Postoperative Pain Management
advertisement

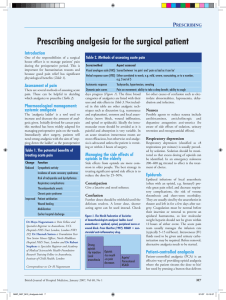
Postoperative Pain Management Negative Effects Of Pain • • • • • • • • Short term effects : Emotional and physical suffering; Sleep disturbance; Cardiovascular effects; Impaired bowel movement; Effects on respiratory function; Delayed mobilization, promotes thrombosis. Long term effects : Acute pain can lead to chronic pain; Behavioral changes in children for a prolonged period after surgical pain. Goals Of Pain Treatment Improve quality of life for the patient; Reduce morbidity; Facilitate rapid recovery and return to full function; Allow early discharge from hospital. Categories Of Pain Postoperative pain can be divided into acute pain and chronic pain: Acute pain is experienced immediately after surgery (up to 7 days); Pain which lasts more than 3 months after the injury is considered to be chronic. Types Of Pain • Somatic (from skin, muscle, bone); • Visceral (from organs within the chest and abdomen); • Neuropathic (caused by damage or dysfunction in the nervous system). Patients can experience more than one type of pain. Pain Pathway • • • • Perception Modulation Transmission Transduction Modulation of nociceptive pathways • Ascending Modulation (Gate control theory) – activity in A/ fibres inhibits transmission from nociceptive fibres to spinothalamic neurones; • Descending Modulation – stimulation of periaqueductal grey and nucleus raphe magnus inhibit nociceptive transmission. Gate Control Theory of Pain • Ascending Modulation (large diameter sensory fibers irritation): – Massage; – Heat and cold applications; – Transcutaneous electrical nerve stimulation (TENS). • Descending Controls – Endogenous opiate pathways from Periaqueductal gray matter – Descending norepinephrine pathways from the Locus Ceruleus – Descending serotonin pathways from the Nucleus Raphe Magnus 1 Principles Of Pain Assessment • • • • • • • Assess pain both at rest and on movement. Evaluate before treatment, than reevaluate after. If pain is intense, evaluate, treat, and re-evaluate frequently. On the ward, evaluate, treat, and re-evaluate regularly. Document pain and response to treatment, including adverse effects. Particular attention to patients who have difficulty communicating pain. Evaluate unexpected intense pain, particularly if associated with hypotension, tachycardia or fever. • Family members are involved when appropriate. Tools For Pain Assessment • • • • Facial expressions; Verbal rating scale (VRS); Numerical rating scale (NRS); Visual analogue scale (VAS). Currently the most frequently used approach to pain management is PRN based monotherapy. What’s wrong with this standard? Analgesic Gaps are specific periods of time when pain management is inadequate. By definition, PRN medications cause analgesic gaps (breakthrough pain). General principles of pain treatment • • • • Proactiveness; Multimodal approach; Escalating approach; Patient control Principles of pain treatment: Proactiveness. • • • • Evaluate, treat, and re-evaluate regularly. Define the intervention threshold. Give immediate pain relief without asking for a pain score to patients in obvious pain. Have predefined pain treatment plan ready and authorized. Principles of pain treatment: Multimodal Approach Pain is complex and multifactorial, thus appropriate management requires a “balanced” therapeutic approach. Benefits of multimodal approach: – higher effectiveness due to synergism; – lower side effects due to lower doses used; – flexibility. Principles of pain treatment: Patient Control PCA stands for “Patient Controlled Analgesia” - the intermittent administration of analgesic drug under direct patient control. In our hospital PCA means IV administration of Morphine. 