magnetic resonance imaging and magnetic resonance cholangiopancreatography At present, MRI with magnetic resonance cholangiopancreatography (MRCP) is the best available imaging modality for cholangiocarcinoma [46]. It provides information regarding tumor extent, biliary and hepatic parenchymal anatomy, and intrahepatic metastases. Cholangiocarcinoma is characterized on MRI as a hypointense structure on T1-weighted images and a hyperintense structure on T2-weighted images (Fig. 2). Central hypointensity on T2-weighted MRI corresponds to central fibrosis. In dynamic contrast-enhanced MRI, cholangiocarcinoma is usually recognized CHOLANGIOCARCINOMA 137 Fig. 2. MRI study of hilar cholangiocarcinoma. Gadolinium-enhanced MRI analysis of the liver with ferumoxide in a patient with hilar cholangiocarcinoma Bismuth type III-IV. (A) T2-weighted MRI images. There is a hyperattenuating mass at the confluence of the right and left biliary ducts and dilatation of the right and left intrahepatic bile duct system (white arrow). (B) MRCP of the same patient demonstrating a dominant stricture in the area of the biliary confluence and dilatation of the intrahepatic left and right biliary system (white arrow). by delayed moderate peripheral enhancement. Involved bile ducts are identified by irregular ductal narrowing with proximal dilatation [52]. The imaging quality of cholangiocarcinoma can be enhanced significantly by the use of ferumoxide, a routine adjunct for MRI at the authors’ center [53,54]. Cholangiography Cholangiography is one of the most important tests in the evaluation of cholangiocarcinoma [46,55]. It allows early diagnosis and can help evaluate the proximal and distal intraductal extent of the tumor. Cholangiography can be done by performing endoscopic retrograde cholangiopancreatography (ERCP), MRCP, or transcutaneous cholangiography (PTC). MRCP has the advantage of being noninvasive and the possibility of obtaining additional information about other intra- and extrahepatic anatomic structures, whereas ERCP and PTC have the advantage of allowing bile duct sampling for diagnostic analysis as well as the possibility of relieving biliary obstruction by the insertion of stents. The choice of the imaging modality depends also on location of the tumor; distal extrahepatic cholangiocarcinoma is optimally evaluated by ERCP. At times, hilar cholangiocarcinomas can only be stented by the percutaneous route. Endosonography with fine-needle aspiration Endosonography allows further evaluation of regional lymph nodes and the biliary tree, thereby obtaining further information for staging. In addition, it allows ultrasound-guided, fine-needle aspiration of lymph node tissue for pathologic analysis. The use of this technique for obtaining tissue 138 BLECHACZ & GORES from a suspicious hilar lesion is not advised because it can result in tumor spread with peritoneal tumor seeding [45]. Positron emission tomography As seen in other malignancies, cholangiocarcinoma cells may accumulate [18F]-2-deoxy-glucose (FDG), thereby depicting cholangiocarcinomas as ‘‘hot spots’’ [46]. Mucinous cholangiocarcinomas are an exception because they have been shown not to accumulate FDG [49]. In a recent study with a limited number of patients, a sensitivity of 92% and specificity of 93% for detecting the primary lesion were described [56]; however, the sensitivity for detecting distant metastases and regional lymph node metastases was only 67% and 13%, respectively. In addition, false-positive results can be generated in the setting of chronic inflammation, and negative results do not exclude malignancy [57]. In a larger number of patients, CT/PET scanning of cholangiocarcinoma was associated with a lower sensitivity, especially for extrahepatic cancer [58]. Other imaging modalities Other imaging techniques include intraductal ultrasound, endoscopic/ percutaneous flexible cholangioscopy, and radiolabeled imaging. These techniques are not part of the routinely performed diagnostic work-up. Laboratory analysis Laboratory-based analysis for the diagnosis of cholangiocarcinoma is restricted to serum, bile, bile duct brush cytology, and lymph node pathology. Percutaneous biopsy of the primary tumor is not advised due to an increased risk of tumor spread. Tumor markers The most studied serum tumor markers are the carbohydrate antigen 19-9 (CA 19-9), carcinoembryonic antigen (CEA), and carbohydrate antigen 125 (CA-125). CEA and CA-125 are unspecific and can be elevated in the setting of other gastrointestinal or gynecologic malignancies or other bile duct pathology such as cholangitis and hepatolithiasis [59]. CA 19-9 was first described in 1979 and is currently the most commonly used tumor marker for cholangiocarcinoma [60,61]. Nevertheless, CA 19-9 has certain limitations which need to be considered when using it as a tumor marker. First, CA 19-9 serum concentrations depend on the Lewis phenotype. As many as 10% of the population have been found to be Lewis negative, resulting in undetectable CA 19-9 levels [62,63]. Second, CA 19-9 can also be elevated in other gastrointestinal or gynecologic malignancies and in the setting of bacterial cholangitis [64–66]. The use of a CA 19-9 level cutoff value of greater than129 U/mL was shown to result in a sensitivity of 78.6% and a specificity of 98.5%, and a change in CA 19-9 of 67.3 U/mL over time provided a sensitivity of 90% and specificity of 98% [67]. CHOLANGIOCARCINOMA 139 Cytologic analysis A tissue diagnosis is usually obtained by brush cytology or bile duct biopsy during ERCP. In the setting of primary sclerosing cholangitis, interpretation of cytology can be challenging