Initiation of labor
advertisement

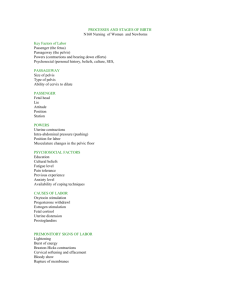
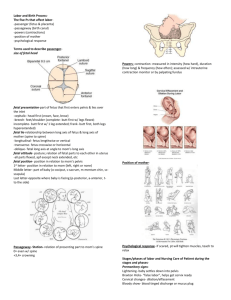
Normal labor Labor is described as the process by which the fetus, placenta and membranes are expelled through the birth canal. Normal labor occurs at term and is spontaneous in onset with the fetus presenting by the vertex. The process is completed within 18 hours and no complications arise. Initiation of labor: The exact mechanism that initiates labor is unknown. Theories include the following: 1. Uterine stretch theory: uterus becomes stretched, pressure increase causing physiologic changes that initiate labor. stretching causes a release of prostaglandins. 2. As pregnancy advances, the uterus becomes more sensitive to oxytocin (pressure on cervix stimulate production of oxytocin). 3. As pregnancy advances, progesterone is less effective in controlling rhythmic uterine contractions that occur normally throughout pregnancy. 4. There is increased production of prostaglandins by fetal membranes and uterine deciduas as pregnancy advances. 5. In later pregnancy, the fetus produces increased levels of cortisone which inhibit progesterone production from the placenta. 6. Placental aging and deterioration triggers the initiation of contractions. General terms: 1. Lie: a comparison of the long axis of the fetus with the long axis of the mother. Fetal lie is either, longitudinal, transverse or oblique. In longitudinal lie either the fetal head presents or the buttocks present. In transverse lie, the shoulders present. 2. Presentation: the part of the fetus deepest in the birth canal. Presentation may be vertex, face, brow, breech or shoulder. 3. Presenting part: portion of the fetus deepest in the birth canal and felt on vaginal examination. 4. Attitude: relationship of fetal parts to each other (normal flexion). 5. Position: Position refers to the location of a fixed reference point on the fetal presenting part in relation to a specific quadrant of the maternal pelvis. The presenting part can be right anterior, left anterior, right posterior, and left posterior. These four quadrants designate whether the presenting part is directed toward the front, back, right, or left of the passageway. It is the relationship of landmark on the fetal presenting part to the front (anterior = A) back (posterior = P) or side (transverse = T) of the mothers pelvis. Landmarks on the fetal presenting parts include head = occiput (O) buttocks = sacrum (S), shoulder = scapula or acromion (A), face = chin of mentum (M). Example: a fetus presenting by the vertex with his occipit on the left anterior part of the woman’s pelvis would have his presentation and position described as LOA or lift occiput anterior. Factors affecting labor: • Powers (physiological forces) • Passageway (maternal pelvis) • Passenger (fetus and placenta) • Passageway _ Passenger and their relationship (engagement, attitude, position) • Psychosocial influences (previous experiences, emotional status) Successful labor and delivery depend on adequate pelvic dimensions, adequate fetal dimensions, presentation and adequate uterine contractions. A. Pelvic dimensions: 1. Adequate pelvic inlet. AP diameter, normal shape. 2. Adequate midpelvis: Ischia spines don’t protrude into bony canal. 3. Adequate outlet: adequate distance between tubrosities and coccyx. B. Fetal dimensions: Important fetal dimensions influenced by fetal size, posture, lie, and presentation. Fetal position is also an important factor in successful labor. C. Uterine contractions: 1. Uterine contractions are involuntary, occurring at regular intervals and having adequate intensity. 2. During uterine contractions, the active upper portion becomes thicker, while the lower uterine segment stretches and becomes thinner. True and false labor contractions True labor contractions false labor contractions 1. Result in progressive Do not result in progressive cervical dilation and cervical effacement. 2. Occur at dilation and effacement. regular Occur at irregular intervals. intervals. 3. Intervals between Intervals remain the same or contractions decrease. 4. Intensity increases. increase. Intensity decrease or remains the same. 5. Location mainly in back Location mainly in groin and abdomen. and abdomen. 6. Generally intensified by Generally walking. walking. unaffected by 7. Not affected by mild Generally relived by mild sedation. sedation. 8. Dilation and effacement There is no change in the cervix. of the cervix are progressive. Events preliminary to labor (Signs and symptoms of labor): Pre-labor is the term given to the last few weeks of pregnancy during which time a number of changes occurring. 1. Lightening, the setting of the fetus in the lower uterine segment occurs 2-3 weeks before the onset of labor (38th) in the primigravida and later during labor in the multigravida. a. The woman’s breathing becomes easier as the fetus falls away from the diaphragm. b. Lordosis of the spine is increased, walking is more difficult because the pelvic joints are more mobile and relaxed, leg cramping may increase. Backache may increase. c. Frequency of micturation occurs because of the pressure on the bladder. 2. Vaginal secretions may increase. 3. Mucus plug is discharged from the cervix along with a small amount of blood from surrounding capillaries, referred as SHOW (bloody show). Its presence often indicates that labor will begin within 24 to 48 hours. 