Documentation Guidelines Job Aide
advertisement

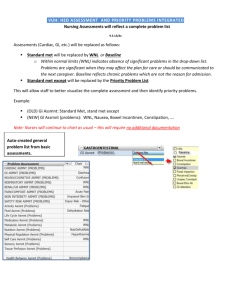
Documentation Guidelines : A summary of when to document what Admission Beginning of Shift • Complete Admission History in StarPanel within 24 hrs. of admission • Assess ALL Care Categories, noting baseline status. If using WEL& OEL enter an annotation with supporting information. • Document Care Contact & VUMC general & unit specific orientation in Education Tab • Assess Care Categories in ALL CAPS + others based on problems or risk for problems • Denote Priority Problems for shift w/ !! & set goals for each priority problem. • Document Interventions in real time or near real time through the shift. • Document either “unchanged” or “unchanged except” & denote changes for OEL, problems, risk for problems or based on orders &/or nursing judgment. DO NOT document on those wnl. Focused Re- • ICU – at least two more times during the shift assessment • Acute Care – at least once during the shift PreProcedure or Transfer End of shift Discharge • Focused reassessment, note new, resolved, or unchanged problems • Summarize response to care focus on priority problems; Identify issues for f/u by receiving nurse; avoid duplication • Enter interventions, vitals, I&O, & meds • Summarize response to care focus on priority problems; Identify issues for f/u by receiving nurse; avoid duplication • Ensure all assessment, interventions, vitals, I&O, meds documentation is up-to-date • Summarize response to care, focus on unresolved problems and action plan post discharge; avoid duplication • Ensure all assessments, interventions, vitals, I&O, meds documentation is up-to-date NEED TO KNOWS…. Modified Charting by Exception – To reduce repetitive charting of normal assessment detail , nurses chart within normal/expected limits (WNL, WEL) for each care category omitting normal findings except for normal values needed for decision support (Braden, Morse, RASS). WNL – Within normal limits. Meets standard criteria for developmental age. Use Hover over feature to display WNL criteria. WEL – Within expected limits ( previously baseline). Does not meet all the standard criteria for development age, but is expected for patients in this clinical phase (post-op) or normal for patient. Does not require measures beyond the standard of care. Requires supporting documentation of finding upon admission assessment only ( example- Right AKA x 4 years, non symptomatic a fib x 3 years, groggy from anesthesia for immediate post op pt) OEL – Outside expected limits - Does not meet criteria for WNL or WEL but has not risen to the level of a problem. Need to continue to evaluate to see if problems develops. No additional or special care needed except to include this in the next focused assessment. (example-hypoactive BS but no other GI Issues, tachycardia for pt w/ fever, jaundice for pt with liver failure) Requires supporting documentation of findings with each shift assessment. Problems (Nursing diagnoses) require targeted interventions and should be a significant focus of the plan of care (eg. Incision) Requires supporting documentation of findings with each shift assessment Priority problems Priority problems are flagged in red and represent the most important shift focus based on patient (eg pain), team (eg oxygenation) and nurse’s assessment of risk (eg skin integrity) . They require measureable goals and outcomes are described in the Response to Care narrative statement. Requires supporting documentation of findings with each shift assessment. Interventions – Reflect implementation of the plan of care (Assess, Care, Teach, Notify) based on provider orders, VUMC Policy & Procedure, and published Nursing standards of care (ie Mosby). My Notes: Assessment Documentation All care categories require documentation on admission. Assessments shown in all capital letters are required documentation every shift. Focused re-assessment is done if the initial assessment for that category was outside expected limits or if the patient unstable, is at risk for, or has an existing problem for that care category. Data Display Before you click on “chart” the display of the data has been collapsed to facilitate easy viewing. Data displays in 1 hour increments VS/I&O Assessment Interventions Pain/CDR Device Protocols Displays in 12h increments Plan ALL DOCS Displays in 24h increments Education FOCUSED REASSESSMENT if problem/risk if problem/risk if problem/risk CARE CATEGORY ADM QSHIFT + - PAIN - NEURO - CARDIAC X X X X X X - Vascular/Perfusion X - RESPIRATORY X X if problem/risk GASTROINTESTINAL X X if problem/risk X X X X X X if problem/risk if problem/risk if problem/risk - SAFETY/FALL RISK - SKIN/WOUND - URINARY/RENAL Activity/Musculoskel etal - Fluid/Nutrition - Medication if problem/risk X if problem/risk X X if problem/risk if problem/risk Infectious/Metabolic X if problem/risk - Psychosocial - Reproductive - Self-care (ADL) X OB X if problem/risk if problem/risk if problem/risk