Health Quality Safety
Commission
Quality Accounts:
Sector Capability Development Workshop
Welcome
Sector Capability Development Programme
2012
PwC
Introduction to Quality Accounts
Programme overview
2012
PwC
Introduction
Over the last five years, the health environment has demanded more from its quality
information and reporting.
All District Health Boards must now be better equipped to deliver reporting that is:
Practical
Clear
Reliable
Strategically
focused
Relevant
Future
orientated
Representative
Consistent
The challenge of encouraging and enabling each health and disability service provider to
consistently report on their assessments of the quality and safety of healthcare services
provided within their organisation should not be underestimated.
The Health Quality and Safety Commission have recognised this and are providing a
development programme for all DHBs to assist in the documentation and publication of
a Quality Account.
PwC
4
The Commission & Quality Accounts
Shining a light
Lending a
hand
Quality at the
heart of
healthcare
Improvement
starts with
knowledge &
clarity
5
Introduction to Quality Accounts
Programme overview
2012
PwC
Two phased approach
The first phase of this programme was successfully completed in June 2012 with the
publication of a best practice advisory guidance manual, which provides a practical stepby-step approach to the preparation, documentation and publication of a Quality
Account.
The second phase of the programme has a stronger focus on knowledge transfer.
PwC
7
Programme objectives
To build the capability required to design, document and publish a Quality
Account within each DHB
To exchange sound, practical ideas throughout the sector on how to measure
and report on quality and safety performance
To provide a setting for deep discussion and shared learning among those
charged the design and generation of their DHB’s Quality Account
To support each DHB during the development of a Quality Account
PwC
8
What we are trying to achieve
Strategic Skills
Capability Level
Expert Skills
Operational Skills
Understanding
“I understand the Quality
Accounts programme
will be rolled out and I
am clear on what the
programme is.”
“I have been briefed and
trained on how to develop
a Quality Account and
know where to get help.”
“I am using the new ways
of working, services and
solution to its full
capability and delivering
maximum value.”
“I am further developing
my health quality
evaluation skills, in
terms of understanding
how the full capabilities
of Quality Accounts can
be used to best support
and inform my DHB and
consumer population.”
Time
PwC
9
Who we are working with
The nominated delegates for the workshops include physicians, nurses, managers, health
care leaders and other health professionals that have a role in contributing to the
development of their organisation’s Quality Account.
Group 1: Rotorua
Wed 26th September
Group 2: Auckland
Thurs 27th September
Bay of Plenty
Northland
Group 3: Wellington
Tues 2nd October
Group 4: Christchurch
Thurs 4th October
Hawkes Bay
Nelson
Marlborough
Whanganui
Waikato
Waitemata
Mid Central
Tairawhiti
Canterbury
Auckland
Lakes
Taranaki
PwC
West Coast
Capital and Coast
Hutt
Counties Manukau
Wairarapa
South Canterbury
Southern
10
Workshop objectives
Module
Know
Think/ Feel
Introduction
The history and purpose
of the New Zealand
Health and Disability
Sector Quality Accounts
Programme
“I understand the Quality
Accounts programme will
be rolled out and I am
clear on what the
programme is”
Understand the benefits,
specific goals and
requirements of the
programme
Making sense
of
information
How to choose and
represent data in a
transparent and effective
format
“I am confident in my
ability to effectively choose
and display my Quality
Account data and
commentary”
Identify key clinical quality
indicators and measures to
document within the DHB
specific Quality Account
Making it
happen
How to lead a successful
Quality Account
development programme
“I know how to develop a
Quality Account and have
clarity on how the
programme will be
successfully led in my
DHB”
Develop the DHB specific
programme plan for the
design, documentation and
publication of a Quality
Account
Where to
from here?
The expectations from the
Commission and support
options available
“I understand what
additional support is
available and how I can
access it if needed”
PwC
Do
Clarity on the next steps
and the identification of
potential future support
requirements
11
Workshop contents & timeline
Intro to
Quality
Accounts
Making sense of information
08.30
11.00
13.00
Registration
& coffee
Morning Tea
Lunch
PwC
Making it happen
15.00
Afternoon
Tea
17.00
Close
12
Learning objectives
The pre-workshop survey indicated that as a sector
your key learning objectives are to establish:
Objective
%
How to develop Quality Accounts
46%
What are Quality Accounts
20%
A consistent approach to Quality
Accounts
10%
Networking opportunities with other
DHBs
8%
How to align with current reporting
4%
How will HQSC use the Accounts?
4%
Possible formats for the Account
2%
How to convince others of the benefits
2%
How to use the Account
2%
How to involve consumers
2%
PwC
What are your top five learning
objectives from this workshop
today and how are you going to
make the space and time to
achieve them?
13
Introduction to Quality Accounts
What is a Quality Account?
2012
PwC
Quality Accounts
Overview
• Quality Accounts are annual reports from health and disability service
providers regarding the quality of the services provided, and how each
provider is progressing in terms of continuous quality improvement, the
consumer experience and health outcomes.
Purpose
• The primary purpose of a Quality Account is to encourage Boards and
leaders of healthcare organisations to assess quality across all of the
healthcare services they offer, and encourage them to engage in the wider
processes of continuous quality improvement.
Benefits
• The publication of a Quality Account provides a mechanism through
which health and disability service providers are able to share their
successes, learnings and future improvements, essentially providing
transparency and accountability for each provider regarding the quality of
their performance.
The introduction of Quality Accounts to all health and disability service providers
within New Zealand marks an important step in putting quality at the heart of all
healthcare activity.
PwC
15
Definition clarity
•
What is your definition of quality?
•
What is your teams / departments /
specialists / divisions and
organisations definition of quality?
•
What is your patients/ consumers /
communities definition of quality?
•
What definition of quality will be
reported on in your quality account?
“O how they cling and wrangle, some who claim
For preacher and monk the honored name!
For, quarreling, each to his view they cling.
Such folk see only one side of a thing”
Udana VI.4Tittha Sutta
PwC
16
The journey so far….
April 2010
Quality
Accounts
became a
reporting
requirement
throughout
the NHS
(UK)
PwC
November
2011
The
Commission
started the New
Zealand Health
and Disability
Sector Quality
Accounts
programme
January 2012
Waikato DHB
published the first
Quality Account
in New Zealand
June 2012
The Commission
published the
New Zealand
Health and
Disability Sector
Quality Accounts
Guidance Manual
August 2012
Waikato DHB
published their
second Quality
Account
National health service programme
Areas of success
• National programme participation
• Consistent focus on the three domains of quality
• Provision of a guidance manual
• A balanced view of positive and negative data
• Regular use of trend data
Opportunities for improvement
• Limited use of statistical tests
• Significant variation in the measures used
• Lack of context and interpretation of the data
• Poor presentation of data
• Limited providers were able to achieve the balance
between rigour and clarity in their data reporting
• Limited use of consumer feedback and participation
PwC
18
Purpose
Quality Accounts allow health and disability
service providers to assess and publicly
report on the quality of healthcare provided
across all of the services they offer.
They:
What is your DHB’s purpose
for designing, documenting
and publishing a quality
account?
Provide a mechanism by which DHBs
are able to transparently share their
successes and future improvements;
Allow boards, clinicians, managers and
staff to demonstrate their commitment
to continuous quality improvement,
and explain their progress to the public;
Provide a means by which the public is
able to hold providers accountable for
their overall performance.
PwC
19
Principles
The principles that should guide the development of each DHB’s Quality Account are:
Accountability and
Transparency
• Quality Accounts are
intended to enhance
responsibility and
accountability within
the system to deliver
high quality health
outcomes.
• Accountability can
only be effective if
matched by
transparency.
Therefore, it is
recommended that
each Quality Account
will be made publicly
available so that the
New Zealand public
can see providers’
progress.
PwC
Meaningful and
Relevant
Focused on Whole of
System Outcomes
Continuous Quality
Improvement
• Each quality measure
within Quality
Accounts must assist
in the understanding
of performance within
the individual provider
and its services.
• It is imperative that
the development of
Quality Accounts does
not become a paper
exercise with the main
driver being “to simply
make the numbers”; it
must be to use the data
to learn and improve.
This means including
meaningful and
relevant quality
measures on quality of
care from a clinical
perspective and also
from the perspective of
consumers.
• All providers of health
and disability services
are encouraged to
produce, or participate
in the production, of
Quality Accounts. This
whole of system
approach will ensure
that patient
accountability extends
across care pathways
and that the reporting
is available across all
sites and services
within individual
organisations.
