Behavioral Health Compliance Solutions LLC documentation training
advertisement

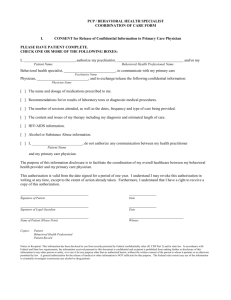
S BHC Behavioral Health Compliance Solutions, LLC Behavioral Health Medicaid Training 7 AAC 135 S BHC Staff Qualifications Behavioral Health Medicaid Training 7 AAC 135 Staff Qualifications Program Staff •Program Staff are professionals who render behavioral health services directly to a recipient. •Required staff qualifications depend on the service category. •Service Categories are –Clinic –Rehabilitation –Residential –Detoxification –Day Treatment 3 Staff Qualifications Staff Types •Substance Use Disorder Counselor •Behavioral Health Clinical Associate -includes Peer Support Specialists •Mental Health Professional Clinician •Directing Clinician 4 Staff Qualifications Behavioral Health Clinical Associate •May have less than a master’s degree in psychology, social work, counseling, or a related field with specialization or experience in providing rehabilitation services to recipients with severe behavioral health conditions. •Responsibilities may include a provision of psychosocial evaluation, education related to a recipient’s behavioral health condition, encouraging and coaching, counseling, and teaching of needed life skills. •Works within the scope of the their training, experience, and education. 5 Staff Qualifications Substance Use Disorder Counselor •Subject to the limits of the their education, training, and experience. They may provide behavioral health rehabilitation services with a focus on the treatment of substance use disorders, while working for a community behavioral health services provider. 6 Staff Qualifications Mental Health Professional Clinician • Working for a community behavioral health services provider; • Performing limited behavioral health services that are within field of expertise; • Not working in a capacity that requires licensure under AS 08; and • Has a master's degree or more advanced degree in psychology, counseling, child guidance, community mental health, marriage and family therapy, social work, or nursing; Note: there are licensure requirements for mental health professional clinicians that are not working for a community behavioral health service provider 7 Staff Qualifications Directing Clinician •A substance use disorder counselor or mental health professional clinician working within the scope of their education, training, and experience who, with respect to the recipient’s treatment plan: –Develops or oversees the development of the plan –Periodically reviews and revises the plan as needed –Signs the plan each time a change is made to the plan –Monitors and supervises the delivery of all services identified in the plan 8 Staff Qualifications Directing Clinician • By signing a treatment plan, a directing clinician attests that (in their professional judgment) the services prescribed in the plan are appropriate to the recipient’s needs, delivered at an adequate skill level, and are achieving treatment goals. • Responsible for monitoring recipients’ care across all programs within an agency as identified on a treatment plan. • May bill Medicaid for 1hr per week/per recipient of case management services for the monitoring by direct observation the delivery of services as those services are provided to the recipient 9 Staff Qualifications Clinic Services Staff Qualifications Integrated assessments Mental health assessments Psychotherapy Psychological testing and evaluation Short-term crisis intervention Mental Health Professional Clinician Psychiatric assessment Physician, Physician Assistant, Advance Nurse Practitioner Pharmacologic management Physician, Physician Assistant, Advance Nurse Practitioner with prescriptive authority 10 Staff Qualifications Rehabilitation Services AST Screening and Brief Intervention (SBIRT) Client Status Review (CSR) Substance Abuse Assessment Case Management Comprehensive Community Support Therapeutic Behavioral Health Recipient Support Daily Behavioral Health Rehabilitation Day Treatment for Children Facilitation of Telemedicine BH Tx Plan Rvw for Methadone Recipient Staff Qualifications Behavioral Health Clinical Associate Substance Use Disorder Counselor 11 Staff Qualifications Rehabilitation Services Staff Qualifications Short-Term Crisis Stabilization Behavioral Health Clinical Associate (BHCA), Substance Use Disorder Counselor (SUDC) Note: If the BHCA or SUDC is unable to resolve the crisis, a mental health professional clinician may assume responsibility for the case and begin providing short-term crisis intervention services. 