due to reactive changes by inflammation [68]. The sensitivity and specificity for conventional brush cytology are reported to be 37% to 63% and 89% to 100%, respectively [69–71]. The limitations of conventional cytology relate to the typically desmoplastic structure of this cancer and limited access to the biliary system. To improve diagnostic accuracy for the diagnosis of cholangiocarcinoma, new advanced cytologic techniques have been introduced, including digital image analysis and fluorescence in situ hybridization (FISH). Both techniques identify aneuploidy. In digital image analysis, DNA content relative to normal ploidy is quantitated. A comparison of digital image analysis with cytology in patients with suspicious biliary strictures demonstrated a sensitivity of 39.3% with digital image analysis compared with 17.9% by cytology. The specificity was 77.3% with digital image analysis compared with 97.7% with cytology [72]. Evaluation of digital image analysis in patients who had primary sclerosing cholangitis, 20% of whom had cholangiocarcinomas, demonstrated a sensitivity and specificity of 43% and 87%, respectively. In patients who had primary sclerosing cholangitis with negative cytology, a sensitivity and specificity of 14% and 88% were described [73]. FISH allows the detection of chromosomal amplifications by fluorescence and is interpreted as positive if five or more cells display gains of two or more chromosomes (polysomy) [73]. In patients who had primary sclerosing cholangitis, polysomy detected by FISH had a sensitivity of 47%, a specificity of 100%, a positive predictive value of 100%, and a negative predictive value of 88% in the detection of cholangiocarcinomas. In the setting of neither positive nor suspicious cytology, the sensitivity was 20% and the specificity 100%; the positive predictive value was reported to be 100% and the negative predictive value 88% [74]. FISH remarkably increases the yield of brush cytology for the diagnosis of cholangiocarcinoma without compromising specificity. Therapy Surgery Resection Surgical resection with curative intent is the treatment of choice for extrahepatic cholangiocarcinoma. Although the rate of resectability has been reported to be as high as 65%, curative resection or margin-free resection (R0) rates are less than 50% [75]. Criteria for unresectability of cholangiocarcinomas include bilateral involvement of the hepatic ducts to the level of the secondary biliary radicals, atrophy of one liver lobe with encasement of the contralateral portal vein branch, or atrophy of one liver lobe with 140 BLECHACZ & GORES contralateral secondary biliary radical involvement [76,77]. Bilateral portal vein branch encasement or involvement of the major portal vein is also a classic contraindication to surgical resection. Likewise, bilateral hepatic artery encasement would be a contraindication. Intrahepatic metastases are associated with such a poor outcome that most surgeons consider these patients unresectable. Lymph node involvement is more controversial. The outcome has not been reported to be influenced by local lymph node involvement [78]; therefore, many surgeons will pursue resection despite local lymph node metastases. Distant lymph node metastases are a contraindication to surgery. Comorbidities including significant liver disease, cirrhosis, and cardiovascular or other systemic diseases as well as the patient’s performance status have to be taken into consideration in the decision to proceed with surgery. Solitary intrahepatic cholangiocarcinomas are resected by hepatic lobectomy or segmentectomy. This strategy has reported to achieve 5-year survival rates of 23% to 63% [79–81]. With R0 resection, overall 5-year survival rates of 30% to 41% for hilar tumors, 31% to 63% for intrahepatic tumors, and 27% to 37% for extrahepatic cholangiocarcinomas have been reported [78,81–85]. Mortality rates of resection are 5% to 10% in major referral centers and mostly due to infections; liver failure is unusual as a cause for postoperative mortality [78]. The perioperative morbidity rate is between 31% and 85% [86–88]. The goal of neoadjuvant treatment options is to increase resectability rates and decrease recurrence rates after resection. Neoadjuvant strategies include chemotherapy, radiation, combined radiochemotherapy, and photodynamic therapy. Studies evaluating the treatment effects have demonstrated only limited effects, have been nonrandomized, have been conducted in only limited numbers of patients, and report only short-term follow-up [89,90]. Currently, no adjuvant therapy can be recommended. Preoperative portal vein embolization before extended complex hepatectomy with the goal of decreasing postoperative liver dysfunction was first described by Makuuchi and colleagues [91]. Liver resection is restricted to a postsurgical remnant liver volume of 25% to 30% [92]. The rationale behind portal vein embolization is a compensatory hypertrophy of the nonembolized hepatic segments, thereby allowing extended hepatectomy with minimal postoperative liver dysfunction. Increased resectability after portal vein embolization was shown in a subset of patients who otherwise would have been marginal candidates for resection due to low remnant liver volumes [93]. A recent study in 150 patients undergoing extended hepatectomy for cholangiocarcinoma failed to show a significant difference in 5-year survival [94]. Transplantation Initial results with liver transplantation for extrahepatic cholangiocarcinomas were disappointing, with 5-year survival rates of 23% to 26% and recurrence rates of 51% to 59% [95–97]. Based on the observed outcomes, liver