• The purpose of Quality
Accounts will be to
drive the New Zealand
health system to
continuously improve
and strive for quality
excellence, rather than
simply achieving or
maintaining minimum
standards.
20
The triple aim
Transformation of health care delivery
starts with a transformational aim and it is
widely agreed that within the New Zealand
health sector such a transformational aim
should include a balance or optimisation of
performance on three dimensions of care —
which we call the ‘Triple Aim’.
Improved
quality,
safety and
experience
of care
Triple
Aim
Improved
health and
equity for
all
populations
PwC
Best value
for public
health
system
resources
21
Retrospective & future focused
Retrospective
• An education opportunity,
ensuring a wide audience of
providers can learn from instances
where things went wrong and what
improvement activities work well
PwC
Future focused
• What has been identified as
priorities for improvement over the
coming financial year, and the
plans to achieve and measure these
priorities
22
Suggested content
Opening Statements
Foreword
Statement of
Endorsement
Statement of
Engagement
Statement of Intent
Regarding Feedback
Performance Review
Nationally Consistent Content
Provider Determined Content
Future Focus
Priorities for Improvement
PwC
Capability Development
23
Tube game
Objective
• Lower the tube to the ground
Rules
• The tube must start at shoulder height
• Everyone must have their two index
fingers touching the tube at all times
• Nothing else may touch the tube
• You may not grip the tube, or hook your
fingers round it
• If anyone is spotted breaking any of the
rules, the tube will be put back to chest
height
PwC
24
Review of the tube game
Organisational objectives may be stated easily, yet despite everyone’s willingness and
desire to achieve the objective, it is difficult to do. Why? – because of the difficulty of
coordinating effort against the inertia of the organisation.
Need to understand the problem BEFORE coming up with solutions
Need to fully understand the desired outcome – tube on the ground – before you launch
into implementation
Solutions got lost because people were talking not listening
Challenge constraints – some are real, but many are
self-imposed
You succeeded because you worked together
PwC
25
All of the system working together
The process of producing a Quality Account
mobilises managers, clinicians, front line
staff and support staff to collect, review and
analyse information relating to quality and
to identify their areas of success and
opportunities for improvement. This is
done in such a way that quality excellence
becomes a fundamental part of the health
and disability service provider’s core
business.
Coming together is a beginning.
Keeping together is progress.
Working together is success.
Henry Ford
PwC
26
Making sense of information
Integrated reporting
2012
PwC
www.pwc.com
Quality Accounts:
Capability Development
National Quality and Risk
Managers Meeting
16.08.2012
Calls for change in reporting
Government
Regulators
Communities
Reporting
Employees
PwC
Patients
29
Drivers for change in business reporting
Healthcare information
needs to reflect the
changing drivers of quality
and safety in healthcare
The International
Integrated Reporting
Committee has been
established to create a new
reporting framework
PwC
Growing consensus that
current reporting is not fit
for purpose
Present reports are unduly
focused on past financial
performance
Companies have a licence
to innovate as the concept
of ‘integrated reporting’
develops
Forward-thinking
companies are already
innovating and changing
the nature and scope of the
information they use and
report on
30
Benefits of effective information and reporting
Internal Discipline
Differentiation
External Benefits
Access to capital
Reporting information
aligned with investor and
stakeholder needs
Focus on strategy execution
Future-facing
Enhanced perception of the
‘quality of management’
Joining up the business –
united purpose
Better risk and opportunity
identification
The war for talent
Improving quality and
availability of information
Better informed decision
making
Breaking down ‘silos’
PwC
Clear and concise external
reporting – effective
communication
Lower reputational risks
Building critical
relationships
Lower cost of capital and
better access to capital
31
Reporting maturity
Integrated Reporting
Bringing it all together
Where is your DHB
presently and where do you
wish to be?
Strategic Reporting
Aligning reporting to what matters
Effective Reporting
most
Doing it well and thinking
about users
Compliance
Reporting
Doing what you
have to
PwC
32
How is integrated reporting different?
Current model
Future model
Reporting
scope
Legal ownership and control
Value chain
Dominant
driver
Financial, past
Strategic, holistic, future
Timeframe
Short term
Short, medium and long term
Detail
Long and complex
Concise and material
Rule bound
Responsive to industry &
company
Presentation
Paper based
Electronic
Trust
Narrow disclosure
Greater transparency
Information
construct
Silos
Integrated
Financial capital
All capital–intellectual, human,
social
Compliance
Performance
Source: International Integrated Reporting Council
PwC
33
Making sense of information
Measuring what matters
2012
PwC
Why should we measure?
The old adage “You can only manage what you measure”
Supplies motivation and focus
Is a catalyst for improvement
Allow the ability to evaluate what worked and what didn’t
Imparts a judgement of overall quality
Prompts the important questions
PwC
35
Quality and safety performance indicators
Nationally Consistent Content gives information to the public, which will be
common across all Quality Accounts.
PwC
MoH National
Health Targets
Serious and
Sentinel
Events
Patient Safety
and Experience
Indicators
Regional &
National
Quality, Safety &
Experience
initiatives
Clinical
Indicators
Quality, Safety &
Experience
improvement
programmes
Provider Determined
Content
Nationally Consistent
Content
Provider Determined Content will allow each provider to demonstrate the quality of
care delivered and shows data relevant to specific services and specialities of the
organisation, as well as what consumers and the public say matters most to them
balanced against the Health and Disability Sector’s Triple Aim.
36
Indicator basics
What is a performance indicator?
• A measurement of performance against peers, or against a pre-determined
benchmark or target
• They are not just “statistics” - good metrics typically have a numerator and a
denominator that allow for meaningful trending or comparisons over time
What is a balanced scorecard?
• A collection of individual metrics that collectively provide a “balanced” view
of overall performance
Structure of the scorecard is driven by how it will
be used:
• Measuring results, progress towards an “ultimate objective”
• Motivating the “right” behaviours and actions that will lead to achievement
of the ultimate objective
• Quantifiable evidence for evaluating and/or rewarding performance
PwC
37
Characteristics of good indicators
Improvement starts with knowledge and clarity
Well designed indicators measure the right data, in the right parts of the system, at the
right time
Indicators that help you understand what parts of the system to change and how
In addition to being “fit for purpose”, each indicator should be “SMART”
S
Specific to the area being measured
M
Measurable, on an objective basis
A
Aligned with Health and Safety objectives and/or critical success factors
Realistic
and controllable
by scorecard
the area being
measured
R
Collectively,
the indicators
used in the
should
provide a “balanced” view of
overall performance.
Timely – can be updated on a regular basis
T
PwC
38
Key Questions
How many indicators?
Segmental or group?
Giving the reader multiple performance
measures without explaining which ones
are key to managing their business does not
aid transparency.
You will need to consider how your
indicators are collated and reported
internally – whether they make sense when
aggregated and reported at a group level, or
would be more usefully reported at an
organisational segment level.
The choice of which ones are key is unique
to each company and its strategy; it is
therefore impossible to specify how many
KPIs a company should have.
However, our experience suggests that
between four and ten measures are likely to
be appropriate for most DHBs.
PwC
In some instances, it may be more
appropriate to report separately for each
organisational segment if the process of
aggregation renders the output
meaningless.
Key Questions
How rigid should they be?
Does reliability matter?
You should reflect on whether the
indicators chosen continue to be relevant
over time.
As you are encouraged to move beyond the
more traditional financial indicators in your
public reporting, the issue of data and
indicator reliability will inevitably be raised.
Strategies and objectives develop over time,
making it inappropriate to continue
reporting on the same indicators as in
previous periods. For the purpose of the
first Quality Account, your choice of
indicators is not set in stone for all time;
but the reason for, nature of, changes in
indicators and how they are measured and
reported should be clearly explained.
PwC
In order to address this issue and provide
readers with useful information, we believe
it is more important that the limitations of
the data and any assumptions made in
providing it are clearly explained. Readers
can then judge the reliability for themselves
and make any necessary adjustments in
their own analysis.
Slide 40
Key Questions
Should I disclose my source and
assumptions?
What about changes to my
indicators?
To enable readers to make their own
assessment of the reliability of the
information, it is important to identify the
sources of the data used in calculating
performance indicators and any limitations
on that data.
Comparability over time is a key principle
of good corporate reporting.
Any assumptions made in measuring
performance should be explained so that
readers can reach an informed view of
judgements made by management.
It is recognised that indicators may evolve
over time as strategies change or more
information becomes available.
When such changes are made to the
indicators being monitored, either in terms
of the measures or how they are calculated,
these changes need to be explained.
An indication of the level, if any, of
independent assurance of the data would
also be valuable.
