OUTSIDE CLEARANCE FORM ************************************************************************************ EMPLOYEE NAME:
advertisement

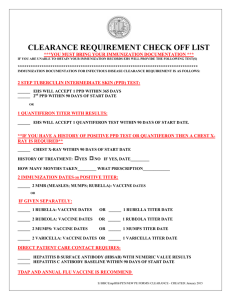
OUTSIDE CLEARANCE FORM SERVICES ARE TO BE DONE BY YOUR PCP (PRIMARY CARE PHYSICIAN) NOT EMPLOYEE HEALTH SERVICES HEALTH CLEARANCE VERIFICATION FOR: OBSERVERS/VISITING PROFESSORS/MISC EMPLOYEE NAME: DEPARTMENT LOCATION: PHONE NUMBER: DEPT CONTACT NAME & PHONE: ************************************************************************************ IMMUNIZATION DOCUMENTATION FOR INFECTIOUS DISEASE CLEARANCE IS AS FOLLOWS: TB SCREENING – WILL ACCEPT 1 PPD WITHIN 365 DAYS, and a 2nd PPD WITHIN 90 DAYS OR A QUANTIFERON TEST WITHIN 90 DAYS OF START DATE. MANDATORY 2 STEP TUBERCULIN INTERMEDIATE SKIN TEST (PPD) OR QUANTIFERON DATE PLACED: DATE READ RESULTS: ____ MM INDURATION NEG POS DATE PLACED: DATE READ RESULTS: ____ MM INDURATION NEG POS QUANTIFERON DATE: RESULTS: DATE OF ANNUAL TB SYMPTOM INTERVIEW: HISTORY OF A BCG VACCINATION: YES NEG POS NO (BCG IS A VACCINE GIVEN TO THOSE BORN OUTSIDE THE UNITED STATES.) HISTORY OF POSITIVE PPD OR QUANTIFERON TEST: A CHEST X-RAY IS REQUIRED WITHIN 3 MONTHS OF ARRIVAL CHEST X-RAY DATE: HISTORY OF TREATMENT: RESULTS: YES TB SYMPTOMS: NO IF YES, DATE: NEG POS HOW MANY MONTHS TAKEN: **MANDATORY 2 IMMUNIZATION DATES OR + POSITIVE TITER REQUIRED: **MMR (MEASLES; MUMPS; RUBELLA): VACCINE DATES: 1. 2. OR IF GIVEN SEPARATELY: **RUBELLA VACCINE DATES: 1. 2. OR TITER DATE: RESULTS: **RUBEOLA VACCINE DATES: 1. 2. OR TITER DATE: RESULTS: **MUMPS VACCINE DATES: 1. 2. OR TITER DATE: RESULTS: 2. OR TITER DATE: RESULTS: **VARICELLA: VACCINE DATES: 1. DIRECT PATIENT CARE CONTACT REQUIRES: HEPATITIS B SURFACE ANTIBODY (HBSAB) DATE: NUMERIC VALUE RESULTS: HEPATITIS C ANTIBODY TITER DATE: RESULTS: COLOR VISION TEST: NORMAL ABNORMAL mIU/ml . THIS EMPLOYEE HAS BEEN EDUCATED ON MODE OF TRANSMISSION, EXPOSURE, PREVENTION, REPORTING AND FOLLOW-UP FOR: AIRBORNE PATHOGENS BLOODBORNE PATHOGENS (TO BE PROVIDED BY DEPARTMENT – HOSPITAL POLICY 2001, 2002, 2010, 2011, 2150, 2164 AND 2167 FOR REVIEW) DO YOU HAVE HEALTH INSURANCE? YES NO - DO YOU HAVE A LOCAL PCP? YES NO I HAVE EVALUATED THIS EMPLOYEE AND HAVE FOUND HER/HIM TO BE FREE FROM INFECTIOUS DISEASE. PRIMARY CARE PHYSICIAN SIGNATURE: DATE: DEPARTMENT TO RETAIN ORIGINAL S:\HBC\EmpHlth\OUTSIDE CLEARANCE FORM REV:1-15-15