Hip Arthroscopy Rehabilitation Protocol Phase I: 0 – 4 weeks
advertisement

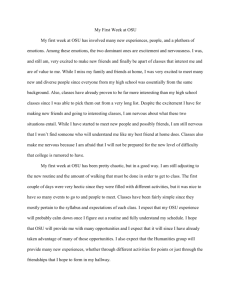
Hip Arthroscopy Rehabilitation Protocol Phase I: 0 – 4 weeks Goals: • • • • Protect healing tissue Restore ROM within pain restrictions Reduce pain and inflammation Enhance proper muscle activation/neuromuscular re-education Dynamic Warm-up • • • Gluteus activation and circumduction Progress to upright bike without resistance when able to perform without pain Upright stationary bike to be used 1-2 x/day once cleared by therapist or physician. No resistance added until 6 weeks Aquatic Therapy • • • • • Start 7 – 10 days post-op Use an occlusive cover for sutures Make arrangements with aquatic facility To be performed 2 – 4 times weekly, independent from physical therapy See attached handout for aquatic therapy guidelines Manual Therapy Soft tissue techniques should target: Iliopsoas ITB and TFL Adductors Gluteus medius Avoid increasing inflammation, pain. Mobility • PROM o Flexion, IR, ABD in pain-free ranges and without complaint of “pinching” o Can include external rotation and hip extension with caution o Do not move into or through soft tissue restriction until 2½ weeks post-op • Hip circumduction o 10 minutes @ 30o of flexion (5 min CW and 5 min CCW) o 10 minutes @ 70o of flexion (5 min CW and 5 min CCW) OSU Sports Medicine sportsmedicine.osu.edu 1 • FABER slide progression Begin at 4 weeks with PT-assisted FABER slides • Cat/camel in quadruped • Hook-lying butterflies and reverse butterflies • Quadruped posterior rocks OSU Sports Medicine sportsmedicine.osu.edu 2 • Prone lying, “belly time” Progress to propped on elbows, at least 20 minutes twice/day Stability • Gluteus activation progression (continue until activation is symmetrical) Begin with involved side activation in supine/prone and progressing to kneel, half kneel, standing • Transverse abdominus (TrA) – combine pelvic tilt with TrA OSU Sports Medicine sportsmedicine.osu.edu 3 Stability • Isometrics: abductors/adductors (supine) IR/ER (prone) • Double leg bridges within pain-free ROM • Begin weight shifts 2 weeks post-op, progressing to single leg balance • Clamshells after 3 weeks if pain-free Gait • • Weaning off crutches depends on patient’s tolerance to gradual increase in weightbearing. Patient should be progressed slowly from bilateral axial crutches to use of one crutch on nonoperative side. Patient may be progressed to full weight-bearing once painfree and able demonstrate ability to ambulate without antalgic pattern and with proper activation of gluteal musculature. Encourage contraction of gluteus muscles with push off and initiation of swing phase to reduce hip flexor overuse or a “pulling” swing phase may also cue patient to push off with calf muscles to reduce hip flexor overuse. OSU Sports Medicine sportsmedicine.osu.edu 4 Consider: • • • • • Focus on mobility of the hip in Phase I Focus on gluteus/TA activation Upper body conditioning can include suspension-type conditioning Lower extremities should be positioned as to avoid pinching in hip or pain with weightbearing Avoid positions that reproduce pain/pinch Criteria to Progress to Phase II • • • • • Greater than 100o flexion without complaints of pinching Ambulate without compensatory pattern or pain Ability to complete all Phase I exercise without increase in pain Improved activation/isolation of glutes, quads and abdominal musculature without cueing No effusion, muscular irritation or pain. Do not continue to progress patient until symptoms subside OSU Sports Medicine sportsmedicine.osu.edu 5 Hip Arthroscopy Rehabilitation Protocol Phase II: 4 – 8 Weeks • • All repetitions should be controlled and slow, NOT explosive. Correct any compensatory movement patterns (anterior weight shift, pelvic drop, valgus collapse) Progress single leg stance balance/proprioception to unstable surfaces (Air-ex, BOSU, Dynadisc) Mobility/Flexibility Exercises • Continue stretches from Phase I • Progress to Thomas position for stretching (hip flexor, quads) • Standing IT band stretch • Continue with FABER mobility • Progress to independent FABER slides • Half-kneeling hip flexor stretch Add rotation at week 6 • Scar mobilization as needed • Continue with FABER mobility OSU Sports Medicine sportsmedicine.osu.edu 6 • Manual joint mobilizations GENTLE – avoid aggressive traction Strengthening/Stability • Prone hip extension Lie on stomach. Tighten glutes and