PwC
Slide 41
Quality indicators based on quality data
You have selected your indictors, now the challenge is to ensure that the results are based
on quality data. A quality indicator can only produce useful results if the data that it is based
on is sufficiently relevant, complete and reliable. It is therefore important if you collect any
data locally that you are able both to ensure that it is good data and able to recognise when
it is not.
Completeness: The more complete the data you collect, the more accurately your
indicator will represent the quality of care in your organisation. You should monitor your
systems and look out for missing data. If you find that large amounts of data are missing,
you should revisit your procedures and talk to those collecting the data to identify why.
Relevance: It will not always be possible to collect
data on every relevant incident or procedure. In
such cases you need to decide whether the data that
you have collected correctly represents the whole
picture, or whether there is a systematic difference
between the incidents for which you were able to get
data and those for which you weren’t.
PwC
Reliability: There will always be an element of
human error in collecting data. You should take
steps to make your data more reliable by making
sure that those responsible for data collection fully
understand what they are expected to collect and 42
why.
Selecting the right indicators
Asking questions can help you determine
the right indicators, so think about the
questions that you are trying to answer with
indicators and ensure these questions are
clear.
What questions are you trying to
answer in your organisation around
Health Quality and Safety?
• E.g. You may want to know whether a
particular aspect of the quality of care in
your DHB has improved since last year,
or you may want to know whether your
performance is better than, worse than
or about the same as the national
average.
Think about the questions that your
audience is likely to ask when they read
your Quality Account and try to ensure that
you provide the answers.
PwC
43
Indicator development: step-by-step
Guiding
Principles
Set a robust mechanism for selecting potential indicators- SMART
objectives, combined with the ‘Good Indicator Guide’.
Comms.
Communicate your guiding principles for indicator development with
your stakeholders. Walk them through the process.
Long List
Develop a ‘long-list’ of potential indictors as early as possible & from a
wide variety of sources.
Refine
Refine the long-list in discussions with stakeholders. This may be an
iterative process. Make sure this is documented.
Check
Ensure that indicators are both locally and nationally relevant to your
population and that they ‘stretch’ the organisation.
Feedback
Involve stakeholders and get critical feedback from them. Ensure
feedback is challenging, reflective and absolutely invaluable.
Socialise
Exploit existing structures wherever possible. QAs are the way forward‘orientate’ the organisation around them… ‘this is how we work now’.
PwC
44
Performance indicators
Opening Statements
Foreword
Statement of
Endorsement
Statement of
Engagement
Statement of
Intent Regarding
Feedback
Performance Review
Nationally Consistent Content
Provider Determined Content
Nationally Consistent Content
• Ministry of Health National
Health Targets
• Serious and Sentinel Events
Provider Determined Content
• Quality, Safety and Experience of
Care
• Health and Equity for the
Population
• Value for Public Health System
Resources
Future Focus
Priorities for Improvement
PwC
Capability Development
45
New Zealand health quality measures
In a new report, the Health Quality and
Safety Commission (the Commission)
presents the first set of health quality and
safety indicators.
The report presents the work towards
developing 17 proposed indicators, displays
findings where available, and welcomes
feedback on how the indicator set could be
further strengthened.
In developing these indicators, the
Commission has built upon existing quality Further detail on the definition and calculation
and safety initiatives throughout the sector of each of the indicators is provided in the
definition standards found on the Health
and involved measurement experts and
stakeholders in the process of selection and Quality Measures website: hqmnz.org.nz
definition.
Finalising a set of credible, robust and reliable quality and safety indicators will:
Provide the public and the
health and disability sector
with a clear picture of the
quality and safety of health
and disability services in New
Zealand, including changes
over time
PwC
Inform the quality
improvement activities of
service providers by
providing information to
support learning and peer
review in clinical settings
Identify key quality and
safety issues and prioritise
improvements to the quality
and safety of health and
disability support services
46
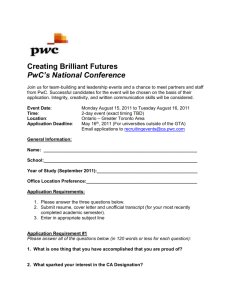
Ten most frequently used measures by the NHS
PwC
92%
• Health care associated infections
90%
• Patient experience
82%
• Waiting times
67%
• Hospital standardised mortality
ratio – overall
54%
• Cancelled operations
49%
• Stroke sentinel clinical audit
46%
• Re-admission rates
44%
• Delayed transfers of care
44%
• Patient safety incidents/never
events/prescribing errors
41%
• Complaints
What indicators could you use
in your DHB?
47
How to define & document an indicator
Once you have selected your indicators it is vital to define and document them. Each
indicator should be defined to the level of detail displayed in the example below, and should
be agreed prior to carrying out data collection, baseline calculation and validation.
Document this in your Quality Account in Section 2.
Indicator ID
IND-001
Indicator Name
Percentage of Hand Hygiene Compliance
Indicator Definition
To be marked as “compliant” , each time a health professional comes in to contact with a patient,
they must carry out hand hygiene steps: Before touching a patient, before a procedure, after a
procedure or Body Fluid Exposure Risk, after touching a patient, after touching a patient's
surroundings
Type
National or Provider
Objective
To increase the number of compliant patient interactions
Rationale
There is a link between infections and hand hygiene, and we want to drive down infections
Owner
Head of Quality Improvement
Measure Calculation
No. of compliant in ward interactions / total number of in ward interactions
Additional
Information
3 wards to be audited with a minimum of 350 interactions audited per ward
3 audits should be performed every year by a qualified auditor
Current Performance
85%
Target
Increase by 5% by December 2012
Review date
Review on the 1st of every month
Data source
This data will be manually collected
PwC
48
Indicator Checklist
Once you have selected your indicators, validate them by using this check list:
the indicators address the important
Do
issues?
Have you captured your local
improvement priorities?
they being captured
Are
/tracked/reported on somewhere else?
Pick a couple of your indicators and
work through a definition and
documentation process for your
Quality Account
Are they aligned to the Triple Aim?
Do know why are you are tracking them?
Do they actually measure what they are
claiming to measure?
Do you know how you will collect the
data?
Do you understand the meaning?
What is the indicator telling you?
What are the implications?
PwC
49
Why indicators fail - pitfalls & how to avoid them
Pitfall
Method of Avoidance
Indicators chosen because they are
immediately measurable or “comfortable”
— even if they are of little value
Start from a solid conceptual framework –
agree first on what needs to be measured,
expressed qualitatively
Indicators drive unintended behaviors
because they do not fully account for the
inherent tradeoffs
Use a balanced scorecard approach with
multiple relevant dimensions, and
objectives within each that address cost,
quality and risk tradeoffs
Indicators are not aligned with “the
ultimate goal” and/or there are too many
indicators and/or the metrics are
“missing” key outcomes or drivers
Use the strategy map framework as the
starting point for developing “top of the
house” metrics, then cascade related
scorecards and metrics to lower level
Lack of buy-in that the indicators are the
“right” ones
Include representation from affected areas
in the development of the indicators
Fear of transparency and accountability
Define and implement an effective change
management programme
PwC
50
Why indicators fail - pitfalls & how to avoid them
(cont)
Pitfall
Method of Avoidance
Don’t have the data required to implement
the “right” indicator
Start with what you have, use proxies
where necessary, and develop a roadmap
for closing the data gap over time
Lack of agreement about what the metrics
mean
Develop clear, easy to understand
definitions and document an “indicator
dictionary”
Indicators are ignored and/or there is
“green light thinking” (a good overall
result that may be hiding significant
underlying pockets of problems)
Define an accountability framework, and a
governance model, enabled by effective
scorecard reporting, including “drilldown”
mechanisms, trend indicators, “stoplights”
etc.
Focus solely on outcome measures
(“lagging indicators”), failure to recognise
emerging issues before it is too late
Overall indicators structure should
contain a good mix of leading indicators as
well, to enable proactive recognition of
emerging issues
PwC
51
Making sense of information
Presenting data
2012
PwC
Presenting Data: Key Principles
Tailor your style and approach to your audience
• Primary audience is the public, but also includes clinicians, DHB staff
commissioners, academics and other experts in healthcare
Focus on the key messages
•
•
•
•
•
These should be of interest to your audience and should matter to them
Do more than just recite the data in words
Explain to the reader what key messages the data contains
Explain what this means about the quality of care provided by your organisation
Explain what this means for them
Use language that your audience will understand
• If you need to use technical language, explain its meaning
• Avoid overly long sentences and try to be as concise as possible
• Stick to simple words and everyday English
PwC
53
Using tables and graphs
Tables and graphs provide a visual representation of your data that can be more effective
than text in getting your message across. They can also break up text and make your
Quality Account much more visually appealing and engaging for the reader.
