Verification of Health Requirements - School Held Student Health Records
advertisement

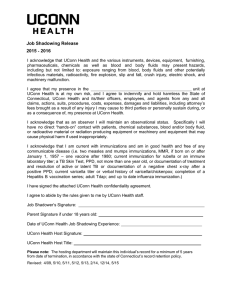
Verification of Health Requirements - School Held Student Health Records Unpaid Educational School Sponsored Experience 2015-2016 I ________________________________________________ verify that the administrative (School/Agency Contact) offices at _____________________________________________ have on record that the (School of Origin) student(s) listed on following page have met the health requirements listed below. Health Requirements for an Unpaid Educational School Sponsored Experience: Documentation of vaccination with two doses of live measles and mumps vaccines (MMR) administered at least 28 days apart (one vaccine must be documented after 1980) or documented immunity by positive laboratory titers for measles and mumps or birth before January 1, 1957. Documentation of vaccination with one dose of live rubella (at least one MMR) or an immune laboratory titer. Evidence of a non-reactive PPD or a negative quantiferon gold test within the past year or documentation of treatment and resolution of active TB or documentation of an absence of symptoms and a negative chest x-ray after a positive PPD or positive quantiferon gold test. Documentation of two doses of varicella vaccine or laboratory evidence of immunity to varicella or history of previous varicella disease or herpes zoster diagnosed by a health care provider. Completion of a Hepatitis B vaccination series with documentation of immunity based upon a positive Hepatitis B Surface antibody titer. Documentation of adult Tdap Up to date influenza immunization Page 1 of 2 Date of Experience: _____________________________________________________________ Students enrolled in an Unpaid School Sponsored Experience at UConn Health (please print clearly): Student’s Name:_______________________________________________________________ Address: ______________________________________________________________________ Local Phone Number: ____________________________________________________________ Student’s Name:_______________________________________________________________ Address: ______________________________________________________________________ Local Phone Number: ____________________________________________________________ Student’s Name:______________________________________________________________ Address: ______________________________________________________________________ Local Phone Number: ____________________________________________________________ Student’s Name:______________________________________________________________ Address: ______________________________________________________________________ Local Phone Number: ____________________________________________________________ Student’s Name:______________________________________________________________ Address: ______________________________________________________________________ Local Phone Number: ____________________________________________________________ ________________ School Authorized Printed Name ________________ Institution _______________ School Authorized Signature __________________________________ Date This form is valid for students affiliating at UConn Health Please return to the student’s UConn Health Host Do not submit individual student health records Please note: The hosting department will maintain this individual’s record for a minimum of 5 years from date of termination, in accordance with the state of Connecticut’s record retention policy. Dev. 1999 Revised: 5/06, 6/07, 4/08, 4/09, 4/10, 5/11, 5/12, 5/13, 2/14, 6/14, 5/15 Page 2 of 2