transplantation was discouraged as a therapeutic option for extrahepatic CHOLANGIOCARCINOMA 141 cholangiocarcinomas. Promising results were achieved with a new neoadjuvant strategy including external beam radiation concomitant with fluorouracil (5-FU) followed by brachytherapy and then venous infusion of 5-FU before liver transplantation for extrahepatic cholangiocarcinomas [98]. Further evaluation of this strategy with a modification of the chemotherapy regimen resulted in significantly improved outcomes after liver transplantation in patients with perihilar cholangiocarcinomas [99]. Pretransplant treatment consisted of external beam radiation with 4500 cGy in 30 fractions with concomitant chemotherapy with 500 mg/m2/d of 5-FU for the first 3 days of radiation. Chemoradiotherapy was followed by brachytherapy with 2000 to 3000 cGy of iridium 192. Upon completion, patients were treated with 2000 mg/m2/d of capecitabine 2 of every 3 weeks until transplantation. Patients with surgically confirmed stage I or II disease were approved for liver transplantation. Five-year recurrence rates were 12%, and the overall 5-year survival rate in intention-to-treat analysis was 58% and 81% in patients who underwent liver transplantation. The results were compared with retrospective data from patients who had undergone potentially curative resection at the same institution between 1993 and 2004. The 5-year survival rate in the resection group was 21% and the 5-year recurrence rate 58%. Risk factors for tumor recurrence in patients treated with this neoadjuvant chemoradiotherapy approach followed by transplantation in a Cox regression analysis were older age, a level of CA 19-9 greater than 100 U/mL on the day of transplantation, prior cholecystectomy, a mass on cross-sectional imaging, residual tumor greater than 2 cm in explant, tumor grade, and perineural invasion in explant [100]. A similar protocol involving brachytherapy with 6000 cGy of iridium 192 and chemotherapy of 300 mg/m2/d of 5-FU but no external beam radiation was evaluated at the University of Nebraska [101]. Long-term disease-free survival was reported in 45% of transplanted patients; however, histopathologic analysis of explants showed the inclusion of stage III tumors in 46% of transplanted patients. The results of these studies show the importance of careful patient selection based on thorough surgical staging as well as the feasibility of a neoadjuvant chemoradiotherapeutic strategy (Box 1). If these requirements are met, excellent results can be achieved in patients with unresectable, localized, and regional lymph node–negative perihilar cholangiocarcinomas [102]. In contrast to the excellent outcomes with liver transplantation for extrahepatic perihilar cholangiocarcinomas, liver transplantation for intrahepatic cholangiocarcinomas is still fraught with disease recurrence and cannot be advocated. Local palliative therapy Photodynamic therapy Photodynamic therapy includes the application of a photosensitizing agent followed by exposure to light at a wavelength corresponding to the 142 BLECHACZ & GORES Box 1. Criteria for liver transplantation Diagnostic criteria Positive (transluminal) biopsy Positive conventional cytology on brush cytology Stricture plus FISH polysomy Mass lesion on cross-sectional imaging Malignant appearing stricture and persistent CA 19-9 >100 U/mL in the absence of cholangitis Exclusion criteria Prior radiation or chemotherapy Uncontrolled infection Intrahepatic metastases Extrahepatic or distal lymph node metastases Other malignancy within 5 years of cholangiocarcinoma diagnosis Age <18 or >65 years Comorbidities forbidding chemo- or radiotherapy or liver transplantation Hilar mass on cross-sectional imaging with a radial diameter of >3 cm absorption spectrum of the photosensitizer. Illumination initiates a type II photochemical reaction resulting in the generation of reactive oxygen species [103]. The antiproliferative effect is mediated by cell death induced by reactive oxygen species as well as thromboses within the tumor-supplying vessels, with ischemia as well as tumor-specific immune reactions [104–106]. The most commonly used compound is porfimer, a hematoporphyrin derivative that is activated at a wavelength of 630 nm and shown to cause cell death at a tissue depth of 4 to 6 mm [107]. Several studies have evaluated the effects of photodynamic therapy in patients with unresectable cholangiocarcinomas [108–110]. The results of these studies indicate a reduction in tumor thickness and an improvement of cholestasis and life quality [110,111]. Several studies also show a trend toward improved survival [111–115]. Two studies also evaluated photodynamic therapy as neoadjuvant or adjuvant treatment [90,116]; however, neither one was a controlled study. A recent study evaluating photodynamic therapy in patients with mostly Bismuth type III and IV cholangiocarcinoma found on multivariate analysis that a visible mass on imaging, low serum albumin levels, and a prolonged time between diagnosis and photodynamic therapy were predictors of poorer survival [117]. Photodynamic therapy is a reasonable approach for palliation in cholangiocarcinomas [118]. Its role as a neoadjuvant or adjuvant treatment requires further study. CHOLANGIOCARCINOMA 143 Radiotherapy Other techniques for local ablation include radiotherapy, radiofrequency ablation, and transcatheter ablation. There are two main administration modes for radiotherapy for cholangiocarcinomasdexternal beam radiotherapy and intraluminal iridium 192 brachytherapy. Several uncontrolled studies have evaluated radiotherapy in the adjuvant, neoadjuvant, and