Smaller tables make it
easier for the reader to
understand the
numbers.
2009-10
2010-11
9.9%
9.5%
Your Region
11.2%
11.0%
All of NZ
10.6%
10.3%
Your Organisation
Table1: Percentage of patients readmitted to hospital within 28 days of discharge
following stroke treatment
Present data in a
logical order to make
it easier to digest
PwC
Right justify numbers
so that their relative
sizes are visually
obvious
Quote numbers only
to accuracy required
to illustrate the key
message
The title should contain all the
information needed to understand
the table. Avoid acronyms and
abbreviations.
54
Tips for using graphs
A good graph can be an extremely effective way of presenting the key results from your data,
but a poor graph can be confusing or misleading. The following tips should help you to create
graphs that are both engaging and revealing to the reader.
Tip 1
Tip 2
Tip 3
One Clear Visual Message: A graph should have one clear visual message.
Resist the temptation to attempt to convey more than one idea in a graph, as this
is likely to confuse the situation.
Clear Headings: Give your graph a clear heading that contains all the
information that the reader needs to understand its content. Avoid acronyms
and abbreviations and use proper grammar.
Avoid Visual Clutter: Avoid unnecessary visual effects, as these can make the
graph much harder to understand. Many common software packages can draw
3-dimensional graphs – steer clear of these as they make it more difficult to see.
Tip 4
Choosing the right type of graph: You should try to choose the most
appropriate type of graph for the data that you want to present.
Tip 5
Axes that don’t start at zero: You should usually start your vertical axis at
zero so that the relative sizes of the values in your graph are visually apparent.
PwC
55
Making sense of information
Using graphs
2012
PwC
Question one
Which graph makes it easier to determine whether the mid-cap US. Stock or the SmallCap U.S Stock are the greater share?
(A)
PwC
(B)
57
Question two
Which of these line graphs is easier to read?
(A)
PwC
(B)
58
Question three
Which of these two tables is easier to read?
(A)
(B)
PwC
59
Question four
Which graph makes it easier to focus on the pattern of change through time, instead of the
individual values?
(A)
(B)
PwC
60
Question five
Only one of these graphs accurately encodes the values. Which graph presents the data
accurately?
(A)
PwC
(B)
61
Question six
Which map makes it easier to find all of the counties with positive growth
rates?
(A)
PwC
(B)
62
Question seven
Which graph makes it easier to determine the R&D’s travel expense?
(A)
(B)
PwC
63
Question eight
In which graph are the labels easier to read?
(A)
PwC
(B)
64
Question nine
Which graph is easier to look at?
(A)
(B)
PwC
65
Question ten
Which table allows you to see the areas of poor performance more quickly?
(A)
(B)
PwC
66
Test answer sheet
Q1. B
Q2. A
Q3. A
Q4. B
Q5. B
Q6. A
Q7. B
Q8. A
Q9. B
Q10. A
PwC
67
Making sense of information
Dashboard design
2012
PwC
Quality account dashboard overview
One way of recording, monitoring and presenting the results of your indicators is through a
dashboard.
• Dashboards are visual displays
• Dashboards display the information needed to
achieve specific objectives
• A dashboard fits on a single computer screen
• Dashboards are used to monitor information at a
glance
• Dashboards have small concise, clear and
intuitive display mechanisms
• Dashboards are customised
• Dashboards provide immediate insight into
what’s going on
• Dashboards enable quick recognition of what
needs attention
“A dashboard is a visual display of the most
important information needed to achieve
one or more objectives; consolidated and
arranged on a single screen so the
information can be monitored at a glance.”
Stephen Few
PwC
69
Dashboard workshop & challenge
Discussion Workshop
Dashboard Design Challenge
This group should discuss their
understanding of a quality and safety
indicator dashboard.
The group should design a Quality and
Safety Indicator dashboard.
The group should come up with:
1. A high level definition
2. Key components
3. Design characteristics
4. What not to include on a
dashboard
PwC
Each component on the dashboard
should be labelled with an explanation
of what it is and why it is required
70 70
Guiding principles of dashboard design
Keep It Super Simple
(KISS)
Selecting the right data
Organise it logically
Single screen –
keeping all data within
eye span
Don’t waste an inch of
space & don’t sacrifice
meaning
Avoid unnecessary and
distracting decoration
Include only the
information that you
really need
Condense information
in ways that don’t
decrease its meaning
Visual display
mechanisms that even
when quite small, can
be easily read and
understood
“Eloquence in communication is often achieved through simplification. Too often we smear a
thick layer off gaudy makeup over data in an effort to impress or entertain, rather than focusing
on communicating the truth of the matter in the clearest possible way.”
Stephen Few
PwC
71
71
Understand your real estate
Different degrees of visual emphasis are associated with different regions of a dashboard.
Emphasised
Neither – Emphasised
Nor de-emphasised
Emphasised
Neither – Emphasised
Nor de-emphasised
PwC
De-emphasised
72
Essentials of dashboard design
Design your
dashboard to fit in
one screen
Supply adequate
context in support
of the data
Display data
through
summaries and
exceptions
Choose your
indicators and
measures carefully
Select simple,
efficient charts and
graphs
Be consistent in
your use of colour,
fonts and display
media
Make sure the data
is accurate
Arrange the data
logically so it
information flows
Highlight
important data
effectively
Keep the display
clean and clear
Use colour
sparingly and with
meaning
Create a pleasant,
easy to view
display
PwC
73
Dashboard design checklist
What level of summarisation should I express the measure?
What means of display would best express this measure?
At what point in the sequence of viewing the items on the dashboard might a Quality
Board what to see this measure?
What unit of measure should I use to express this measure?
What complementary information should I include as context to enhance this
measure’s meaning?
How important is this measure to the Quality Account compared to the other
measures?
What other measures might you want to compare to this one?
Get your audience involved in the design process and
involve them in answering these questions
PwC
74
Dashboard design step by step
Determine the
objectives of your
dashboard
Determine what
decisions /
actions will be
made
Determine how
the information
will be delivered
(media)
Determine who is
the audience of
your dashboard
Confirm
definition of
metric
Confirm how the
metrics are being
calculated
Determine where
these metrics will
come
Determine which
metrics will be
used
Create a
‘wireframe’ using
dashboard design
principles
Seek feedback on
the ‘wireframe’
with a sample
audience
Review and
revise design in
light of feedback
Implement your
dashboard and
test again
PwC
75
Example dashboards
PwC
76
Making sense of information
Statistical process control
2012
PwC
There are four key applications of SPC for the
health sector
Examine a process for stability
over time before starting a
quality improvement
intervention
Find any special causes of
variation & explain it or
contain & mitigate it
Why use
SPC?
Communicate process
performance over a period of
time
PwC
Monitor the progress of a
process during and after
intervention
78
A basic understanding of statistics
• The mean (µ) is the arithmetic average of a set of data – calculated by adding together
all data values and dividing by the number of values.
• The standard deviation (σ) of a group of numbers can be thought of as the average
distance from each data point to the mean, and is easily calculated using an Excel
spreadsheet.
• For a normal distribution, 99.73% of points will fall within three standard deviations
from the mean in either direction.
68.26%
95.46%
99.73%
µ-3σ
PwC
µ-2σ
µ-1σ
µ
µ+1σ µ+2σ
µ+3σ
Slide 79
Variation exists in all processes – there are two
main causes for this
Common cause
• Predicted or expected variation
• Inherent in the process
• E.g. age, gender, condition
Special cause
• Unusual or unexpected variation
• Can be traced back to a special event or specific
action
• E.g. someone coded in the wrong number
PwC
Slide 80
These causes require different actions to be taken
Type of variation
What it means
Appropriate action to take
Common cause
• Process is in
control
• Variation is
inherent in the
process
• Change the process
• Do not react to individual differences or
try to explain differences between high
and low numbers
Special cause
PwC
• Process is
unstable and
unpredictable
•
•
•
•
Identify and resolve special cause
If negative, minimise or prevent
If positive, build into process
Do not react by changing the process, as
it may not be the system at fault
Slide 81
SPC uses Control Charts with three basic
components to distinguish between the causes of
variation
1. A centreline (CL), usually
the mathematical average of
the sample points plotted.
2. Upper and lower
statistical control limits
(UCL, LCL) that define the
constraints of common
cause variations.
3. Performance data plotted
over time.