12 Staff Qualifications Rehabilitation Services Staff Qualifications Short-Term Crisis Stabilization Behavioral Health Clinical Associate (BHCA) Substance Use Disorder Counselor (SUDC) Note: If the BHCA or SUDC is unable to resolve the crisis, a mental health professional clinician may assume responsibility for the case and begin providing short-term crisis intervention services. Medication Administration, On/ Off Site physician, physician assistant, advanced nurse practitioner, registered nurse, or licensed practical nurse. 13 Staff Qualifications Rehabilitation Services Staff Qualifications Peer Support Services You must be a behavioral health clinical associate or substance use disorder counselor. You must have experienced behavioral health issues in your life or within your family. Note: Must be supervised by a mental health clinician, determined by your employer to be competent to supervise peer support. 14 Staff Qualifications Peer Support Specialists •Peer support staff must be employed by the Provider as a behavioral health associate. •Minimum age is determined by labor laws for employment and agency policy. •Good practice indicates that all employees, and particularly peer support staff should be aware of the prohibition of dual relationships with clients and maintain appropriate boundaries. 15 S BHC Recipient Eligibility Behavioral Health Medicaid Training 7 AAC 135 Recipient Eligibility There are five categories of recipient eligibility for Medicaid services. Recipients who are eligible to receive behavioral health clinic services include: 1) A child experiencing an emotional disturbance– a recipient is under the age of 21 who is experiencing on non-persistent mental, emotional, or behavioral health disorder that: a) Is identified and diagnosed during a professional behavioral health assessment; and b) Is not the result of an intellectual, physical, or sensory deficit 2) An adult experiencing an emotional disturbance – a recipient is 21 years of age or older who is experiencing on non-persistent mental, emotional, or behavioral disorder that: a) Is identified and diagnosed during a professional behavioral health assessment; and b) Is not the result of an intellectual, physical, or sensory deficit 17 Recipient Eligibility Behavioral health clinic services 3) A child or adult experiencing a substance use disorder – a recipient of any age experiencing a disorder that is identified by a diagnostic code found in the American psychiatric Association’s diagnostic and statistical manual of mental disorders that is related to: a) alcohol, amphetamine, or similar acting sympathomimetics; b) cannabis, cocaine, hallucinogens, inhalants, nicotine or opioids c) analogues of phencyclidine (PCP) or similar arylcyclohexylamines;or d) sedatives, hypnotics, or anxiolytics 18 Recipient Eligibility Behavioral health clinic services 4) A child experiencing a severe emotional disturbance– a recipient is under the age of 21 who: a) has or had a diagnosable mental, emotional, or behavioral health disorder any time in the past year that resulted it in a functional impairment (that is not a result of response to stressful situations) which substantially interferes with the child’s role functioning in family, school, or community activities as indicated by a global assessment of functioning score of 50 or less b) exhibits specific mental, emotional, or behavioral disorders that i) place them at imminent risk for out of home placement ii) place the individual at imminent risk for being placed in the custody of the Division of Juvenile Justice iii) have resulted in the individual being placed in the protective custody of the Office of Children’s Services 19 Recipient Eligibility Behavioral health clinic services 5) An adult experiencing a serious mental illness– a recipient that is 21 years of age or older who a) has or had a diagnosable mental, emotional, or behavioral health disorder any time in the past year that resulted it in a functional impairment (that is not a result of response to stressful situations) which substantially interferes with or limits one or more life activities including i) basic daily living skills ii) instrumental living skills such as managing money iii) functioning and social, family, or vocational/educational contexts 20 Recipient Eligibility Three of the five categories of recipient eligibility for Medicaid service are eligible to receive behavioral health rehabilitation services including: 1) A child or adult experiencing a substance use disorder 2) A child experiencing a severe emotional disturbance 3) An adult experiencing a serious mental illness 21 S BHC Clinical Documentation Requirements Behavioral Health Medicaid Training 7 AAC 135 Clinical Documentation