palliative setting [119–121]. In the palliative setting, survival benefits in a subset of patients without metastases were described [122]; however, the studies were uncontrolled, the results mixed, and the radiation had significant morbidity including gastrointestinal bleeding, strictures, small bowel obstruction, and even hepatic decompensation [123]. The authors do not employ postoperative external beam radiotherapy as an adjuvant strategy at their center. Systemic therapy There are no randomized controlled studies evaluating the effect of chemotherapy in cholangiocarcinoma. Existing data are derived from case reports or small clinical studies with insufficient statistical power to allow definitive conclusions. Several different chemotherapeutic drugs have been evaluated. In general, tumor response to these drugs was poor. The most commonly studied chemotherapeutic drugs include 5-FU and gemcitabine. 5-FU has been studied extensively as a monotherapeutic agent as well as in combination with other chemotherapeutic agents such as doxorubicin, epirubicin, cisplatin, lomustine, mitomycin C, paclitaxel, and other drugs (eg, interferon-a) [124–133]. These studies were limited in the number of patients studied, nonrandomized, and noncontrolled, and were not able to demonstrate significant tumor responses or significant prolongation of life. More recent studies have focused on gemcitabine, which was approved in 2002 by the US Food and Drug Administration for cholangiocarcinoma [134]. Studies evaluating gemcitabine as a monotherapeutic agent or in combination with other chemotherapeutic agents such as cisplatin, oxaliplatin, docetaxel, mitomycin C, and 5-FU/leukovorin reported up to 60% response rates [135,136]. Nevertheless, there are no randomized controlled studies evaluating gemcitabine in cholangiocarcinoma; therefore, its impact on survival is unclear. Targeted chemotherapy We are rapidly entering the era of targeted chemotherapy for solid malignancies. For example, antiangiogenic therapies and targeted inhibition of receptor tyrosine kinases are now approved for several malignancies. Such therapies have not yet been thoroughly exploited for the treatment of cholangiocarcinoma. Targeted inhibition of the epidermal growth factor receptor has been reported with a suggestion of benefit [137,138]. Potential therapies in the future may include targeted inhibition of IL-6, blockade 144 BLECHACZ & GORES of Mcl-1 expression/function, and employment of the death ligand agonist, tumor necrosis factordrelated, apoptosis-inducing ligand (TRAIL). It is hoped that such trials can be developed for cholangiocarcinomas. Palliation of cholestasis The main cause of morbidity in cholangiocarcinoma is cholestasis and its complications including cholangitis and pruritus. Several treatment options for restoration of biliary drainage exist, including endoscopic treatment via ERCP, surgical, or percutaneous approaches. Surgical drainage is achieved by choledochojejunostomy or hepaticojejunostomy and radiologic treatment by PTC with stent placement. A comparison of endoscopic stent placement with surgical biliary bypass showed similar efficiency in the treatment of malignant cholestasis but lower mortality, treatment-related early complications, and shorter hospital stay with endoscopic treatment [139–141]; therefore, endoscopic restoration of biliary drainage is generally preferred. In complete biliary obstruction, percutaneous or surgical methods can be unavoidable. A comparison between unilateral and bilateral hepatic duct drainage showed that unilateral stent placement achieved similar rates of successful drainage as bilateral stenting [142]. Plastic stents require exchange in 2- to 3-month intervals because they tend to become occluded by a biofilm of bacteria and proteinacious material, but they are preferred in patients with expected survival of less than 6 months or those awaiting planned surgery [143]. Metal stents are superior in stent patency and more cost effective in patients with anticipated survival of greater than 6 months [144]. Summary Cholangiocarcinoma is a highly malignant tumor and the second most common form of primary hepatic carcinoma. Its incidence has increased within the last 3 decades without clear etiologic explanations for the increase. Its prognosis is devastating, and the only curative therapy is surgical; however, significant progress has been achieved in our understanding of the etiology and molecular pathogenesis of this malignancy. Also, progress has occurred in diagnosis and therapy. With the increasing arsenal of diagnostic modalities, patients can potentially be diagnosed at earlier stages, thereby making them amenable to curative therapies. With the increase in aggressive surgical management, the results of resection have improved as reflected in better overall outcomes. For patients with unresectable perihilar cholangiocarcinomas, impressive 5-year survival rates can be achieved with liver transplantation combined with neoadjuvant chemoradiotherapy in highly selected patients. With the increasing knowledge of the molecular pathogenesis of this disease, there is hope for nonsurgical alternatives in the future, especially targeted therapies. CHOLANGIOCARCINOMA 145 References [1] de Groen PC, Gores GJ, LaRusso NF, et al. Biliary tract cancers. N Engl J Med 1999;341: 1368–78. [2] Renshaw K. Malignant neoplasms of the extrahepatic biliary ducts. Ann Surg 1922;76: 205–21. [3] Goldzieher M, von Bokay Z. Der primaere Leberkrebs. Virchows Arch 1911;203:75–131. [4] Yamagiwa K. Kenntnis des primaren parenchy: matosen Leberkarzinoms (‘‘Hepatoma’’). Virchows Arch 