PwC
Slide 82
Creating and interpreting a control chart
Determine quality measure you want to
monitor and retrieve historical data (at
least 30 data points)
Collect the sample data (at least 15-20
data points)
Construct the chart in Excel and
annotate the chart
Investigate any areas of variation & take
appropriate action
Recalculate control limits when a
permanent change has occurred in the
process
PwC
Slide 83
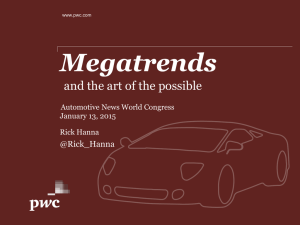
Control Charts can be divided into six zones to aid
interpretation and identify special cause variation
UCL = µ + 3σ
µ + 2σ
µ+σ
CL = µ
µ-σ
µ - 2σ
LCL = µ - 3σ
• The zone between
the control limits
represents
common cause
variation
• The zone outside
the limits is the
area of special
cause variation
Identifying special cause variation:
a. One data point falling outside the 3σ control limits =
OUTLIER
b. 2 out of 3 consecutive points outside the 2σ limit = TREND
c. 4 out of 5 consecutive points outside the 1σ limit = TREND
d. 6 points in a row steadily increasing or decreasing =
TREND
e. 7 points in a row on same side of the centreline = SHIFT
f. 14 or more points alternating up and down = CYCLE
PwC
Slide 84
Control Charts can be divided into six zones to aid
interpretation and identify special cause variation
Daily Potassium TAT
Common cause
120
variation
only
Net Operating Margin for Hospital B
12
UCL = 114.6
UCL
= µ + 3σ
110
8
90
Percent
CLX == 83.3
µ
80
70
60
LCL = µ - 3σ
6
CL
=µ
X = 4.60
4
2
0
LCL = -.04
LCL
= µ - 3σ
LCL = 51.9
50
40
-2
-4
1
3
5
7
9
11
13
15
17
19
21
23
25
1
2
3
4
5
6
7
8
9
Month
12
10
Patient Time at Clinic (arrival to departure)
UCL
UCL== µ
9.5+ 3σ
8
6
4
CL = µ
X = 3.2
2
LCL== µ
None
LCL
- 3σ
10-Apr
08-Apr
04-Apr
02-Apr
31-Mar
29-Mar
27-Mar
25-Mar
23-Mar
21-Mar
19-Mar
17-Mar
15-Mar
13-Mar
11-Mar
09-Mar
0
07-Mar
Wait time (hours)
Day (Not Counting Weekends)
Variation can be
explained by an
event
Special variation
– needs to be
investigated
10 11 12 13 14 15 16 17 18 19 20 21 22 23
06-Apr
Minutes
UCL
= µ + 3σ
UCL = 9.25
10
100
Day
PwC
Slide 85
Control chart interpretation
Using the previously
explained rules, how
would you interpret
UCL = µ + 3σ this control chart?
µ + 2σ
µ+σ
CL = µ
µ-σ
µ - 2σ
LCL = µ - 3σ
PwC
Slide 86
Interpretation example
Annotation
should explain
any special
variation
There are two months where the fall rate was unusually high. Investigation should
begin to explore the special causes behind those identified months with high fall rates
to help prevent this from occurring in the future. For example, one of the months
may have been unusually high because a new, inexperienced nurse was added to the
floor who had not yet been fully trained in fall prevention strategies.
PwC
Slide 87
Summary
SPC is a useful tool for monitoring,
controlling and improving a process over
time through statistical analysis
When and where will you use SPC
in your Quality Account?
It is most effective when used as an ongoing
monitoring tool with clearly defined actions
and responsibilities – not as a reaction to
problems.
Need to understand the type of variation
that is occurring as this will determine how
to address the issue.
Recalculate control limits only when a
permanent, desired change has occurred in
the process and using only data after the
change occurred.
SPC Template
PwC
Slide 88
Making sense of information
Improvement identification
2012
PwC
Prioritisation matrix
Many organisations struggle to balance a
growing list of new and pending projects
while the need for core services continues,
often with less funding.
A prioritisation matrix supports structured
decision-making in the following ways:
Multiple criteria
• Helps prioritise complex or unclear issues when
there are multiple criteria for determining
importance
A prioritisation matrix is a simple tool that
provides a way to sort a diverse set of items
into an order of importance. It also
Consistency
identifies their relative importance by
• Provides a quick and easy, yet consistent, method
deriving a numerical value for the priority
for evaluating options
of each item.
Objective
The matrix provides a means for ranking
• Takes some of the emotion out of the process
projects (or project requests) based on
Quantifiable
criteria that are determined to be
• Quantifies the decision with numeric rankings
important. This enables a department to
see clearly which projects are the most
Adaptable
important to focus on first, and which, if
• Is adaptable for many priority-setting needs
any, could be put on hold or discontinued.
Provides focus
• Establishes a platform for conversations about
what is important
PwC
Slide 90
Healthcare example
Example Prioritisation Tool - Courtesy of
Waitemata DHB
Remember that the prioritisation matrix
itself is just a tool, and the people scoring
projects are using their best judgment.
What is the criteria that you
will use in your DHB to
determine your improvement
priorities?
Upon review, your Quality Accounts
programme team may decide that a project
needs to move up or down in priority,
despite the score it received. These types of
adjustments are expected and help finetune the priority list.
Be sure to vet the results with others in the
organisation, as well as customers and
stakeholders.
PwC
July 2011
Slide 91
Ball game
Objective
• Complete the ball circuit
Rules
• Everyone must touch the ball
• You may only touch the ball once
• The ball may not bounce, or touch
anything other than your hands
• If anyone is spotted breaking any of the
rules, the circuit will be started again
PwC
92
Review of the ball game
Thinking differently was the only real, sustainable bridge to get you from where you were
to where we would like to be.
To succeed in this game you were able to progress your team through the following
journey:
Perceived
issue
Look at it
differently
Reframe the
issue
Creative
refinement
Apply
criteria to
select ideas
Generate
ideas and
approaches
Test revised
process
Tweak if
necessary
Success!!
PwC
93
Looking at things differently
"Here is Edward Bear, coming downstairs
now, bump, bump bump, on the back of
his head, behind Christopher Robin. It is,
as far as he knows, the only way of
coming downstairs, but sometimes he
feels that there really is another way, if
only he could stop that bumping for a
moment and think of it.”
AA Milne
PwC
94
PDSA methodology & quality accounts
PDSA is a great methodology to implement improvements using indicators. The Quality
Account is where you document your plans, your results and what you plan to do next.
There are four stages of the PDSA
cycle:
Plan
the change to be tested or
implemented
Do
carry out the test or change
Study
data before and after the
change and reflect on what was
learned
Act
plan the next change cycle or
full implementation
Note: You can use plan, do, study, act (PDSA) cycles to test
an idea by temporarily trialling a change and assessing its
impact
PwC
95
PDSA methodology basics
PDSA cycles form part of the quality improvement framework,
which provides a model developing, testing and implementing
changes leading to quality improvement. The framework
includes three key questions and a process for testing change
ideas.
The answers to these questions should be documented in
Section 1 of the Quality Account.
Model For
Improvement
What are we trying to
accomplish?
How will we know if a
change is an
improvement?
What changes can we
make that will result
in improvement?
• What are we trying to accomplish?(The aims
statement )
• How will we know if the change is an
improvement?
• What changes can we make that will result in
improvement?
PwC
96
PDSA basics: goal focused
Set clear and focused goals relating to your quality
improvement efforts. It is vital that you select relevant goals
supported by the right mix of indicators.
Goals should focus on quality and safety problems that cause
concern to you, as well as to patients and staff.
These quality improvement goals for your DHB are expressed
in the “aims statement” and should be documented in section
1 of the Quality Account.
Model For
Improvement
What are we trying to
accomplish?
How will we know if a
change is an
improvement?
What changes can we
make that will result
in improvement?
Top Tips for Aims Statements:
• Be consistent with any national goals and
relevant to the length of the project
• Be bold in its aspirations
• Have clear, measurable targets
Note: We discuss indicator selection later on in the section
PwC
97
PDSA Basics: recognising an improvement
Recognising a change as improvement is a vital part of the PDSA
methodology. You want to know whether your change has worked
and the effort paid off.
You will need to measure outcomes, such as reduction in the time
a patient has to wait in order to answer this question.
If you make a change, this should affect the measures and
demonstrate over time whether the change has led to sustainable
improvement. The measures in the model are tools for learning
and demonstrating improvement, not for judgment.
Model For
Improvement
What are we trying to
accomplish?
How will we know if a
change is an
improvement?
What changes can we
make that will result
in improvement?
You should collect data to demonstrate whether changes result in
improvement.