lift leg while keeping knee straight. Progress to hip extension off end of plinth or over exercise ball. • Side lying hip abduction Lie on uninvolved side. Position upper leg in slight extension and lift up then slowly lower to starting position. Keep toes facing forward and hip extended. • Hip hikes Stand sideways on a step with uninvolved leg on a 4-inch step with involved lower extremity free of the step. Keep both hips facing forward with shoulders and pelvis shoulders level. While keeping your uninvolved leg straight, raise your hip straight up then lower slowly. OSU Sports Medicine sportsmedicine.osu.edu 7 • Leg press/unilateral leg press Sit or lie back in the seat with lower back and hips against the pads. Feet should be placed hip-width apart with feet above hips. Feet should be in a slightly toed-out position. Push on plate to straighten knees. Slowly bend knees and hips. Start bending knees only 45o, progress depth based on tolerance. Do not progress depth if patient complains of pinching or reproduction of symptoms. Progress to single leg. • Sport cord rotations – begin at 6 weeks Start with double leg rotations with band around waist, progress to single leg stance rotations. Patient should focus on good glute and core activation while maintaining a level pelvis and preventing any valgus collapse throughout lower extremity. Avoid pinching. • Posterior squats Position feet parallel to each other. Emphasize proper form with knees remaining above ankles without collapsing in or out. Start with partial knee bends and increase depth per tolerance without complaints of pinching. Progress to squats on unstable surfaces. Can use wall to facilitate posterior weight shift and proper squat mechanics. OSU Sports Medicine sportsmedicine.osu.edu 8 • Split squats/lunges Step forward with involved lower extremity. Lower hips toward floor then push through front foot to return to starting position. Depth is dependent on patient tolerance and no complaints of pinching. • Bridging progression Lie on back and position both feet on ball. Keep knees straight and raise hips off floor to form straight line from feet to shoulders. Return to starting position slowly. May progress to marching bridges and then single leg bridges after ~6 weeks, once able to perform double leg bridges on ball without anterior hip pain. OSU Sports Medicine sportsmedicine.osu.edu 9 • Step and holds Position in front of mirror. Step forward onto a slightly bent knee and balance for a few seconds. Maintain control of knee and do not let it move in or out. Knee should remain positioned directly above foot. • Romanian dead lift Start with feet parallel to each other. Lift uninvolved leg back and off the floor. Bend forward at the hips while maintaining a straight lower back position. Only bend forward as far as you can without rounding your lower back. • Sidesteps Start with knees and hips slightly flexed with resistance band positioned around ankles. Keep feet and knees pointed forward as you step sideways with leading leg then take a small step in same direction with back leg while maintaining tension in band. • Posterior reaches Start with knees and hips slightly flexed with resistance band around ankles. Step back with one leg at a 45o angle then return to starting position. OSU Sports Medicine sportsmedicine.osu.edu 10 • Planks Lie on your stomach with your elbows and forearms underneath your chest. Prop yourself up to form a plank using your knees/toes and forearms for support. Maintain a flat back. Do not allow your hips to sag towards the ground. Kneeling planks at Week 6 – trial full planks beginning at Week 8. • Side Planks Lie on your side with your elbow on the ground below your shoulder. Lift yourself up to form a plank. Hold this position until you can no longer maintain a straight line from your shoulders to your knee/toes. • Step-ups/step-downs Place foot on small (2- or 4-inch) step. Step up onto step then lower uninvolved foot back to the floor. Repeat. Increase step height per tolerance without pain or symptoms. • Stand with involved leg on a small step. Lower opposite foot to the ground by slowly bending your knee while keeping hips/pelvis level. When foot touches ground, straighten knee and return to starting position. Control knee, do not allow knee collapse. Keep knee behind toes. OSU Sports Medicine sportsmedicine.osu.edu 11 Consider: • No crunches, no sit-ups (no hip flexor dominant/lower