2 Pharmacological Methods Of Pain Treatment Non-opioid analgesics Weak opioids Paracetamol (Acamol), Dipyrone (Optalgin) NSAIDs (including COX-2 inhibitors) Codeine Tramadol Morphine Strong opioids Pethidine Oxycodone Ketamine Adjuvant Gabapentine (Neurontin), Pregabalin (Lyrica) Clonidine, Dexmedetomidine (Precedex) Non-opioids: Paracetamol (Acamol) •Inhibits COX-3 in the hypothalamus, very low activity on COX-1, possible 5-HT activity. •No anti-inflammatory properties. •Rapidly absorbed from GI tract, reaches a peak plasma level in 30 to 60 min, rectally: 2-2.5 h. •Metabolized in liver; half life is ~ 2 hours. •Associated with hepatotoxicity when taken in large doses (10 to 15 g). Administration Dosage Comments Rectal;Oral (as soon as possible). 1 g x 4 /day PO, rectal dose 50% higher. Should be combined with NSAID and/or opioids or loco-regional analgesia for moderate to severe pain. Non-opioids: Dipyrone (Optalgin) • Popular in some regions (Middle East, Asia, S.Africa, S.America, part of Europe), but prohibited in others (USA, EU, Australia…). • Presumably inhibits COX-3 in spinal cord. • No anti-inflammatory properties. • IV administration can result in hypotension. • Questionable risk of agranulocytosis. Administration Dosage Comments IV, IM, Rectal; Oral (as soon as possible). The single dose in all age groups is 8 to 16 mg/kg BW up to 1g x 4/day, 3 days max. Should be combined with NSAID and/or opioids or loco-regional analgesia for moderate to severe pain. 3 Non-opioids: NSAIDs Intravenous (30-60 min before end of surgery); Administration Intramuscular (painful); Oral (as soon as possible). Monitoring Renal function in patients with renal or cardiac disease, elderly patients, or patients with episodes of severe hypotension. Gastrointestinal side effects. Comments Can be added to the premedication. Would be combined with proton inhibitors (i.e. Omeprasol) in patients at risk of gastrointestinal side effects. Analgesia •Ceiling effect; •Effects are evident in 1-2 hr; •Administration limited to 1-2 wks; If inadequate results, change to another NSAID. Opioids Opiate Receptors • Mu • Delta • Kappa Mu most important for analgesic actions. Opioids: problems… Side-effects: euphoria/dysphoria, constipation, respiratory depression, nausea/vomiting, urinary retention. Tolerance Definition: A change in the dose-response relationship induced by exposure to the drug and manifest as a need for a higher dose to maintain an effect. Develops at different rates to varying effects: respiratory depression, somnolence, nausea >> analgesia Analgesic tolerance is rarely a problem. Opioid doses remain relatively stable in the absence of worsening pathology and increased opioid requirements after stable periods is often a signal of disease progression. Dependence Definition: The development of a withdrawal syndrome following dose reduction or administration of an antagonist. Often develops after only a few days of opioid therapy. Not a clinical problem if drug is tapered before discontinuation. Taper by no more than 50% of the dose/day. Addiction • Compulsive use; • Loss of control; • Continued use despite harm to self and others. Risk of iatrogenic addiction in patients with pain and no prior history of substance abuse is extremely small. “Pseudoaddiction”- behavior that resembles addiction, but is driven by pain and disappear4 with adequate analgesia. Opioids: MORPHINE Intravenous Administration Subcutaneous (by continuous infusion or intermittent boluses); Intramuscular (not recommended). IV: Bolus: 2-3 mg each 5-10 min, up to 0.1- 0.15 mg/kg. Dosage SC: 0.1- 0.15 mg/kg 4 - 6/h IM: 5-10 mg 3 - 4 hourly. Monitoring Sedation, respiratory rate, nausea, vomiting, urinary retention. Oral Strong Opiates • No maximum dose for morphine; • No maximum dose for oxycodone alone; • Doses are limited with combination products. Morphine Immediate Release MSIR Controlled Release MS Contin Oxycodone Combination product Percocet® Controlled release Oxycontin® Transition From PCA To Orals • Give ~2/3 of previous 24 hour morphine requirements as OxyContin®; • Oxycodone for breakthrough. Opioids: CODEINE Administration Dosage Comments Oral 3 mg/kg/day (combined with Paracetamol) Analgesic action is likely to be due to conversion to morphine. Part of patients derive no benefit due to absence of the converting enzyme. Equianalgesic