You should report improvement progress monthly on time series
graphs known as ‘run charts' or statistical process control charts
(SPC) and then document in the annual Quality Account in
section 2, the Performance Review.
PwC
Slide 98
98
PDSA basics: selecting the change
There are many potential changes your team could make. However,
evidence from scientific literature and previous improvement
programmes suggests that there are a small number of changes
that are most likely to result in improvement.
These changes you have made and the reasons why should be
documented in your Quality Account in section 2.
Top Tips from the UK
The Cancer Service Collaborative identified twenty eight
change principles which they grouped into four areas that
you may find helpful. These were their areas for changes.
Each area had a series of change iterations associated with
them in order to achieve their goal.
• Connect up the patient journey
• Develop the team around the patient journey
• Make the patient and care experience central to every
stage of the journey
• Make sure there is capacity to meet patients' needs at
every stage of the journey
PwC
Model For
Improvement
What are we trying to
accomplish?
How will we know if a
change is an
improvement?
What changes can we
make that will result
in improvement?
99
Improvement priorities: consumer feedback
Consumer feedback is a great input into the
selection of improvement opportunities and also
the future focus of the DHB. Consumer feedback
can also help:
• To improve communication and shared
decision-making between consumers and staff
How could you engage with
your consumers and get their
feedback? What feedback
would ask them for?
• To build trust and confidence in the DHB locally
and nationally
• To inform planning and service improvement
• To provide accessible and responsive services,
based on people’s identified needs and wants
• Consumers to shape the services that they use
If you engage with consumers to drive out future
priorities for improvement, then document this in
your Quality Account in section 3, Future Focus
PwC
100
Making it happen
Programme management
2012
PwC
Protected Quality Assurance Activity1 (PQAA)
• The coverage of the PQAA law will vary by DHB
• It is recommended that you speak to your in-house legal council to
determine ramifications for publishing Quality Accounts
1Section
PwC
54 – Health Practitioners Competence Assurance Act 2003
102
Making it happen
Feasibility
2012
PwC
Feasibility stage
The feasibility stage recommends activities to make sure that each provider is ready to
develop and implement their Quality Account.
Main Activities
Prepare a business case; develop estimates for the
costs and timescales
Expected Outcomes
Completed business case including risk register
Confirmation that the resources (people, budget
Identify non clinical resources required to develop
and time) required to generate and deliver the
and implement the Quality Account
Quality Account are available
Engage with clinical and executive leads to
Approval gained from the board and executive
establish and confirm senior level support
team
Consult individual clinical teams and provide a
clear understanding of the practical benefits of the
Strong clinical engagement and support
Quality Account in improving health outcomes
and local clinical care
Identification of how the Quality Account will
Consider how the Quality Account can address
help to improve the quality of care and the
local concerns and difficulties
service provided to patients
Gain an overview of existing systems and
An understanding of the provider’s capability to
reporting
implement and accurately measure performance
Identify target stakeholder groups for the Quality
Completed stakeholder management and
Account, including assessing their needs and
communications plan
expectations
Page 104
PwC
Create a programme aim
The aim statement enables the organisation to have a
Using the purpose you defined
good understanding of why Quality Accounts are
earlier today, develop an aim
important and to engage key clinical staff and the
statement for your DHB’s Quality
wider workforce regarding both the benefits of
Account
Quality Accounts and the process for implementing
them.
Creating a clearly defined vision of the future that
inspires and motivates the workforce is an important
first step on the path of success for this programme.
An effective aim statement should be concise,
motivating, and memorable and should be easily
understood by a wide variety of stakeholders and is
written with the broadest grouping of stakeholders as
the target audience.
PwC
105
Obtain board sponsorship and buy in
Addressing these demands needs to be
treated as a project in its own right, with
sponsorship from a member of the Board
and ownership clearly taken by the Board
or a Board sub-committee. Whoever takes
responsibility will need to oversee a
planned and transparent process.
How will you obtain board
sponsorship for this programme?
A first step should be to nominate an
individual with responsibility for
understanding the implications of these
demands for the accounts development.
This individual should then brief the Board
on what the implications are for their DHB.
PwC
106
Business case
A business case captures the reasoning for
initiating a project or task. It is often presented
in a well-structured written document, but may
also sometimes come in the form of a short
verbal argument or presentation.
What activities will your
programme team need to do to
develop and have your DHB
approve a business case for your
Quality Accounts programme?
The business case answers the question: ‘Is the
investment in this programme worth it?’
And is an aggregation of specific information
about the programme:
Value of the benefits
Risks to achieving them
Costs of delivering
Timescales for achievement
PwC
107
Programme risk
As part of your business case, it is recommended
that you identify any potential risks and issues to
your programmes success and establish appropriate
mitigation actions.
Risks
Aspect
Affected
(e.g. getting
stakeholder buyin)
(e.g.
completion,
execution)
PwC
What risks can you foresee
and what actions would
you need to put in place to
mitigate these?
Mitigations
(e.g. action, accept)
Stakeholder management & communications
Engaging stakeholders is more than relying on
planned communications that are little more than a
task list with a bias toward outbound information.
Successful communications are based on four core
elements:
• Message clarity and consistency: ensure relevance
and recognition, and engender trust
• Stakeholder identification and analysis: send the
right message to the right audience
• A system of collection: obtain feedback and assess
the effectiveness of the communications process
• A system of message delivery: get the right
messages to the right stakeholders in a timely and
effective way
It will also be important at this stage to identify the
relevant “information owners” who may be required
to contribute to the annual report.
PwC
Identify who your key
stakeholders for this
programme are and how you
will communicate with them
Making it happen
Initiation
2012
PwC
Initiation stage
The initiation stage involves defining the requirements for each set of Quality Accounts,
and understanding what will be delivered, who will deliver it, and at what cost.
Main Activities
Establish governance structures and
processes for the Quality Account project
Produce a structured, detailed and
resourced Project Plan for putting the
Quality Account in place
Share any existing metric information
from previous prototypes, pilots or other
processes that may be relevant
Set up wider clinical teams and give them
the appropriate background information.
These teams should include
multidisciplinary team members
June 2012
PwC
Expected Outcomes
Documented and agreed governance and
processes for the Quality Account project
including sign-off requirements and
change management processes
Confirmed approach to generating the
Account
Project team and their availability
confirmed
Utilisation of existing reports and metrics,
avoiding the ‘re-invention the wheel’ where
possible
To have consulted clinicians and to have
attracted as much interest in the project as
possible
Page 111
Planning your programme
Developing a robust programme plan is
essential to ensure that all time, cost and
quality requirements are delivered to.
*
Benefits
It manages the transition of the solution
developed into business operations.
It provides a framework that integrates and
reconciles competing demands for
resources.
It recognises the people aspects of change
that must be accommodated if the
programme is to succeed.
“He who fails to plan is planning to fail”
Winston Churchill
PwC
112
Planning and Control Checklist
Budget – are we within our spending limits?
Schedule – are tasks happening on time?
Risk and Issue Management – are we
mitigating risks and addressing issues?
Develop a high level plan for
the design, documentation
and publication of your
Quality Account
Progress Monitoring and Reporting – are we
communicating our progress?
Change Control – are we tracking changes?
Quality Management – are we following a
quality-driven approach?
PwC
113
Making it happen
Scoping
2012
PwC
Scoping stage
The scoping stage will ensure that requirements for the Quality Account are able to be
agreed with the clinical teams. Identifying realistic and achievable areas to focus on will
enable the planned benefits to be realised within the timescales set. This can be done
through a number of workshops.
Main Activities
Engaging a broad range of clinicians from each
speciality to attend requirements-gathering
workshop(s)
Carrying out research into the availability of data
(inside and outside the organisation)
Carrying out and supporting requirements sign-off
workshop
Conduct project scoping and create development
plan
Consulting clinical teams on any identified
difficulties or changes to metrics and ensuring the
clinical relevance and purpose of the metrics is
maintained
PwC
Expected Outcomes
Agreement on a balanced selection of indicators
covering:
• Quality, Safety and Experience of Care
• Health and Equity for the Population
• Value for Public Health System Resources
An agreed estimate of resource and cost
requirements for the generation and on-going
management of the data measurement system
Requirements signed off by the clinical leads for
each specialty and the Board
A detailed project plan to put the Quality
Accounts in place and a key milestone
development plan for each of the Accounts
modules
Ongoing engagement with the clinical leads
Performance indicators
As discussed previously, there are two
elements to the performance measures that
are to be represented in your Quality
Account:
How will you engage across
your organisation and
community to identify the
indicators in your account?