Requirements Community behavioral health services providers (CBHS) “must maintain a clinical record for each recipient in accordance with the standards used for the Medicaid Program” [7 AAC 70.100(a)(6)] 7 AAC 135.130 Clinical Record A CBHS must maintain a clinical record that contains the following: –Screening using AST –Client Status Review –Behavioral Health Assessment –Treatment Plan –Progress Notes (for each service / each day service provided) 23 Clinical Documentation Requirements •A Medicaid provider must retain a record of service for each recipient according to requirements noted in 7 AAC 105.230 •To document active treatment a Medicaid provider must describe or list active interventions provided to a recipient •All changes to assessments and treatment plans must be noted in the recipient’s clinical record 24 Clinical Documentation Requirements •A provider shall maintain accurate records necessary to support the services for which the provider requests payment, and ensures that the provider’s staff meet the requirements of this section 7 AAC 105.230 •A provider’s record must identify all the following: –Recipient name –Specific services provided –Extent of each service provided –Date of service –Individual who provided service 25 Clinical Documentation Requirements • A Provider shall maintain a clinical record for each recipient in accordance with professional standards applicable to the provider that includes: –Recipient’s diagnosis –Medical need for each service –Prescribed Service or Plan of Care –List of prescription drugs –Stop and start times for time-based codes –Progress notes of services provided signed / dated by person who provided service 26 Clinical Documentation Requirements Behavioral Health Screening Alaska Screening Tool (AST) •A CBHS must complete the AST for each new or returning recipient of behavioral health services before a behavioral health assessment is conducted [7 AAC 135.100(a)] •AST does NOT have to be completed for recipients receiving: –SBIRT –Short-term Crisis Intervention / Crisis Stabilization •AST is a reimbursable Medicaid service [7 AAC 145.580] 27 Clinical Documentation Requirements Behavioral Health Screening Client Status Review The Department will pay a CBHS for completing a client status review with the client present if: 1. it is used as relevant clinical information concurrent with an initial Behavioral Health Assessment 2. Conducted Every 90-135 Days 3. Conducted at discharge from treatment [7 AAC 135.100(b)] 4. Administered using the Dept. CSR Form 28 Clinical Documentation Requirements Behavioral Health Screening Client Status Review 6. Documented in the clinical record 7. CSR data reported to Department 8. Used to help determine recipient’s level of functioning 9. Used by Directing Clinician to: a. Measure Treatment Outcomes b. Make Treatment Decisions c. Revise Treatment Plan 29 Clinical Documentation Requirements Professional Behavioral Health Assessments If a behavioral health screening (AST), or a referral by a court or other agency, has identified an individual suspected of having a behavioral health disorder that could require behavioral health services, the Dept. will pay a CBHS for one of the following behavioral health intake assessments [7 AAC 135.110]: 1.Mental Health intake assessment 2.Substance Use intake assessment 3.Integrated MH and Substance Use intake assessment 4.Psychiatric Assessment (used as Intake Assessment) 30 Clinical Documentation Requirements Professional Behavioral Health Assessments Mental Health Intake Assessment • Are conducted by a Mental Health Professional Clinician for the purpose of determining: –Recipient’s Mental Status, Social & Medical Histories –Nature & Severity of Mental Health Disorder(s) –Complete DSM Multi-axial Diagnosis 31 Clinical Documentation Requirements Professional Behavioral Health Assessments Elements of ALL Behavioral Health Assessments: • Finalizes in a written report • Documents that results of AST and CSR were reviewed and considered • Documents information on functional impairment • Documents treatment recommendations that form basis of a treatment plan • Identifies the need for Recipient Support Services (if appropriate) that includes Hx of violence/need for vigilance & location/frequency of RSS • Is updated as new information becomes available 32 Clinical Documentation Requirements Professional Behavioral Health Assessments Substance Use Intake Assessment •Conducted by a Substance Use Disorder Counselor, Social Worker, or other Qualified Staff Member working within the scope of their authority, training, and job description •Conducted to Determine: –If recipient has substance