urine sample form - Hugglescote Surgery
advertisement

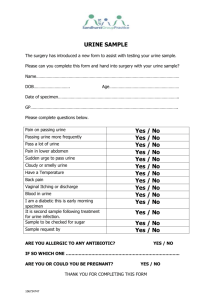
Hugglescote Surgery Partners: Dr D Woods, Dr T Gauhar Associate: Dr A Shah, Dr H Noble Practice Manager: Keleigh Atkin URINE SAMPLE FORM To be filled in by anyone handing in a urine for testing (white top bottles) Name of Patient: Date of birth: Present address of patient & contact telephone number: REASON FOR TEST Suspected urine infection Dip for blood pressure Early Morning urine for diabetes Yes Yes Yes No No No SYMPTOMS – for people with suspected urine infection only Pain on passing water Frequently passing water Pain in the lower abdomen Pain on the loin (kidney area) Blood in the urine Vaginal discharge Vaginal bleeding (eg: period) Yes Yes Yes Yes Yes Yes Yes No No No No No No No RESULTS OF URINE DIP TEST Leucocytes Nitrites Blood Protein Yes Yes Yes Yes No No No No Yes Yes Yes No No No OUTCOME OF ANALYSIS Sample sent to lab for further testing Prescription supplied Referred to GP Comments: Date of sample: T: 01530 832109 F: 01530 832553 E: TBC W: www.hugglescotesurgery.co.uk Hugglescote Surgery 151 Grange Road Coalville Leicestershire LE67 2BS