Nationally Consistent Content
Ministry of Health National Health Targets
Serious and Sentinel Events
Provider Determined Content
Quality, Safety and Experience of Care
Health and Equity for the Population
Value for Public Health System Resources
PwC
116
Making it happen
Development
2012
PwC
Development stage
The development stage will typically start once the scoping stage is complete and the
requirements for the Quality Account have been agreed with the clinical team.
Main Activities
Setting regular development checkpoints to
help achieve the main aims
Developing a training and user acceptance
testing plan
Developing and agreeing a communications
plan
Expected Outcomes
Quality of the Account is assured, through a
structured system test plan
A defect identification and resolution plan
developed
Communications, testing and training plans
agreed
An understanding of the information
management and information technology
Produce a detailed data plan – outlining the
resource implications for delivering the
metrics that are needed and the systems
Quality Account (e.g. if systems need to be
that the data will be taken from
changed to capture data required for the
Account)
Consulting clinical teams on any identified To continue developing useful metrics,
difficulties or changes to metrics because of agreed by the clinical lead to be an
data configuration and so on, and making
appropriate balance between the metrics
sure the clinical relevance and purpose of
identified initially and any identified
the metrics is maintained
difficulties with local data flows
118
PwC
Data plan
Outline the metrics that are needed, the systems that What is your plan / approach
to collecting data?
the data will be taken from, and any resource
implications for delivering the Quality Account (e.g. if
systems need to be changed to capture data required
for the Account).
Metric
PwC
Data
System or
Manual?
System
Name
Resource
Implications
119
Publishing
Below is a recommended approach to publishing a
Quality Account:
Where will you be publishing
your Account?
PwC
Publish
Communicate
Final Edit
Ensure that
all employees
Upload the
within the
Review with
Quality
organisation,
Consumers,
the
Account to the
Health
organisation’s
community
Literacy
website and
and the wider
Specialists
sector
share the link
and Content
with The
understand
Editors
Commission
where and
how to access
the Account
Consider the needs of the community and adopt
relevant distribution methods as necessary.
120
Making it happen
Writing for the reader
2012
PwC
Structured Thinking Tools
“If you do not know where you are
going, then any road will do”
The Cheshire Cat to Alice,
from Lewis Carroll’s Alice in
Wonderland
PwC
Page 122
Good structures begin with thinking about what
you need to write
Your structure will help you:
• prioritise and organise your ideas
• check that your message has a logical flow
• ensure completeness.
These are some useful techniques for structuring your thoughts:
• Minto
• Mind-mapping
• Storyboarding
Generating, prioritising and
organising ideas
• Captive Moments
• “The Ministerial Three”
Writing with impact
PwC
Page 123
Minto’s structured thinking is a method of critical
thinking designed to present ideas in a logical way
SUMMARY
IDEA
We all seek structure, whether we
realise it or not.
The mind automatically sorts
information into groups to understand
it.
These groups are pyramids:
• A summary idea
• Lesser ideas grouped logically
below (e.g. in order
of importance).
IDEA
1
A
B
C
IDEA
2
D
E
=Main idea/
Conclusion
IDEA
3
F
G
H
@
@
@
# # #
= Supporting
arguments
I = Supporting
arguments
= Facts
The Pyramid Principle: Logic in Writing and Thinking, Barbara Minto (2002)
PwC
Page 124
Structured Thinking Tools – Minto
Imagine you receive this letter from Lucy.
What does she want to tell you?
Dear Shirley
Remember last Saturday afternoon when I was playing in the
park with my boyfriend and you came over, and he told me
that when my back was turned, you kissed him?
And also, on Sunday when you came to my house and my
Mum made you a tuna fish salad for lunch and you said:
“Yech! That’s the worst salad I ever ate!”?
And yesterday, when my cat brushed against your leg, you
kicked her and threatened to set your dog “Monster” on her?
Well, for all of these reasons, I hate you, and I no longer want
to be your friend.
Lucy
PwC
Page 125
Structured Thinking Tools – Minto
Wouldn‘t the message be far clearer if the letter
were written according to Minto’s pyramid
principle?
Main idea / conclusion
Dear Shirley
I hate you. Here are my reasons:
1. You stole my boyfriend.
2. You insulted my mother.
Reasons
supporting
the main idea/
conclusion
3. You scared my cat.
PwC
Page 126
Structured Thinking Tools – Minto
In letter 2, Lucy’s thought hierarchy becomes
explicit and can be considered as a fictitious
question-answer dialogue
Q: Why did Lucy write this letter to me?
Lucy hates me
A: Because…
Q: Why?
A: Because…
PwC
I stole her boyfriend
I insulted her mother
I scared her cat
Page 127
Structured Thinking Tools - Minto
To communicate effectively with your audience,
you need to summarise your ideas into a pyramid
that they can understand.
The pyramid can guide the structure of your final document.
IMPROVE
BOTTOM LINE
Improve
Marketing
Reduce
Costs
= Title
Increase
Output
Increase
Print Media
Improve
Website
Increase
Targeted Direct
Mail
Improve
Look
Improve
Speed
Increase
Functions
PwC
#
#
= Sections /
chapters
= Sub-sections/
paragraphs
= Sub-paragraphs
# = Bullet points/text
Page 128
Structured Thinking Tools - Minto
Using inductive and deductive arguments in
writing
You Must
Change
You Must
Change
Why?
Here’s what is
going wrong
Here’s what is
causing it
How?
Therefore,
here’s what
you should do
about it
How?
A1
PwC
B1
C1
A2 B2 C2
A3 B3 C3
B2
Why?
A2 - Cause
of problem
C3
B3
A3 - What you
should do
B1
C2
C1
A1 - What’s
going wrong
Page 129
Structured Thinking Tools - Minto
Minto advocates avoiding deductive arguments in
writing
An example of inductive thinking/reasoning:
You Must
Change
•
•
•
•
How?
B3
A3 - What you
should do
Why?
A2 - Cause
of problem
PwC
Situation
Complication
Question
Answer
C3
How?
B2
B1
C2
C1
A1 - What’s
going wrong
Page 130
Structured Thinking Tools - Minto
Supporting technique
S–C–Q–A
Situation:
“For a long time we have been …..”
- Something you already know
- Sets up complication
Complication:
“Recently the situation has changed…..”
- Triggers the question to be asked
Question:
“So what should we do?”
- Leads to the answer
Answer:
“We need to ….”
- Your main point
- Summary thought for your introduction
PwC
Page 131
Structured Thinking Tools – Mind Mapping
Mind mapping: a mind (or concept) map consists
of a central word with related ideas radiating out
from it
PwC
Page 132
Structured Thinking Tools – Mind Mapping
Use a mind map to generate, prioritise and order
logically the issues that you want to present in your
document
= main points to include in document
PwC
Page 133
Structured Thinking Tools – Mind Mapping
5 Steps to Making a Mind Map
PwC
Page 134
Structured Thinking Tools – Mind Mapping
Seven tips for making a mind map
Tip
Rationale
1.
Start in the centre of a blank page
turned sideways.
2.
Use an image or picture for your
central idea.
3.
Use colours throughout.
Because starting in the centre gives your brain freedom
to spread out in all directions and to express itself more
freely and naturally.
Because an image is worth a thousand words and helps
you use your Imagination. A central image is more
interesting, keeps you focussed, helps you concentrate,
and gives your brain more of a buzz!
Because colours are as exciting to your brain as are
images. Colour adds extra vibrancy and life to your mind
map, adds tremendous energy to your creative thinking,
and is fun!
Because your brain works by association. It likes to link
two (or three, or four) things together. If you connect the
branches, you will understand and remember a lot more
easily.
Because having nothing but straight lines is boring to
your brain.
Because single key words give your mind map more
power and flexibility.
Because each image, like the central image, is also worth
a thousand words. So if you have only 10 images in your
mind map, it's already the equal of 10,000 words of
Page 135
notes!
4. Connect your main branches to
the central image and connect your
second- and third-level branches to
the first and second levels, etc.
5. Make your branches curved rather
than straight-lined.
6. Use one key word per line.
7.
PwC
Use images throughout.