use disorder –Nature & severity of disorder –Correct diagnosis 33 Clinical Documentation Requirements Professional Behavioral Health Assessments Integrated Mental Health and Substance Use Intake Assessment •Conducted by a Mental Health Professional Clinician (able to diagnose BOTH Mental Health & Substance Use Disorders) •Documents –All Requirements for Mental Health Intake Assessment –All Requirements for Substance Use Intake Assessment 34 Clinical Documentation Requirements Professional Behavioral Health Assessments Psychiatric Assessments • The department will pay a community behavioral health services provider for a psychiatric assessment that is to serve as the professional behavioral health assessment if the recipient's condition indicates the need for a more intensive assessment, including an assessment to evaluate the need for medication. [7 AAC 135.110(f)] • A psychiatric assessment must be conducted by a licensed practitioner working within the scope of their education, training, and experience, if the provider has prescriptive authority, and if the provider is enrolled under 7 AAC 120.100(c) as a dispensing provider: •Physician •Physician Assistant •Advanced Nurse Practitioner 35 Clinical Documentation Requirements Professional Behavioral Health Assessments Psychiatric Assessments •2 Types of Psychiatric Assessments: 1.Psychiatric Assessment Interview 2.Interactive Psychiatric Assessment (uses equipment and devices) •Both Types must include: – Review of medical & psychiatric history or problem; – Relevant recipient history; – Mental Status Examination; –Complete Multi-axial DSM diagnosis –Listing of identified psychiatric problems 36 Clinical Documentation Requirements Professional Behavioral Health Assessments Psychological Testing and Evaluation The Dept. will pay a CBHS, or psychologist for psychological testing and evaluation to assist in the diagnosis and treatment of mental and emotional disorders [7 AAC 135.110(g)] •Psychological testing and evaluation must be conducted by a Mental Health Professional Clinician working within the scope of their education, training, and experience. •Psychological Testing and Evaluation includes: –assessment of functional capabilities –administration of standardized psychological tests –interpretation of findings 37 Clinical Documentation Requirements Behavioral Health Treatment Plan • Based on Behavioral Health Assessment recommendations • Developed with recipient or –Recipient’s representative if recipient 18 & older –Treatment team if recipient is under 18 • Supervised by Directing Clinician • Remains current based on Client Status Review conducted every 90-135 days 38 Clinical Documentation Requirements Behavioral Health Treatment Plan Documentation Requirements [7 AAC 135.130(a)(7)]: •Recipient’s identifying information •Date that plan will be implemented •Treatment goals related to assessment findings •Services & interventions employed to address goals •Frequency and duration of services & interventions •Name, signature & credentials of Directing Clinician •Signature of recipient or recipient’s representative 39 Clinical Documentation Requirements Behavioral Health Treatment Plan Treatment Team for Recipient under 18 MUST include: •Recipient •Recipient’s Family Members (including parents, guardians, or others providing general oversight of Recipient) •OCS Staff Member if Recipient in State Custody •DJJ Staff Member if Recipient in DJJ Custody •Directing Clinician •Case Manager, if Recipient is SED 40 Clinical Documentation Requirements Behavioral Health Treatment Plan Treatment Team for Recipient under 18 MAY include: •Representative(s) from Foster Care, Residential Child Care, or Institutional Care •Representative(s) from Recipient's Educational System 41 Clinical Documentation Requirements Behavioral Health Treatment Plan ALL treatment team members shall: • Attend team meetings In-person or by telephone • Be involved in team decisions unless the clinical record documents – (1 ) that participation by Recipient or other Individual involved with Recipient care is detrimental to Recipient's well-being (2) family members, school district employees, or government agency employees refuse or unable to participate after provider's responsible efforts to encourage participation or (3) weather, illness, or other circumstances beyond member's control prohibits participation 42 Clinical Documentation Requirements Behavioral Health Treatment Plan Directing Clinician- Substance Use Disorder Counselor or Mental Health Professional Clinician working within the scope of their education, training, and experience who, with respect to the recipient’s Treatment Plan: 