1911;206:437–67. [5] Klatskin G. Adenocarcinoma of the hepatic duct at its bifurcation within the porta hepatis: an unusual tumor with distinctive clinical and pathological features. Am J Med 1965;38: 241–56. [6] Hirohashi K, Venishi T, Kubo S, et al. Macroscopic types of intrahepatic cholangiocarcinoma: clinicopathologic features and surgical outcomes. Hepatogastroenterology 2002;49: 326–9. [7] Olnes MJ, Erlich R. A review and update on cholangiocarcinoma. Oncology 2004;66: 167–79. [8] Parker SL, Tong T, Bolden S, et al. Cancer statistics, 1996. CA Cancer J Clin 1996;46: 5–27. [9] Shaib Y, El-Serag HB. The epidemiology of cholangiocarcinoma. Semin Liver Dis 2004;24: 115–25. [10] Patel T. Increasing incidence and mortality of primary intrahepatic cholangiocarcinoma in the United States. Hepatology 2001;33:1353–7. [11] Shaib YH, Davila JA, McGlynn K, et al. Rising incidence of intrahepatic cholangiocarcinoma in the United States: a true increase? J Hepatol 2004;40:472–7. [12] Mouzas IA, et al. Increasing incidence of cholangiocarcinoma in Crete 1992-2000. Anticancer Res 2002;22:3637–41. [13] Okuda K, Nakanuma Y, Miyazaki M. Cholangiocarcinoma: recent progress. Part 1. Epidemiology and etiology. J Gastroenterol Hepatol 2002;17:1049–55. [14] Welzel TM, McGlynn KA, Hsing AW, et al. Impact of classification of hilar cholangiocarcinomas (Klatskin tumors) on the incidence of intra- and extrahepatic cholangiocarcinoma in the United States. J Natl Cancer Inst 2006;98:873–5. [15] Patel T. Worldwide trends in mortality from biliary tract malignancies. BMC Cancer 2002; 2:1–5. [16] McLean L, Patel T. Racial and ethnic variations in the epidemiology of intrahepatic cholangiocarcinoma in the United States. Liver Int 2006;26:1047–53. [17] Burak K, et al. Incidence and risk factors for cholangiocarcinoma in primary sclerosing cholangitis. Am J Gastroenterol 2004;99:523–6. [18] Bergquist A, et al. Hepatic and extrahepatic malignancies in primary sclerosing cholangitis. J Hepatol 2002;36:321–7. [19] Watanapa P, Watanapa WB. Liver fluke-associated cholangiocarcinoma. Br J Surg 2002; 89:962–70. [20] Kurathong S, et al. Opisthorchis viverrini infection and cholangiocarcinoma: a prospective, case-controlled study. Gastroenterology 1985;89:151–6. [21] Tesana S, et al. Ultrastructural and immunohistochemical analysis of cholangiocarcinoma in immunized Syrian golden hamsters infected with Opisthorchis viverrini and administered with dimethylnitrosamine. Parasitol Int 2000;49:239–51. [22] Parkin DM, et al. Liver cancer in Thailand. I. A case-control study of cholangiocarcinoma. Int J Cancer 1991;48:323–8. [23] Kubo S, Kinoshita H, Hirohashi K, et al. Hepatolithiasis associated with cholangiocarcinoma. World J Surg 1995;19:637–41. [24] Lesurtel M, et al. Intrahepatic cholangiocarcinoma and hepatolithiasis: an unusual association in Western countries. Eur J Gastroenterol Hepatol 2002;14:1025–7. 146 BLECHACZ & GORES [25] Su CH, Shyr YM, Lui WY, et al. Hepatolithiasis associated with cholangiocarcinoma. Br J Surg 1997;84:969–73. [26] Chapman RW. Risk factors for biliary tract carcinogenesis. Ann Oncol 1999;10(Suppl 4): 308–11. [27] Lipsett PA, Pitt HA, Colombani PM, et al. Choledochal cyst disease: a changing pattern of presentation. Ann Surg 1994;220:644–52. [28] Scott J, Shousha S, Thomas HC, et al. Bile duct carcinoma: a late complication of congenital hepatic fibrosis. Case report and review of literature. Am J Gastroenterol 1980;73: 113–9. [29] Gores GJ. Cholangiocarcinoma: current concepts and insights. Hepatology 2003;37: 961–9. [30] Malhi H, Gores GJ. Cholangiocarcinoma: modern advances in understanding a deadly old disease. J Hepatol 2006;45:856–67. [31] Berthiaume EP, Wands J. The molecular pathogenesis of cholangiocarcinoma. Semin Liver Dis 2004;24:127–37. [32] Okuda K, Nakanuma Y, Miyazaki M. Cholangiocarcinoma: recent progress. Part 2. Molecular pathology and treatment. J Gastroenterol Hepatol 2002;17:1056–63. [33] Moss SF, Blaser MJ. Mechanisms of disease: inflammation and the origins of cancer. Nat Clin Pract Oncol 2005;2:90–7, quiz 1 p following 113. [34] Okada K, Shimizu Y, Nambu S, et al. Interleukin-6 functions as an autocrine growth factor in a cholangiocarcinoma cell line. J Gastroenterol Hepatol 1994;9:462–7. [35] Sugawara H, et al. Relationship between interleukin-6 and proliferation and differentiation in cholangiocarcinoma. Histopathology 1998;33:145–53. [36] Park J, Tadlock L, Gores GJ, et al. Inhibition of interleukin 6-mediated mitogen-activated protein kinase activation attenuates growth of a cholangiocarcinoma cell line. Hepatology 1999;30:1128–33. [37] Isomoto H, et al. Interleukin 6 upregulates myeloid cell leukemia-1 expression through a STAT3 pathway in cholangiocarcinoma cells. Hepatology 2005;42:1329–38. [38] Kobayashi S, Werneburg NW, Bronk SF, et al. Interleukin-6 contributes to Mcl-1 upregulation and TRAIL resistance via an Akt-signaling pathway in cholangiocarcinoma cells. Gastroenterology 2005;128:2054–65. [39] Isomoto H, et al. Sustained IL-6/STAT-3 signaling in cholangiocarcinoma cells due to SOCS-3 epigenetic silencing. Gastroenterology 2007;132:384–96. [40] Yoon JH, et al. Bile acids inhibit Mcl-1 protein turnover via an epidermal growth factor receptor/Raf-1-dependent mechanism. Cancer Res 2002;62:6500–5. [41] Werneburg NW, Yoon JH, Higuchi H, et al. Bile acids activate EGF receptor via a TGFalpha-dependent mechanism in human cholangiocyte cell lines. Am J Physiol Gastrointest Liver Physiol 2003;285:G31–6. [42] Yamagiwa Y, Meng F, Patel T. Interleukin-6 decreases senescence and increases telomerase activity in malignant human cholangiocytes. Life Sci 