Storyboarding: A good story has simple, logical
elements
Element
Purpose
Roadmap
“Tell them what you’re going to tell them”
What the problem is
Set the stage
What we did
Outline approach or methodology; build credibility
What we found
Present findings
What that means
Interpret findings and make conclusions
What we need to do
Make recommendations
What happens next
Outline next steps
PwC
Page 136
Making it happen
Structured writing tools
2012
PwC
Structured thinking tools
•
Minto’s Pyramid Principle
•
Captive Moments
•
“The Ministerial Three”
PwC
Page 138
Structured Writing Tools – Minto
How to build your document according to the
pyramid principle
Step 1: Start with the pyramid
foundations:
Step 2: Create the pyramid outline:
•
Situation, problem and main idea must
fit together
•
Ensure your pyramid forms a questionand-answer dialogue
•
Ensure all parts of the pyramid are
formulated as proper sentences
•
Ensure your message is summarised in a
one-sentence main idea/conclusion
• Define your audience
• Define your goals
• Define the situation
• Define the complication
• Define the question (problem)
PwC
Page 139
Structured Writing Tools – Minto
How to build your document according to the
pyramid principle (continued)
Step 3: Check the solidity of your
pyramid construction:
Step 4: Check proper relationships:
•
Ensure supporting elements are mutually
exclusive and collectively exhaustive
•
• Ensure each statement has at least 2,
but no more than 5 supporting
statements
Ensure supporting elements are of the
same level of abstraction
•
Ensure supporting elements answer the
same question
• Ensure the supporting information is
a group or valid chain
•
Ensure supporting elements are
presented in a logical sequence
• Ensure your question-and-answer
dialogue is complete
PwC
Page 140
Structured Writing Tools – Minto
How to build your document according to the
pyramid principle (continued)
Step 5: Writing your document:
• Consider the pyramid’s foundations
(step 1)
•
Ensure chapters have introductory
paragraphs
• Think about contents of text
•
Ensure the logical relationship between
paragraphs is indicated
•
Ensure your text fits your goal and
audience
• What structure best suits your message?
• Begin writing first draft
• Ensure your text has a clear introduction •
PwC
Revise draft as needed
Page 141
Structured Writing Tools – Minto
Structure your document according to the
pyramid principle
The pyramid will guide the structure of your document.
Major Thought/
Conclusion
H1
H2
Paragraph
H1
H1
Section Headings /
Chapter
1.
H2
H2
Sub-section Headings /
Paragraphs
1.1
Paragraph
Paragraph
Numbered Sub-Paragraphs
#
PwC
Title
#
#
1.1.1
Bullet points/text
Page 142
Structured Writing Tools – Minto
Tips and tricks on building your pyramid
• You can build the pyramid two ways:
- Bottom up
- Top down
• Start bottom up if you have a lot of
information, but don’t know the main
idea
• If you know your main idea, but
haven’t got lots of facts and figures,
start at the top and work down
PwC
Introductions tell stories around:
1.
The situation - quick, factual sketch
of current situation
2.
The complication - a problem that
unsettles the situation in the story
3.
The question - can be ‘what should
we do?’ or ‘how can we do it?’
4.
The answer - your response to the
question and your solution to the
complication
Page 143
Structured Writing Tools – Captive Moments
Take advantage of your audience’s two moments of
greatest interest to communicate main messages
Level of Interest
START
Start of document:
set expectations and
create interest
END
End of document:
summarise key
points and actions
Stage of Document
Also known as: “Always put your best strawberries at the top
of the basket.”
PwC
Page 144
Structured Writing Tools – The Ministerial Three
Ideas for structuring your content - using the “Tell
Them” approach
This well-known rule of thumb offers a useful starting point and reminds us that
audiences need strong orientation and clear reminders of what has been covered:
• Tell them what you're going to tell them (Introduction)
• Tell them (Body)
• Tell them what you told them (Conclusion)
PwC
Page 145
Structured Writing Tools – The Ministerial Three
“The Ministerial Three”:
use repetition to guide your audience through your
document and emphasise important messages
Step One
Tell your audience what you’re
going to cover (A, B, C…)
Step Two
Cover the information (A, B, C …)
Step Three
Summarise what you’ve covered
(A, B, C …)
No mystery tours!
PwC
Page 146
Structured Thinking Tools - Minto
Some style tips
Your audience, message and purpose of communication should determine the specific
language you use. But all audiences will benefit if you follow these rules.
• Use active verbs in place of passive
• Avoid strings of nouns
• “Own” your writing - e.g.. the personalised
CV
Create a sense of action
and ownership
• Use simple words and phrases
• Limit jargon
Keep it simple
• Keep your sentences short
• Grammar accuracy
• Tables/diagrams to illustrate key points
• Choose the right tone
PwC
Suit your tone to your audience
Page 147
Structured Writing Tools – Summary
Sample style checklist
source: Plain English NZ
Check the whole document
It's simple, clear and concise
The topic is obvious
The main message is obvious
It's obvious what action the reader needs to take
Check the document structure
Detailed, explanatory document title or page headline
Summary or key message follows title or headline
Content organised in a logical sequence for the reader
Each paragraph starts with its topic
Short paragraphs
Sub-headlines and short lists break up solid text
Check your sentences
Mainly short sentences
Mainly active verbs (I appointed you not You were appointed by me)
Logically structured sentences (subject-verb-object)
Only one main idea in each sentence
Correct grammar, spelling and punctuation
PwC
Page 148
Structured Writing Tools – Summary
Sample style checklist
source: Plain English NZ
Check your words
Words that are common, simple, and familiar to your target audience
Write you, I and we: speak directly to the reader
No jargon (but technical terms are fine for a technical audience)
No clichés or wordy phrases
Consistent words: using the same word for the same thing throughout the document
Only a few abstract nouns, e.g. words ending in -ment, -tion, -ance, -ence, -ancy, -ency, -ity, ism. Words positive in meaning and tone
Check readability
At least 60% score on Flesch Reading Ease
Tip: Use the grammar checker in your word processor to check your document's readability. The
Flesch Reading Ease score measures the percentage of adults who would be able to read your
writing easily. At least 60% of adults should be able to read your document easily. Just check the
prose, not data such as addresses.
Check design
The page looks orderly. Plenty of white space (in margins, between paragraphs etc), print so
that's big enough to read
PwC
Page 149
Structured Thinking Tools - Minto
Further reading
The Pyramid Principle, Logic in Writing and Thinking
Barbara Minto
The Economist Style Guide
Fowler’s Modern English Usage
RW Burchfield
Eats, Shoots and Leaves
Lynne Truss
Golden Bull Awards
plainenglish.co.uk
Plain English checklists
plainenglish.org.nz
PwC
Page 150
Structured Writing Tools – Summary
Summary
• Structured thinking tools
- Minto’s pyramid principle
- Mind-mapping
- Storyboarding
• Structured writing tools
- Minto’s pyramid principle
- Captive Moments
- “The Ministerial Three”.
PwC
Page 151
Thank you
Disclaimer
This document has been prepared solely for the purposes
stated herein and should not be relied upon for any other
purpose.
In preparing this document and providing our
recommendations, we have relied upon, and assumed the
accuracy and completeness of, all information available to us
from public sources and furnished to us by the Commission.
We have evaluated that information through analysis, inquiry
and review but have not sought to verify the accuracy or
completeness of any such information. It should not be
construed that we have conducted an audit of the information
we have used.
This document has been prepared solely for use by the Health
Quality and Safety Commission.
Our engagement did not constitute a statutory audit (the
objective of which is the expression of an opinion on financial
statements) or an examination (the objective of which is the
expression of an opinion on management’s assertions).
To the fullest extent permitted by law, PwC accepts no duty of
care to any third party in connection with the provision of this
document and/or any related information or explanation
(together, the “Information”).
Accordingly, regardless of the form of action, whether in
contract, tort (including without limitation, negligence) or
otherwise, and to the extent permitted by applicable law, PwC
accepts no liability of any kind to any third party and disclaims
all responsibility for the consequences of any third party
acting or refraining to act in reliance on the Information.
This document has been prepared with care and diligence and
the statements and opinions within it are given in good faith
and in the belief on reasonable grounds that such statements
and opinions are not false or misleading. No responsibility
arising in any way for errors or omissions (including
responsibility to any person for negligence) is assumed by us
or any of our partners or employees for the preparation of the
document to the extent that such errors or omissions result
from our reasonable reliance on information provided by
others or assumptions disclosed in the document or
assumptions reasonably taken as implicit.
We reserve the right, but are under no obligation, to revise or
amend the document if any additional information
(particularly as regards the assumptions we have relied upon)
which exists at the date of this document, but was not drawn
to our attention during its preparation, subsequently comes to
light.
This document is issued pursuant to the terms and conditions
set out in our Contract for services with the Health Quality and
Safety Commission.
© 2012 PricewaterhouseCoopers New Zealand. All rights reserved. PwC refers to the New Zealand member firm, and may sometimes refer to the PwC network. Each member firm is
a separate legal entity. Please see www.pwc.com/structure for further details.
PwC