1.Develops or oversees treatment planning process 2.Periodically reviews & revises plan 3.Signs plan each time plan is changed 4.Monitors & directs delivery of services identified in plan • By signing treatment plan, directing clinicians attest (in their professional judgment) that services prescribed are: • Appropriate to recipient’s needs • Delivered at adequate skill level • Achieving treatment goals 43 Clinical Documentation Requirements Progress Notes Requirements: [7AAC 135.130(a)(8)] •Progress note is written for each service/each day service is provided •Date service was provided •Duration of service expressed in service units or clock time •Description of “active treatment” provided •Treatment goals that service targeted •Description of recipient’s progress toward treatment goals •Name, signature & credentials of individual who rendered service 44 Clinical Documentation Requirements Short-term Crisis Intervention Provided by a Mental Health Professional Clinician who: 1.Conducts initial assessment to determine: a. Nature of Crisis b. Recipient's Mental, Emotional, & Behavioral Status c. Recipient's overall Functioning related to Crisis 2. Develops Crisis Intervention Plan a. Uses Dept. Form 3.Directs ALL Services (except Pharmacologic Management Services) 45 Clinical Documentation Requirements Short-term Crisis Intervention Clinician may order & deliver ANY Medically Necessary and Clinically Appropriate Behavioral Health Clinic or Rehabilitation Service or intervention to: • Reduce Symptoms • Prevent Harm • Prevent further Relapse or Deterioration • Stabilize the Recipient 46 Clinical Documentation Requirements Short-term Crisis Intervention ST Crisis Intervention Plan MUST Contain: •Treatment goals derived from assessment •Description of Medically Necessary and Clinically Appropriate Services •Documentation by individual who delivered service 47 Clinical Documentation Requirements Short-term Crisis Stabilization Provided by a Substance Use Disorder Counselor or Behavioral Health Clinical Associate who: 1.Conducts initial assessment of recipient's overall functioning in relation to crisis 2.Develops Short-term Crisis Stabilization Plan 3.Orders ANY Medically Necessary and Clinically Appropriate Rehabilitation Service to return recipient to level of functioning before crisis occurred 4.Documents Assessment, Stabilization Plan, and Services on Dept. Form 48 Clinical Documentation Requirements Short-term Crisis Stabilization ST Crisis Stabilization includes: • Individual or Family Counseling • Individual or Family Training & Education related to Crisis and Preventing Future Crisis • Monitoring Recipient for Safety Purposes • Any other Rehab Service ST Crisis Stabilization May be Provided: • Any Appropriate Outpatient or Community Setting • Premises of CBHS • Crisis Respite Facility • Recipient’s Residence, Workplace or School • Documented by Individual who Provides the Service 49 Clinical Documentation Requirements Short-term Crisis Stabilization ST Crisis Stabilization includes: • Individual or Family Counseling • Individual or Family Training & Education related to crisis and preventing future crisis • Monitoring recipient for safety purposes • Any other Rehab Service ST Crisis Stabilization may be provided: • Any appropriate outpatient or community setting • On the premises of CBHS • Crisis Respite Facility • Recipient’s residence, workplace or school • Documented by individual who provides the service 50 S BHC Covered Services Service Authorization Medical Assistance Billing & Payment Post-Payment Activities (Appeals, Audits) Behavioral Health Medicaid Training 7 AAC 135 Covered Services, Service Authorization, Medical Assistance Billing & Payment, Post-Payment Activities (Appeals, Audits) Refer to Alaska Medical Assistance Program Policies and Claim Billing Procedures Manuals •Section I, Part B – Service Detail Sheets – –Service Definition/Description – from regulations –Service Code/Code Set Description – from national code sets •Current Procedural Terminology – CPT •Health Care Procedure Coding System – HCPCS •Section I, Appendix I-D – Claims Billing & Payment Information –List of Procedure Codes & Modifiers, Adult/Child Coverage, Brief Descriptions, Unit Values, Payment Rates, Service Limits, Program Approval Categories 52 Covered Services, Service Authorization, Medical Assistance Billing & Payment, Post-Payment Activities (Appeals, Audits) Coverage EXCLUSIONS & LIMITATIONS •EXCLUSIONS –Persons in the custody of Federal, State, or Local Law Enforcement (including juveniles in detention) Authority: 42 CFR 435.1009, 42 CFR 436.1005, 7 AAC 105.110 –Persons between age 22 and 65 who are