2006;78:2494–502. [43] Jaiswal M, LaRusso NF, Burgart LJ, et al. Inflammatory cytokines induce DNA damage and inhibit DNA repair in cholangiocarcinoma cells by a nitric oxide–dependent mechanism. Cancer Res 2000;60:184–90. [44] Torok NJ, Higuchi H, Bronk S, et al. Nitric oxide inhibits apoptosis downstream of cytochrome C release by nitrosylating caspase 9. Cancer Res 2002;62:1648–53. [45] Malhi H, Gores GJ. Review article: the modern diagnosis and therapy of cholangiocarcinoma. Aliment Pharmacol Ther 2006;23:1287–96. [46] Khan SA, et al. Guidelines for the diagnosis and treatment of cholangiocarcinoma: consensus document. Gut 2002;51(Suppl 6):VI1–9. [47] Robledo R, Muro A, Prieto ML. Extrahepatic bile duct carcinoma: US characteristics and accuracy in demonstration of tumors. Radiology 1996;198:869–73. [48] Hann LE, Greatrex KV, Bach AM, et al. Cholangiocarcinoma at the hepatic hilus: sonographic findings. AJR Am J Roentgenol 1997;168:985–9. CHOLANGIOCARCINOMA 147 [49] Slattery JM, Sahani DV. What is the current state-of-the-art imaging for detection and staging of cholangiocarcinoma? Oncologist 2006;11:913–22. [50] Foley WD, Quiroz FA. The role of sonography in imaging of the biliary tract. Ultrasound Q 2007;23:123–35. [51] Hann LE, et al. Hepatic lobar atrophy: association with ipsilateral portal vein obstruction. AJR Am J Roentgenol 1996;167:1017–21. [52] Manfredi R, Barbaro B, Masselli G, et al. Magnetic resonance imaging of cholangiocarcinoma. Semin Liver Dis 2004;24:155–64. [53] Braga HJ, Imam K, Bluemke DA. MR imaging of intrahepatic cholangiocarcinoma: use of ferumoxides for lesion localization and extension. AJR Am J Roentgenol 2001;177:111–4. [54] Raman SS, et al. Hepatic MR imaging using ferumoxides: prospective evaluation with surgical and intraoperative sonographic confirmation in 25 cases. AJR Am J Roentgenol 2001;177:807–12. [55] Gores GJ. Early detection and treatment of cholangiocarcinoma. Liver Transpl 2000;6: S30–4. [56] Kluge R, et al. Positron emission tomography with [(18)F]fluoro-2-deoxy-D-glucose for diagnosis and staging of bile duct cancer. Hepatology 2001;33:1029–35. [57] Fritscher-Ravens A, et al. FDG PET in the diagnosis of hilar cholangiocarcinoma. Nucl Med Commun 2001;22:1277–85. [58] Petrowsky H, et al. Impact of integrated positron emission tomography and computed tomography on staging and management of gallbladder cancer and cholangiocarcinoma. J Hepatol 2006;45:43–50. [59] Chen CY, Shiesh SC, Tsao HC, et al. The assessment of biliary CA 125, CA 19-9 and CEA in diagnosing cholangiocarcinoma: the influence of sampling time and hepatolithiasis. Hepatogastroenterology 2002;49:616–20. [60] Koprowski H, et al. Colorectal carcinoma antigens detected by hybridoma antibodies. Somatic Cell Genet 1979;5:957–71. [61] Nehls O, Gregor M, Klump B. Serum and bile markers for cholangiocarcinoma. Semin Liver Dis 2004;24:139–54. [62] Narimatsu H, et al. Lewis and secretor gene dosages affect CA 19-9 and DU-PAN-2 serum levels in normal individuals and colorectal cancer patients. Cancer Res 1998;58:512–8. [63] Vestergaard EM, et al. Reference values and biological variation for tumor marker CA 19-9 in serum for different Lewis and secretor genotypes and evaluation of secretor and Lewis genotyping in a Caucasian population. Clin Chem 1999;45:54–61. [64] Kim HJ, et al. A new strategy for the application of CA 19-9 in the differentiation of pancreaticobiliary cancer: analysis using a receiver operating characteristic curve. Am J Gastroenterol 1999;94:1941–6. [65] Akdogan M, et al. Extraordinarily elevated CA 19-9 in benign conditions: a case report and review of the literature. Tumori 2001;87:337–9. [66] Albert MB, Steinberg WM, Henry JP. Elevated serum levels of tumor marker CA 19-9 in acute cholangitis. Dig Dis Sci 1988;33:1223–5. [67] Levy C, et al. The value of serum CA 19-9 in predicting cholangiocarcinomas in patients with primary sclerosing cholangitis. Dig Dis Sci 2005;50:1734–40. [68] Rabinovitz M, et al. Diagnostic value of brush cytology in the diagnosis of bile duct carcinoma: a study in 65 patients with bile duct strictures. Hepatology 1990;12:747–52. [69] Ponsioen CY, et al. Value of brush cytology for dominant strictures in primary sclerosing cholangitis. Endoscopy 1999;31:305–9. [70] Lee JG, Leung JW, Baillie J, et al. Benign, dysplastic, or malignant: making sense of endoscopic bile duct brush cytology. Results in 149 consecutive patients. Am J Gastroenterol 1995;90:722–6. [71] Furmanczyk PS, Grieco VS, Agoff SN. Biliary brush cytology and the detection of cholangiocarcinoma in primary sclerosing cholangitis: evaluation of specific cytomorphologic features and CA 19-9 levels. Am J Clin Pathol 2005;124:355–60. 148 BLECHACZ & GORES [72] Baron TH, et al. A prospective comparison of digital image analysis and routine cytology for the identification of malignancy in biliary tract strictures. Clin Gastroenterol Hepatol 2004;2:214–9. [73] Moreno Luna LE, Gores GJ. Advances in the diagnosis of cholangiocarcinoma in patients with primary sclerosing cholangitis. Liver Transpl 2006;12:S15–9. [74] Moreno Luna LE, et al. Advanced cytologic techniques for the detection of malignant pancreatobiliary strictures. Gastroenterology 2006;131:1064–72. [75] Nagorney DM, Kendrick ML. Hepatic resection in the treatment of hilar cholangiocarcinoma. Adv Surg 2006;40:159–71. [76] Patel T. Cholangiocarcinoma. Nat Clin Pract Gastroenterol Hepatol 2006;3:33–42. [77] Jarnagin WR, Shoup M. Surgical management of cholangiocarcinoma. Semin Liver Dis 2004;24:189–99. [78] Jarnagin WR, et al. Staging, resectability, and outcome in 225 patients with hilar cholangiocarcinoma. Ann Surg 2001;234:507–17 [discussion: 517–9]. [79] Yeh CN, Jan YY, Yeh TS, et al. Hepatic resection of the intraductal papillary type of peripheral cholangiocarcinoma. Ann Surg Oncol 2004;11:606–11. [80] Ohtsuka M, et al. Results of surgical treatment for intrahepatic cholangiocarcinoma and clinicopathological factors influencing survival. Br J Surg 2002;89:1525–31. [81] DeOliveira ML, et al. Cholangiocarcinoma: thirty-one-year experience with 564 patients at a single institution. Ann Surg 2007;245:755–62. [82] Neuhaus P, et al. Extended resections for hilar cholangiocarcinoma. Ann Surg 1999;230: 808–18 [discussion: 819]. [83] Silva MA, et al. Surgery for hilar cholangiocarcinoma: a 10 year experience of a tertiary referral centre in the UK. Eur J Surg Oncol 2005;31:533–9. [84] Pichlmayr R, et al. Surgical treatment in proximal bile duct cancer: a single-center experience. Ann Surg 1996;224:628–38. [85] Weber SM, et al. Intrahepatic cholangiocarcinoma: resectability, recurrence pattern, and outcomes. J Am Coll Surg 2001;193:384–91. [86] Kawarada Y, Das BC, Naganuma T, et al. Surgical treatment of hilar bile duct carcinoma: experience with 25 consecutive hepatectomies. J Gastrointest Surg 2002;6:617–24. [87] Hemming AW, Reed AI, Fujita S, et al. Surgical management of hilar cholangiocarcinoma. Ann Surg 2005;241:693–9 [discussion: 699–702]. [88] Gazzaniga GM, Filauro M, Bagarolo C, et al. Surgery for hilar cholangiocarcinoma: an Italian experience. J Hepatobiliary Pancreat Surg 2000;7:122–7. [89] McMasters KM, et al. Neoadjuvant chemoradiation for extrahepatic cholangiocarcinoma. Am J Surg 1997;174:605–8 [discussion: 608–9]. [90] Wiedmann M, et al. Neoadjuvant photodynamic therapy as a new approach to treating hilar cholangiocarcinoma: a phase II pilot study. Cancer 2003;97:2783–90. [91] Makuuchi M, et al. Preoperative portal embolization to increase safety of major hepatectomy for hilar bile duct carcinoma: a preliminary report. Surgery 1990; 107:521–7. [92] Vauthey JN, et al. Standardized measurement of the future liver remnant prior to extended liver resection: methodology and clinical associations. Surgery 2000;127:512–9. [93] Abdalla EK, Barnett CC, Doherty D, et al. Extended hepatectomy in patients with hepatobiliary malignancies with and without preoperative portal vein embolization. Arch Surg 2002;137:675–80 [discussion: 680–1]. [94] Nagino M, et al. Two hundred forty consecutive portal vein embolizations before extended hepatectomy for biliary cancer: surgical outcome and long-term follow-up. Ann Surg 2006; 243:364–72. [95] Meyer CG, Penn I, James L. Liver transplantation for cholangiocarcinoma: results in 207 patients. Transplantation 2000;69:1633–7. [96] Casavilla FA, et al. Hepatic resection and transplantation for peripheral cholangiocarcinoma. J Am Coll Surg 1997;185:429–36. CHOLANGIOCARCINOMA 149 [97] Iwatsuki S, et al. Treatment of hilar cholangiocarcinoma (Klatskin tumors) with hepatic resection or transplantation. J Am Coll Surg 1998;187:358–64. [98] De Vreede I, et al. Prolonged disease-free survival after orthotopic liver transplantation plus adjuvant chemoirradiation for cholangiocarcinoma. Liver Transpl 2000;6:309–16. [99] Rea DJ, et al. Liver transplantation with neoadjuvant chemoradiation is more effective than resection for hilar cholangiocarcinoma. Ann Surg 2005;242:451–8 [discussion: 458–61]. [100] Heimbach JK, et al. Predictors of disease recurrence following neoadjuvant chemoradiotherapy and liver transplantation for unresectable perihilar cholangiocarcinoma. Transplantation 2006;82:1703–7. [101] Sudan D, et al. Radiochemotherapy and transplantation allow long-term survival for nonresectable hilar cholangiocarcinoma. Am J Transplant 2002;2:774–9. [102] Heimbach JK, et al. Liver transplantation for unresectable perihilar cholangiocarcinoma. Semin Liver Dis 2004;24:201–7. [103] Ortner MA, Dorta G. Technology insight: photodynamic therapy for cholangiocarcinoma. Nat Clin Pract Gastroenterol Hepatol 2006;3:459–67. [104] Abels C. Targeting of the vascular system of solid tumours by photodynamic therapy (PDT). Photochem Photobiol Sci 2004;3:765–71. [105] Krammer B. Vascular effects of photodynamic therapy. Anticancer Res 2001;21:4271–7. [106] Korbelik M, Dougherty GJ. Photodynamic therapy-mediated immune response against subcutaneous mouse tumors. Cancer Res 1999;59:1941–6. [107] Dougherty TJ, Mang TS. Characterization of intra-tumoral porphyrin following injection of hematoporphyrin derivative or its purified component. Photochem Photobiol 1987;46: 67–70. [108] Rumalla A, et al. Endoscopic application of photodynamic therapy for cholangiocarcinoma. Gastrointest Endosc 2001;53:500–4. [109] Ortner MA, et al. Photodynamic therapy of nonresectable cholangiocarcinoma. Gastroenterology 1998;114:536–42. [110] Berr F, et al. Photodynamic therapy for advanced bile duct cancer: evidence for improved palliation and extended survival. Hepatology 2000;31:291–8. [111] Ortner ME, et al. Successful photodynamic therapy for nonresectable cholangiocarcinoma: a randomized prospective study. Gastroenterology 2003;125:1355–63. [112] Shim CS, et al. Prospective study of the effectiveness of percutaneous transhepatic photodynamic therapy for advanced bile duct cancer and the role of intraductal ultrasonography in response assessment. Endoscopy 2005;37:425–33. [113] Harewood GC, et al. Pilot study to assess patient outcomes following endoscopic application of photodynamic therapy for advanced cholangiocarcinoma. J Gastroenterol Hepatol 2005;20:415–20. [114] Dumoulin FL, et al. Phase II study of photodynamic therapy and metal stent as palliative treatment for nonresectable hilar cholangiocarcinoma. Gastrointest