Urinary tract obstruction & Stones

Urinary tract obstruction &
Stones
Loin pain & hematuria
Principal sites of pathology leading to loin pain
• Spinal nerve roots
• Vertebral column
• Paraspinal & lumbar muscles
• Kidneys
• Renal pelvis / ureters
• Abdominal aorta
• Pancreas
• Renal pain arises because of rapid stretching or inflammation of renal capsule
• Pain from the renal pelvis / ureter is caused by distention & excessive peristaltic contractions
• Any back / retroperitoneal structure may give rise to back pain
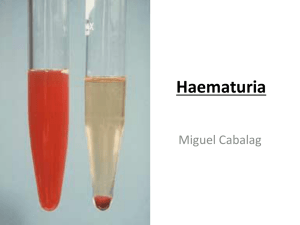
Macroscopic hematuria
• May arise from lesions anywhere within the urinary system, kidney, renal pelvis, ureter, bladder, urethra can be detected visually as red-coloured urine
• Macroscopic hematuria needs to be distinguished from
– Red discolouration of urine caused by certain dyes & some drugs
– Presence of Haem pigment : intravascular hemolysis
(Hb), rhabdomyolysis (myoglobin)
– Bleeding from outside the urinary tract; perineum, vagina
• Bleeding from the bladder or above cause uniform discoloration of urine
• Bleeding from the urethra may cause bleeding separate from the urine or mixed with urine
• Hematuria from the renal parenchyma – glomeruli or interstitium – tends to be accompanied by proteinuria, casts, & dismorphic
RBC (abnormal morphology)
• Bleeding from renal tumors or from lesions in the renal pelvis or below may be isolated or associated with pyuria – particularly with infections.
• Macroscopic hematuria from tumors are usually painless, whereas that from calculi / infection is usually associated with pain
Pyelonephritis/infections
• The formation of stone is usually the result of many metabolic and physiologic disorders contributing to stone formation
• Stones in the urinary tract are composed of crystals and matrix skeleton.
• Physical factors of stone formation
– Supersaturation of the urine with respect to a particular solute, e.g. uric acid, due to increase in excretion or decrease in urine volume. At some point spontaneous nucleation and crystal growth occur – homogenous nucleation.
– Urine pH, determines the solubility of ccompounds in the urine.
Uric acid & cystine are poorly soluble in acidic media, whereas calcium salts are poorly soluble at an alkaline pH.
– Crystalization inhibitors; normal urine contain factors that inhibit formation & growth of crystals – Mg, citrate, pyrophosphate,
TPH, glucosamine, nephrocalcin.
– Heterogenous nucleation appears to be a major mechanism in stone formation. A small crystal, e.g. uric acid, serves as a nidus on which another compound, e.g. ca-oxalate, precipitates
– Infection with urea splitting / urease producing microorganisms
Disorders causing stone disease
• Gastrointestinal disorders;
– Fat malabsorption, IBD, small bowel resection & bypass can cause decreased urinery volumes, hyperoxaluria, hyperuric-aciduria, hypocitrateuria, acidic urine.
• Hyperparathyroidism / hypercalcemia
– Causes of hypercalcemia (& hypercalciuria) are #
• Cancer, immobilization, endocrinopathies, dietary, granulomatous disease, renal, drugs
• Vit D increases Ca absorption from intestine
– Idiopathic Hypercalciuria.
• 24h urine[Ca] > 300mg/24h (men), >250mg/24h (women)
• Gout & hyperuricosuria.
– May promote Ca-oxalate stones
• Epitaxy, ca-oxalate deposits on uric acid / Na-urate crystals as nidus
• Urate in urine binds glycosamineglycans, an inhibitor of stone formation
• Uric acid promotes the degree of aggregation of precipitated crystals
– Uric acid lithiasis; elevated urinary uric acid (24h urinary uric acid), acid urine;
• Gout, myeloproliferative disorders
• Treatment: alkalinization of urine to pH 6-7 , fluids, allopurinol
• Infection with urease producing bacteria urea splitting struvite stones
– Proteus in majority; Klebsiella, Pseudomonas, Providencia, Staphylococcus,
Ureaplasma urealyticum, rarely E. coli.
– More common in patients with ileal conduits, hyperchloremic metabolic acidosis, ureteral dilatation, increased volume of residual urine, decreased renal function
• Obstruction & anatomic abnormalities
• Drugs.
– Acetazolamide causes hyperchloremic metabolic acidosis, transiently elevates urine pH, and reduces citrate excretion
– Allopurinol increases xanthine excretion and may produce xanthine stones
– Several drugs have limited urine solubility,
• May promote stone formation or are absorbed into the crystal matrix of other stone
• Triamterene, ceftriaxone, sulfonamides, bactrim, sulindac, phenazopyridine
• Other : laxatives, vit D, calcium,
• Renal tubular disorders.