abdominal leg lowering) • Resistance training: Caution loading equipment and machines. Limit carrying weights or twisting and pivoting on hip during exercise setup/preparation. Utilize preloaded upper body circuit machines early in phase • Cardio: Elliptical/bike/swimming with pull buoy. Add resistance to upright bike at 6 weeks. Begin easy skating at week 8 o Discuss duration/volume with physical therapist or physician • Avoid walking on treadmill Criteria to Progress to Phase III • Ability to complete all Phase II exercises without increase in pain, joint effusion, muscle irritation • Demonstrate full pain-free PROM with minimal hip flexion AROM “pinching” at 115 o • Full weight-bearing as tolerated – able to ambulate 15 minutes without fatigue or pain and without compensatory pattern or pain, no use of assistive devices OSU Sports Medicine sportsmedicine.osu.edu 12 Hip Arthroscopy Rehabilitation Protocol Phase III: 8 – 12 Weeks Avoid knee valgus positioning with all exercises. (Knee valgus is when your knees fall inwards towards the middle of your body as compared to the ankle position.) Keep knees BEHIND toes with all exercises. Mobility / Flexibility Exercises: • • Continue stretches from Phase I and Phase II as needed Continue to Thomas position for stretching (hip flexor, quads) Standing IT band stretch • Walking spiderman stretch • Manual AP joint mobilizations, manual long axis distraction • Continue supine active FABER stretches • Prone quad stretch • Continue scar tissue mobilizations – by PT and patient • OSU Sports Medicine sportsmedicine.osu.edu 13 Strengthening/Stability • Three position squats Position feet parallel to each other, shoulder-width apart. Now stagger your stance so your surgery foot is in front of the non-surgery foot and feet are shoulder width apart (the farther the stagger distance, the increased difficulty of exercise). Shift more bodyweight to posterior leg. Repeat with legs switched. Band Hip Flexor Progression Start in supine position with feet supported by ball and band around foot. Pull back on band, bringing knee toward hip. Stop once knee is above hip. Avoid excessive flexion or any pinching in hip. Progress to feet unsupported then to bridge position on ball. OSU Sports Medicine sportsmedicine.osu.edu 14 • Walking lunges Step forward with one leg in front, feet shoulder-width apart, and bend both knees to lower pelvis toward the floor. Straighten knees and step forward to advance other leg in front. You should be making forward progress. Repeat across the length of room. Be sure not to lower past any “pinch” pain. Progress to walking lunges with rotation – can add weight as able without increased pain or pinch symptoms. • Reverse lunge with X chop Posterior leg elevated on surface ~1-2 feet high (low plinth, couch seat). Hold a 1-2 pound weight (medicine ball) in hands. With both knees slightly bent and arms starting at one shoulder, chop down moving weight to opposite hip. Increase knee bending as you chop down. Repeat 10 times. Then, keeping legs in same position, switch starting position of arms to begin at opposite shoulder and repeat 10 times. You’ve made an “X” with arm chops. Switch legs and make an “X” with the arm chop again. OSU Sports Medicine sportsmedicine.osu.edu 15 • Sidesteps with X chop Progression of lateral ambulation: When going to the right, start with medicine ball at right shoulder and chop to left hip. Repeat downward chop with each left leg sidestep. Return ball to right shoulder with each sideways right step. Repeat with the opposite chop on your return to the start position. Avoid sideways trunk lean. • Single leg squats with chair taps Single leg squat tapping your buttock to a chair. Do not put any weight on the seat of the chair – it’s just a tap. • Sport cord walking Walk against resistance in all four directions – forward, sideways and backward. Maintain end resistance for a period of time, starting with 15 seconds and increasing by 5 seconds as able. OSU Sports Medicine sportsmedicine.osu.edu 16 • Single leg balance (advanced) Plyometrics (10 – 12 Weeks) All landings should be performed quietly and controlled, with knees behind toes and no knee valgus. Discontinue and return to strengthening exercises if pain increases with any plyometric activity. Shuttle • Double leg (DL) hops Begin with minimal resistance, as this is one of your first plyometric exercises. Push off footplate and land with equal weight