Doses of Opioid Analgesics PO / PR Analgesic SC / IV / IM 200 Codeine - 30 Morphine 10 20 Oxycodone - - Fentanyl 0.1-0.25 5 Opioids: TRAMADOL Intravenous; Administration Intramuscular; Oral (as soon as possible). Dosage Mechanism of action 50-100 mg 6h; reduces serotonin and norepinephrine reuptake and is a weak opioid agonist Side effects nausea and vomiting Comments 100 mg is equivalent to 5-15 mg Morphine; ~ 7% is "poor metabolizers”. Oxford Analgesic League Table (NNT) Ibuprofen 800mg 1.6 Ketorolac 60mg IM 1.8 Diclofenac 100mg 1.9 Rofecoxib 50mg 1.9 Celecoxib 400mg 1.9 Paracetamol 1G + Codeine 60mg 2.2 Pethidine 100mg IM 2.9 Morphine 10mg IM 2.9 Paracetamol 1000mg 3.8 Tramadol 100mg 4.8 Adjuvant Ketamine; Magnesium; Corticosteroids; Clonidine - Normopresan; Dexmedetomidine - PRECEDEX®; Gabapentin - Neurontin®; Pregabaline - Lyrica®. 6 Epidural Analgesia Dosage • • The response is not the same if the same dose is used but in a different volume and concentration. A higher volume of a low concentration of LA will result in a larger number of segments blocked but with less dense sensory block and less motor block. Local anesthetics in epidural space produce three types of blocks: – sympathetic; – sensory; – motor. The resulted block is concentration depended, the sympathetic block is been appearing first. Postdural puncture headache (PDPH). • • • Results from the tension force applied to meningeal and vascular structures. May herald incipient cerebrovascular accident. Treatment: – simple analgesics; – bed rest; – fluid hydration; – an epidural blood patch after 24 hours. Peripheral nerve block PNB is induced by injecting LA near the course of nerves or plexuses. • Cervical plexus; • Brachial plexus; • Lumbar plexus; • Sacral plexus. Cervical plexus • The cervical plexus is formed from the first four cervical nerves (C1-C4). • The most common clinical use for this block is for carotid endarterectomy. • Phrenic Nerve from C3 & C4 & C5 Brachial Plexus • Interscalene; • Supraclavicular; • Infraclavicular; • Axillary. 7 Comparison of regional analgesia techniques Advantages Continuous Epidural Analgesia (CEA) Continuous Peripheral Nerve Blocks (CPNB) Disadvantages •Much experience; •Excellent pain control over an extended period; •Differential block with motor sparing is possible. • • • • • • Better efficacy than parenteral opioids and comparable to epidural; Lower incidence of side effects than with epidural; Excellent pain control over an extended period. • • Motor block and urinary retention may develop; Requires regular clinical monitoring; May risk a spinal haematoma or abscess. Slower learning curve; Higher incidence of technical problems. Regional anesthesia: COMPLICATIONS. Intravascular injection. Arterial injection: direct injection into the vertebral or carotid artery immediately manifests as a seizure (most common with interscalene block). The convulsant dose after an unintentional arterial injection is 14.4 mg of lidocaine or 3.6 mg of bupivicaine. Larger doses of anesthetic are tolerated from venous injection. Unintentional subarachnoid or epidural injection. LA intended for plexus block may spread to the neuraxis. Interscalene block in particular has been linked to unintended spinal and lumbar plexus block is prone to epidural spread. Nerve damage. Regional Anesthesia. Direct nerve damage 1 in 10,000–1 in 30,000 Significant permanent nerve damage less than 1 in 100,000 Spinal haematoma 1 in 150,000–1 in 220,000 Spinal infection 1 in 100,000–1 in 150,000 Nerve Damage. Central Blocks • Direct injury caused by the needle or the catheter; • Haematoma; • Infection, Abscess; • Inadequate blood supply; • Other causes (wrong drug administration). Nerve damage. Peripheral Blocks. Most present as a residual paresthesia or hypoesthesia and rarely as paresis. The median presentation is 3 days post op. Permanent nerve damage is ~ between 1 in 5,000 and 1 in 30,000 nerve blocks. Symptoms lasting more than one week happen in 1–5%; 8 92–97% recover within 4 to 6 weeks, 99% recover within a year.