– Cystinuria,
• Inherited disorder of amino acid transport,
• associated with increased urinary excretion of cystine, ornithine, lysine, & arginine
(COLA)
• Limited soloubility of cystine promotes recurrent stones, which are radioopaque, homogeneous, may assume staghorn form
• Therapy: high fluid intake, alkalinization of urine to pH 7.5 or more; reduce cystine excretion by low Na diet, D-penicillamine, trioponine, captopril (drugs with sulfhydryl)
– Distal RTA
• Alkaline urine, hypocitrateuria,hypercalciuria
– Hyperphosphaturia, causing hypophosphatemia & elevated 1,25-(OH)2D3, hypercalcemia
– Idiopathic hypercalciuria; reduced tubular reabsorption of Ca
• Enzymatic defects
– Xanthinuria. Deficiency xanthine oxidase
• Radiolucent xanthine stones
– 2,8-dihydroxyadenine.
• Deficiency adeninephosphoribosyl transferase (APRT)
• Radiolucent stones, requires infrared / crystallographic analysis
• Treatment with allopurinol
– Primary hyperoxaluria,
• Idiopathic Urolithiasis
– Majority of patients
– Risk factor profile
• Abnormally high excretion of Ca (>4mg/kg/d), uric acid, oxalate, Na
• Decrease in several inhibitory solutes
• Decreased urine volume!
• Ability of urine to inhibit agglomeration improves after treatment with alkali, which increase urinary citrate
– Excretion of citrate is decreased by systemic acidosis, depletion of kalium & magnesium, starvation acetazolamide,
– Most patients with low urinary citate have RTA, chronic diarrhea, hypokalemia, malabsorption, or high intake of animal protein
First stone episode
Dietary advice: meat, dairy, salt
Fluids; f/u 6-12 months
No growth Metabolically active
Monitor 1-2 years
Urinary risk assessment
Dietary/fluid hypercalciuria hyperuricosuria hypocitric aciduria hyperoxaluria
Factors persist
Evaluate diet Evaluate for Evaluate for
Meat, Ca, Na acidosis, RTA dietary excess
GI malabsorption
Dietary, meat GI disorders measure oxalate/ glycoliate
Treatment options
Repeat specific Reduce meat dietary fat /
Dietary advice dietary Rx & / excess oxalate restriction
Thiazides allopurinol K-Citrate B6, PO4
?thiazides
Asymptomatic No Rx
Symptomatic Acute colic: analgetics, fluids
Calcium stones Mg/NH4/PO4 Cystine (cannot Uric acid stones dissolve, or (cannot dissolve/ obstructive obstructive)
Symptomatic obstructive
Percutaneous extraction +
ESWL
Small <2cm >2cm
New stones old stones
ESWL
Often requires
Urography
Usg
ESWL Perc
<2cm >3cm ureteric stones
ESWL Perc upper1/3 lower1/3
ESWL
ESWL Extraction laser Rx
7-dehydrocholesterol Diet
Skin UV
Cholecalciferol liver
PTH
Hypophosphatemia
25-hydroxycholecalciferol kidney
Calcitriol 24,25 D
Small intestine Bone Kidney
+PTH
Increase Increase Decrease
CaHPO4 Ca & Po4 Ca & PO4 absorption release excretion
Metabolic activation of vit.D
The result is an increase in
Ca & PO4 concentration
Plasma Ca
PTH
Bone Kidney
Vit.D
Reabsorption
Phosphate Ca Calcitriol
Excretion reabsorption formation
Release of
Calcium & phosphate
Intestinal
CaHPO4 absorption
Effect of PTH on Ca & phosphate metabolism.
Net effect is increase in plasma Ca , with no change or decrease in plasma phosphate concentration
Plasma Ca [2+]
PTH
Cacitriol
Increased Ca increased Ca increased phosphate increased phosphate
From bone from intestine from bone & intestine excretion in urine
Plasma Ca increase
Plasma Phosphate unchanged
Plasma phosphate
Calcitriol
Ca from intestine
PTH
Decreased decrease increase phosphate
Ca from bone phosphate from intestine excretion in urine
Plasma [Ca] Plasma [PO4]
Slight increased increased
Increased = systemic disease
Serum [calcium] normal
Normal
Hyperuricosuria
Hyperoxaluria
No abnormality
Urinary calcium = idiopathic hypercalciuria
RTA
Laboratory investigation
• Serum electrolytes, BUN, Cr, Ca, PO4, Uric acid
• Urinalysis; microscopic exam of fresh specimen
• Urine culture
• Nitroprusside test for cystine
• Urine pH, first AM urine, under oil
• Stone analysis
• 24h urine for Cr, Ca, PO4, uric acid, Cystine, oxalate
• Radiologic studies, USG, BNO, IVP
• Special test as indicated; PTH, Thyroid, Cortisol, etc