residents of an Institution for Mental Diseases (IMD) Authority: 42 CFR 436.1005 •IMD is a hospital, nursing facility, or other institution of more than 16 beds that is primarily engaged in providing diagnosis, treatment, or care to patients with mental diseases –Persons of any age who are residents of a Skilled Nursing or Intermediate Care Facility (SNF/ICF) Authority: 7 AAC 140.505, 7 AAC 140.580 53 Covered Services, Service Authorization, Medical Assistance Billing & Payment, Post-Payment Activities (Appeals, Audits) Coverage EXCLUSIONS & LIMITATIONS •LIMITATIONS –Persons who are inpatients of an acute care hospital or a residential psychiatric treatment center are limited to coverage of assessment and case management services for treatment planning or preparation for transition to lower level of care within 30 days of discharge from the acute care hospital 54 Covered Services, Service Authorization, Medical Assistance Billing & Payment, Post-Payment Activities (Appeals, Audits) Service Authorization Annual Service Limits changed from CALENDAR year to STATE FISCAL year (July 1 through June 30) NEW Service Authorization request forms are available in provider manuals and via DBH and fiscal agent websites Requests are to be made in correlation with Client Status Review requirements Requests limited to a maximum of 90 to 135 days of planned services (to be submitted approximately 3 to 4 times annually) Requires signature of directing clinician ALL Requests to be submitted to the fiscal agent for capture/control and entry into Medicaid Management 55 Information System (MMIS). Covered Services, Service Authorization, Medical Assistance Billing & Payment, Post-Payment Activities (Appeals, Audits) Claims Billing - General ALL CLAIMS MUST BE FILED WITHIN 12 MONTHS OF THE DATE SERVICE • The 12-month timely filing limit applies to all claims, including those that must first be filed with a third party carrier. • Submit on paper form or electronically; complete required fields –Use Paper CMS-1500 Claim Form for Professional Services - Set B for billing behavioral health services –Use Electronic Claim Transaction (837-Professional) –Include Service Authorization number as required if services billed exceed annual service limits Ensure services are: –Performed as active treatment, documented in treatment plan, stated as a need in assessments, etc. –Performed by staff qualified 56 Covered Services, Service Authorization, Medical Assistance Billing & Payment, Post-Payment Activities (Appeals, Audits) Claims Adjudication, Editing & Response All claims submitted are processed according to program rules which will result in one of the following outcomes: • adjudicated claim (paid or denied) • reduction in payment • denial of service • in-process claims (further internal review or information needed) • pending status requiring internal staff review • additional information requested from the provider (via RTD) • Remittance Advice (RA) statement includes the claims processing details that include three-digit claims edit codes each with a unique explanation of how the claim was processed. These edit codes are listed on the Explanation of Benefit (EOB) description page of the RA and lists all EOB codes and a brief description of each code used within that specific Remittance Advice statement. • Contact the fiscal agent’s Provider Inquiry for clarification as needed 57 Covered Services, Service Authorization, Medical Assistance Billing & Payment, Post-Payment Activities (Appeals, Audits) Medical Assistance Appeals for Providers (7 AAC 105.270) REASONS for Providers to Request an Appeal –Denied or reduced claims (180 days) –Denied or reduced service authorization (180 days) –Disputed recovery of overpayment (60 days) Three Levels of Appeals –First level appeals –Second level appeals –Commissioner level appeals 58 Covered Services, Service Authorization, Medical Assistance Billing & Payment, Post-Payment Activities (Appeals, Audits) Medical Assistance Appeals for Providers (7 AAC 105.270) First Level Appeals- Fiscal Agent Must be submitted in writing within 180 days of remittance advice for claim or other notification (service authorization decision, request for recovery of funds) Appeal form is available in provider manual, include: •A copy of the Claim or Disputed Authorization Decision •A copy of the Remittance Advice Statement •Supporting Documentation •Completed Adjustment Request, if applicable •Mail to: Xerox Provider Services Unit P. O. Box 240808, Anchorage, AK 99524-0808 59 Covered Services, Service Authorization, Medical Assistance Billing & Payment, Post-Payment Activities (Appeals, Audits) Medical Assistance