on both legs. Land with feet shoulder-width apart, knees behind toes and no valgus knee positioning. Repeat (slowly and with control) for 15 seconds before stopping. Only progress to jogging and hops with rotation if no pain with DL hops. OSU Sports Medicine sportsmedicine.osu.edu 17 • DL hops with rotation Same as DL hops but rotate hips and pelvis so both feet point about 45o to the side with landing. Rotate hips to the right for first landing, 45o to the left for the second landing. Repeat (slowly and with control) for 15 seconds before stopping. • Single leg (SL) hops and jogging SL hops: Begin with minimal resistance. Repeat (slowly and with control) for 15 seconds before stopping. Only trial jogging and hops with rotation if there is no pain. Jogging: With same minimal resistance, alternate SL landings on foot plate. Repeat (slowly and with control) for 15 seconds before stopping. • DL mini hops in place Land with feet shoulder-width apart. Repeat for 15 seconds before stopping. Consider: • • • • May add crunches and sit-ups now if there is NO pinch feeling in the hips and no pain Resistance Training: Caution adding weight to exercises. Hand weights may be used if no pain or “pinch” is felt with exercises using body weight. Slow gradual return to back squat with barbell – caution with racking and unracking weights Increase the depth of squats and lunges as able but avoid any “pinch” feeling in the hip Cardio: Continue elliptical/bike/swimming now without pull buoy o Discuss duration/volume with physical therapist or Dr. Thomas Ellis Criteria to Progress to Phase IV • • Ability to complete all Phase III exercises without increase in pain, join effusion, muscular irritation Demonstrate full pain-free AROM without hip “pinching” OSU Sports Medicine sportsmedicine.osu.edu 18 Hip Arthroscopy Rehabilitation Protocol Phase IV: 12-16 weeks Continue emphasis on proper landing mechanics as before. Do not continue if plyometrics exercises cause increased pain – return to strengthening program. Mobility/Flexibility Exercises • Seated FABER stretches • Inch worms OSU Sports Medicine sportsmedicine.osu.edu 19 • Hurdle steps • Walking spiderman stretch Dynamic Strengthening and Stability • Hop ups DL hop up to 2-inch box – soft, quiet landing with good knee position. Progress to 4-inch box. Trial SL if not painful and with proper mechanics. • Hop downs DL hop down from 2-inch box to floor. Remember important landing mechanics. Progress to 4-inch box. Trial SL if not painful and with proper mechanics. OSU Sports Medicine sportsmedicine.osu.edu 20 • DL line jumps Jump forward across the room for distance – but note that control and proper landing mechanics are more important than distance itself. Be sure each landing is quiet and controlled before beginning next jump. • SL line jumps Jump forward across the room for distance – but note that control and proper landing mechanics are more important than distance itself. Be sure each landing is quiet and controlled before beginning next jump. First alternate legs – jump from R to L to R to L. Then continue on same leg – jump from R to R to R. • 3-way hop drill (DL first and trial SL) o Perform small DL hops forward and backward over line for 15 seconds Remember soft and quiet landings! o Perform small DL hops sideways back and forth over line for 15 seconds o If no pain with above, perform small DL rotational hops (no line needed) for 15 seconds o Keep feet shoulder-width apart and maintain proper landing mechanics before trial of SL hops • 3-way jog matrix o Slowly jog forward and then backpedal to return o Repeat down and back with side shuffling o Repeat with carioca • Agility ladder drills • Begin walk/jog program after 12 weeks if able to complete above exercises without pain/pinch Criteria to progress to walk/jog program: o 20 heel touches o Ambulation with symmetrical gait o No weight shifts with squatting o No pain with SL hopping Consider: • Cardio: Continue elliptical/bike/swimming now without pull buoy Discuss duration/volume with physical therapist or physician Return to Sport Criteria: • • • • No signs of FAI with clinical testing 90% on Hip Outcome Score (ADL 68/76; Sport 32/36) or 90% on Global Rating Scale <10% side to side difference with: Single leg hop Single leg triple hop No compensation with functional movements (e.g. pelvic drop, knee valgus, excessive anterior weight shift) OSU Sports Medicine sportsmedicine.osu.edu 21