Endosc 2003;57: 860–7. [115] Zoepf T, Jakobs R, Arnold JC, et al. Palliation of nonresectable bile duct cancer: improved survival after photodynamic therapy. Am J Gastroenterol 2005;100:2426–30. [116] Nanashima A, et al. Adjuvant photodynamic therapy for bile duct carcinoma after surgery: a preliminary study. J Gastroenterol 2004;39:1095–101. [117] Prasad GA, et al. Factors associated with increased survival after photodynamic therapy for cholangiocarcinoma. Clin Gastroenterol Hepatol 2007;5:743–8. [118] Berr F. Photodynamic therapy for cholangiocarcinoma. Semin Liver Dis 2004;24:177–87. [119] Czito BG, Anscher MS, Willett CG. Radiation therapy in the treatment of cholangiocarcinoma. Oncology (Williston Park) 2006;20:873–84 [discussion: 886–8, 893–5]. [120] Foo ML, Gunderson LL, Bender CE, et al. External radiation therapy and transcatheter iridium in the treatment of extrahepatic bile duct carcinoma. Int J Radiat Oncol Biol Phys 1997;39:929–35. 150 BLECHACZ & GORES [121] Pitt HA, et al. Perihilar cholangiocarcinoma: postoperative radiotherapy does not improve survival. Ann Surg 1995;221:788–97 [discussion: 797–8]. [122] Grove MK, Hermann RE, Vogt DP, et al. Role of radiation after operative palliation in cancer of the proximal bile ducts. Am J Surg 1991;161:454–8. [123] Cherqui D, et al. Intrahepatic cholangiocarcinoma: results of aggressive surgical management. Arch Surg 1995;130:1073–8. [124] Falkson G, MacIntyre JM, Moertel CG. Eastern cooperative oncology group experience with chemotherapy for inoperable gallbladder and bile duct cancer. Cancer 1984;54:965–9. [125] Takada T, et al. Comparison of 5-fluorouracil, doxorubicin and mitomycin C with 5fluorouracil alone in the treatment of pancreatic-biliary carcinomas. Oncology 1994;51: 396–400. [126] Choi CW, et al. Effects of 5-fluorouracil and leucovorin in the treatment of pancreaticbiliary tract adenocarcinomas. Am J Clin Oncol 2000;23:425–8. [127] Patt YZ, et al. Phase II trial of intravenous fluorouracil and subcutaneous interferon alfa-2b for biliary tract cancer. J Clin Oncol 1996;14:2311–5. [128] Patt YZ, et al. Phase II trial of cisplatin, interferon alpha-2b, doxorubicin, and 5-fluorouracil for biliary tract cancer. Clin Cancer Res 2001;7:3375–80. [129] Ducreux M, et al. Effective treatment of advanced biliary tract carcinoma using 5-fluorouracil continuous infusion with cisplatin. Ann Oncol 1998;9:653–6. [130] Lee MA, Woo IS, Kang JH, et al. Epirubicin, cisplatin, and protracted infusion of 5-FU (ECF) in advanced intrahepatic cholangiocarcinoma. J Cancer Res Clin Oncol 2004;130:346–50. [131] Taieb J, et al. Optimization of 5-fluorouracil (5-FU)/cisplatin combination chemotherapy with a new schedule of leucovorin, 5-FU and cisplatin (LV5FU2-P regimen) in patients with biliary tract carcinoma. Ann Oncol 2002;13:1192–6. [132] Raderer M, et al. Two consecutive phase II studies of 5-fluorouracil/leucovorin/mitomycin C and of gemcitabine in patients with advanced biliary cancer. Oncology 1999;56:177–80. [133] Jones DV Jr, Lozano R, Hoque A, et al. Phase II study of paclitaxel therapy for unresectable biliary tree carcinomas. J Clin Oncol 1996;14:2306–10. [134] Alberts SR, et al. Treatment options for hepatobiliary and pancreatic cancer. Mayo Clin Proc 2007;82:628–37. [135] Kiba T, et al. Single-agent gemcitabine for biliary tract cancers: study outcomes and systematic review of the literature. Oncology 2006;70:358–65. [136] Scheithauer W. Review of gemcitabine in biliary tract carcinoma. Semin Oncol 2002;29: 40–5. [137] Jimeno A, et al. Epidermal growth factor receptor dynamics influence response to epidermal growth factor receptor targeted agents. Cancer Res 2005;65:3003–10. [138] Wiedmann M, et al. Novel targeted approaches to treating biliary tract cancer: the dual epidermal growth factor receptor and ErbB-2 tyrosine kinase inhibitor NVP-AEE788 is more efficient than the epidermal growth factor receptor inhibitors gefitinib and erlotinib. Anticancer Drugs 2006;17:783–95. [139] Shepherd HA, et al. Endoscopic biliary endoprosthesis in the palliation of malignant obstruction of the distal common bile duct: a randomized trial. Br J Surg 1988;75:1166–8. [140] Andersen JR, Sorensen SM, Kruse A, et al. Randomised trial of endoscopic endoprosthesis versus operative bypass in malignant obstructive jaundice. Gut 1989;30:1132–5. [141] Smith AC, Dowsett JF, Russell RC, et al. Randomised trial of endoscopic stenting versus surgical bypass in malignant low bile duct obstruction. Lancet 1994;344:1655–60. [142] De Palma GD, Galloro G, Siciliano S, et al. Unilateral versus bilateral endoscopic hepatic duct drainage in patients with malignant hilar biliary obstruction: results of a prospective, randomized, and controlled study. Gastrointest Endosc 2001;53:547–53. [143] Abu-Hamda EM, Baron TH. Endoscopic management of cholangiocarcinoma. Semin Liver Dis 2004;24:165–75. [144] Kaassis M, et al. Plastic or metal stents for malignant stricture of the common bile duct? Results of a randomized prospective study. Gastrointest Endosc 2003;57:178–82.
 0
0

No more boring flashcards learning!
Learn languages, math, history, economics, chemistry and more with free StudyLib Extension!
- Distribute all flashcards reviewing into small sessions
- Get inspired with a daily photo
- Import sets from Anki, Quizlet, etc
- Add Active Recall to your learning and get higher grades!
Related documents




Add this document to collection(s)
You can add this document to your study collection(s)
Sign in Available only to authorized usersAdd this document to saved
You can add this document to your saved list
Sign in Available only to authorized users