4. Taking up of the cervix. The cervix softens (“cervical ripening”), stretches, and thins, and eventually is taken up into the lower segment of the uterus. This softening and thinning is called cervical effacement 5. False labor contractions; Braxton-Hicks contractions may occur q 10-20 minutes. 6. Membranes may rupture, only 12% have spontaneous ROM, otherwise amniotomy. 7. In addition to some other signs; energy spurt, wt loss (.5-1.5kg due to fluid loss), and GI disturbance. Stages of labor 1. The 1st stage is that of dilation of the cervix. It begins with regular rhythmic contractions and is complete when the cervix is fully dilated 10 cm (takes most of the time). It consists of 3 phases; latent, active, and transition. 2. The 2nd stage of labor is the expulsion of the fetus. It begins when the cervix is fully dilated and is completed when the baby is completely born. 3. The 3rd stage of labor includes separation and expulsion of placenta and membranes. It lasts from the birth of the baby until the placenta and the membranes have been expelled. (about half an hour) 4. The 4th stage lasts from delivery of the placenta until the postpartum condition of the woman has become stabilized “usually 1-2 hour after delivery” Note: the 1st stage consists of 3 phases: a. Latent phase: cervical dilation is 0-3 cm Begins with the establishment of regular contractions (labor pains). Labor pains are often initially felt as sensations similar to painful menstrual cramping and are usually accompanied by low back pain. Contractions during this phase are typically about 5 minutes apart, last 30 to 45 seconds, and are considered to be mild. Usually, woman is excited about labor and chatty. It takes up to 10-14 hours. b. The active phase of labor; a cervical dilation is 47 cm. It is characterized by more active contractions. The contractions become more frequent (every 3 to 5 minutes), last longer (60 seconds), and are of a moderate to strong intensity. Cervical dilation during this phase advances more quickly as the contractions are often more efficient. While the length of the active phase is variable, nulliparous women generally progress at an average speed of 1 cm of dilation per hour and multiparas at 1.5 cm of cervical dilation per hour. c. Transitional phase: cervical dilation is 7-10 cm The transition phase is the most intense phase of labor. Transition is characterized by frequent, strong contractions that occur every 2 to 3 minutes and last 60 to 90 seconds on average. Other sensations that a woman may feel during transition include rectal pressure, an increased urge to bear down, an increase in bloody show, and spontaneous rupture of the membranes (if they have not already ruptured). Mechanism of labor If the woman’s pelvis is adequate, size and position of the fetus are adequate and uterine contractions are regular and of adequate intensity, the fetus will move through the birth canal. The position and rotational changes of the fetus as he/she moves down the birth canal will be affected by resistance offered by the woman’s bony pelvis, cervix and surrounding tissues A. Engagement: When biparietal diameter of fetal head has passed through pelvic inlet. 1. Primigravida: occurs up to 2 weeks before onset of labor 2. Multigravida: usually occurs with onset of labor. 3. Since biparietal diameter of fetal head and AP diameter is narrowest of pelvic inlet, the fetal head usually enters pelvis in a transverse position. The fetal head enters the maternal inlet in the occiput transverse or the oblique position because the pelvic inlet is widest from side to side. B. Descent: Occurs throughout labor and is essential for rotations of the fetus prior to birth: 1. Accomplished by force of uterine contractions on fetal portion in funds, during second stage of labor the bearing down increases intra-abdominal pressure thus augmenting effects of uterine contractions. 2. Degree of descent described as: a. Floating: presenting part is not engaged in pelvic inlet. b. Fixed presenting part has entered pelvis c. Engagement: presenting part has passed pelvic inlet d. Station O: presenting part has reached the level of ischial spine e. Stations (-1,-2,-3,-4) presenting part in 1,2,3,4 cm above the level of ischial spine. f. Stations (+1, +2, +3, +4) presenting part in 1, 2, 3, 4 cm below the level of ischial spine. A station of +4 indicates that presenting part is on pelvic floor. C. Flexion Resistance to descent causes head to flex so that the chin is close to the chest. This cause the smallest fetal head diameter, subocciputobregmatic (9.5 cm) to present through the canal. D. Internal rotation: In accommodating to the birth canal, the fetal occiput rotates interiorly from its original position toward the symphysis pubis. E. Extension: As the fetal head descends further, it meets resistance from the perineal muscles and is forced to extend. The fetal head becomes visible at the vulvovaginal ring. Its largest diameter is encircled (crowing) and the head then emerges from the vagina. The head is born in extension as the occiput slides under the symphysis and the face is directed toward the rectum. The fetal brow, nose, and chin then emerge. F. External rotation: When the head emerged, the shoulder are undergoing internal rotation to accommodate to the birth canal, the head now born, rotates as the shoulders undergo the internal rotation. G. Expulsion Following delivery of the infant’s head and internal rotation of the shoulder, the anterior shoulder rest beneath the symphonies pubis. The posterior shoulder is born followed by the anterior shoulder and the rest o the body.