Appeals for Providers (7 AAC 105.270) Second Level Appeals – DBH, Must be submitted in writing to Division of Behavioral Health within 60 days of First Level Appeal Decision. Include: –Reason for Appeal including a description of the issue or decision being appealed –Copy of decision from First Level Appeal –Copy of denial or payment notice (Remittance Advice) –Copy of Original Claim –All other information and materials for consideration 60 Covered Services, Service Authorization, Medical Assistance Billing & Payment, Post-Payment Activities (Appeals, Audits) Medical Assistance Appeals for Providers (7 AAC 105.270) Commissioner Level Appeals •ONLY used to challenge/appeal adverse timely filing denials/reductions •Must be submitted in writing to the DHSS Commissioner within 60 days of Second Level Appeal decision •Include clear description of the reason for appeal (the issue or decision being appealed) 61 Covered Services, Service Authorization, Medical Assistance Billing & Payment, Post-Payment Activities (Appeals, Audits) Recommended Keys to Achieve Success in Billing/Payment: •Read and maintain your billing manual •File your license renewals •Verify recipient eligibility and/or certification/permits timely •Verify eligibility code (keep your enrollment •Verify dates of eligibility current) •Verify Third Party Liability • Ensure completion of •Verify the services you are claim forms eligible to provide •Verify procedure codes 62 Covered Services, Service Authorization, Medical Assistance Billing & Payment, Post-Payment Activities (Appeals, Audits) Recommended Keys to Achieve Success in Billing/Payment: • Document Third Party Liability payment on claim, if applicable • Include attachments as required • FILE TIMELY • RECONCILE PAYMENTS (Remittance Advice (RA) Statements) • Read and distribute RA messages • Address problems/issues promptly • Call Provider Inquiry with questions 63 Covered Services, Service Authorization, Medical Assistance Billing & Payment, Post-Payment Activities (Appeals, Audits) Alaska Medical Assistance Regulations Request for Records 7 AAC 105.240 – Request for records At the request of a DHSS representative or authorized federal, or other representative, including an employee of the Department of Law, a provider shall provide records, including financial, clinical, and other records, that relate to the provision of goods or services on behalf of a recipient: – To the person making the request at the address specified in the request – No later than the deadline specified in the request – Without charge and in the format stated in the request 64 Covered Services, Service Authorization, Medical Assistance Billing & Payment, Post-Payment Activities (Appeals, Audits) Audits • Federal Audits – – – – Department of Health and Human Services (DHHS) Office of Inspector General Department of Justice U. S. Government Accountability Office (GAO) • State Audits – – – – Department of Health and Social Services (DHSS) Department of Law Legislative Audits Fiscal Audits 65 Covered Services, Service Authorization, Medical Assistance Billing & Payment, Post-Payment Activities (Appeals, Audits) Previous Audit Findings • • • • • • • • • • • No client signature on treatment plan No treatment plan reviews to cover dates of service No documentation to match billed services Progress notes do not match service billed Duplicates of notes for the same service on a different day Units billed and documented do not match notes Duration of service is not supported by content of note No treatment plan Insufficient documentation to support units of service billed Wrong service code submitted Agency forms that contained check boxes that were unchecked and the missing information was not supported by a narrative explanation elsewhere in the note 66 Resources Alaska Medical Assistance Provider Billing Manuals • Section I: Community Behavioral Health Clinic Services, Policies and Procedures: https://medicaidalaska.com/dnld/PBM_CBHC.pdf • Section II: Professional Claims Management: https://medicaidalaska.com/dnld/PBM_Prof_Claim_Mgmt.pdf • Section III: General Program Information: https://medicaidalaska.com/dnld/PBM_Gen_Program_Info.pdf State of Alaska Division of Behavioral Health • http://dhss.alaska.gov/dbh/Pages/Resources/Regulations.aspx 67 Behavioral Health Medicaid Training 7 AAC 135 Behavioral Health Compliance Solutions, LLC Contact information • Connie Greco E-mail: cgreco@gci.net Phone: 907-522-8170 • Pam Miller E-mail: pmillerbhcs@yahoo.com Phone: 907-717-9180 Blog site address: www.bhcompliance.com Facebook page: https://www.facebook.com/pages/Behavioral-HealthCompliance-Solutions-LLC/185142004863501 68