Presentation Slides - The Open University
advertisement

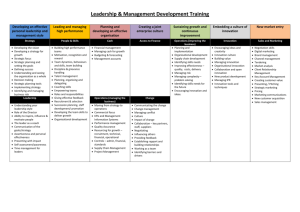
Building Capacity for Health Workers in Developing Countries: M-Libraries concept/proposal Adesina Iluyemi adesina.iluyemi@port.ac.uk Mobile ICT in Africa • Up to 300 million GSM mobile users in Africa • Similar figures in India, China and South America • Mobile ICT impact and growth in Africa – Increased GDP – Individual and personal empowerment – Business process transformation (m-commerce) Health Workers in Africa • • • • Delivers essential primary care services Agents of Change and health promoters Brain drain Community/facility based care (HIV/AIDS, TB, Malaria etc) • Information, communication & logistic needs • Work as individuals & in teams • But issues of organisational and end-users context need to be considered Different users’ Context • CBHWs – Remote, Local & Fixed mobility • Clinicians, Managers, Administrators, Technicians – Local & Fixed mobility (Remote?) • Context modulates devices and connectivity access mHealth-Libraries Process • Process Collection Transmission Presentation • Geography: Rural or Urban • Facility: Community vs. Hospital/Clinics • Users: – Community Based Health Workers (CBHWs)- Volunteers, salaried, Mid wives. (Community Level) – Doctors, Nurses (Hospital/Clinic) – Managers/Administrators M-Libraries: A rethink • Libraries means database or repositories (Traditional or Electronic) • Re-conceptualizing M-Libraries in developing countries within the wider eHealth paradigm • To improve adoption and diffusion • For mainstreaming and sustainability • What is eHealth? eHealth as a developmental tool • eHealth is the use of information (data) and communication technologies for health processes (Health System) either locally and at a distance (WHO 2005). • Also health workers and health system capacity • For improving patients’ outcomes • eHealth involves health management information systems, (EHR, DSS etc) health knowledge systems (Libraries) . • The combination of mobile/wireless technologies with eHealth is known as mHealth • Instead of M-Libraries should be “mHealth Libraries” Rationale: Rethinking M-Libraries • Mobile/Wireless ICTs provide the most appropriate and Low-cost for bridging digital divide in developing countries (Africa) (ITU 2007). • Future mobile ICTs trend demonstrate cheaper, increased capacity and availability • Why? Rethinking M-Libraries : Wireless/Mobile tools • Wireless technologies use: GSM/GPRS/3G, WiFi, WiMAX, WLL (Fixed or Mobile CDMA), Broadband wireless, Satellite, VSAT (Mobility vs Universal Access) • Mobile devices: PDAs, Smartphone, Cellular phones, Tablet PCs, Laptops, smart cards, memory sticks, USB keys, sensors. Rethinking M-Libraries : Applications • Electronic Health Records • Health data collection • Health Management Information System, Continuing medical education (CME)/eLearning • Laboratory Information System • Drug management system • Telemedicine Proposed Model: Context and Technology mHealth-Libraries Technology CME CME Human & Organisational issues mHealth-Libraries EHR HMIS DDS DDS EHR HMIS Mobile Devices HEALTH HEALTH WORKER WORKER Facility & Community Levels Integration Interoperability Connectivity Access Mobility mHealth Libraries: Different faces • mHealth Libraries in developing countries have different presentation • Depending on the mHealth technology available • Cases to illustrate below the applications mHealth-Libraries: Case Study 1 • UHIN (Uganda) – Started in 2003 and has continued to expand within & beyond the Country (Mozambique). – Uses existing GSM/GPRS/ WiFi links with PDAs to support (community) health workers (HWs) creating a regional eHealth network – Uses solar panels for power – For Primary Health Care service provision – Provides learning materials, health information and e-mail (upcoming) to HWs mHealth-Libraries: Case Study 2 • Cell-Life (South Africa) – Started in 2003 by 2 universities in SA – EHR for the therapeutic and logistic management of HIV/AIDS population – Mobile devices (Cellphones & PDAs) with 3G/GPRS/SMS networks – Enable community health volunteers to assist their fellows HIV+ management. mHealth-Libraries: Case Study 3 • MindSet Health (South Africa) – Started about 2002 – Uses DVB wireless satellite technology to provide – Health education (eLearning) to rural health workers in clinics and hospital (datacasting) through PCs/Laptops – Health promotion to patients and citizens through large screens and TVs (broadcasting) in clinics and community settings in form of documentaries, drama etc. – Delivers health information all aspects of health (TB, HIV, Malaria etc). – Improves health workers’ capacity and empowers citizens’ to keep healthy mHealth-Libraries: Case Study 4 • EHAS (Peru) – Started in Peru is early 2000 with joint collaboration between a Spanish and two Peruvian universities & MoH and an international NGO – Initially with HF/VHF but now with long distance WiFi wireless links connected with Laptops creating a regional eHealth network – Uses solar panels for power – For Primary Health Care service provision – Provides learning materials, e-mail and voice communication and teleconsultation to HWs , organisational health information & data exchange Issues & Barriers • Understanding context for sustainable mHealth-Libraries in developing countries • End-users • Technological • Organisational Success & Failure from Developing countries • 2 cases will be employed for illustration • Could provide “bottom-up” experience to mHealth Libraries implementation • India • Uganda IHC-Case • • • • • • • India: The India Health Care (IHC) project Started in 1994 (Apple Newton) 2001 new PDAs (Compaq Ipaq, Simputer) Closed in 2003 CBHWs, mostly women Primary Health Care Standalone 200 PDAs deployed India: IHC case • Purposes – Digital data collection – Improved and timely data collection process – Decision support system for immunization management – CBHWs’ workflow process planning and coordination • Outcome: Failure! Why? Technological • Technical – Insufficient memory (I6MB?) (technical) – Low Battery life – Low processing speed – Poor software design • (These accounted mostly for the failure rate) Organisational • Process – High health needs and demand – Poor HIS & database design – Perceived high cost of the PDAs – Lack of ownership due to fear of financial responsibility – Lack of piloting or modular approach – Lack of technical support and poor maintenance process Users’ impact & Outcome (Negative) • Users’ impact – Low users’ adoption due to duplication of efforts – Poor Human Computer Interface (HCI) design – Eye sight and visibility issues (Black and white screen & Sunlight) – Lack of adequate training provided • The failure of this programme is due to improper recognition, analysis and management of human and organization issues (BEANISH 2006). Uganda UHIN: A contrast • Organisational behaviour – – – – – – – – – Improved organisational efficiency Modular and iterative approach Local ownership (UCH, a research of the university) Multiple applications Choice of PDAS? (Palm vs. Pocket PC) (Linux?) Networked devices (GSM, GPRS, WiFi?) Solar panels ($30) Local production Local contents development Open source software • End users’ behaviour – Health workers’ integration – Health workers’ ownership – Health workers’ usage and adoption End-Users Issues • Technical – Human Computer Interface (HCI) – Open Source (Hardware & Software) • Social – Adoption issues (Development & Implementation) – Culture – Local Knowledge Human Issues: Technical • HCI – Screen size and design (Adaptive) – Power- Solar? (Global Green Movement) – Memory (Stable and Labile) – Security – Structure- (Ruggedized) – Connectivity – Network ConfigurationThin & Thick clients, remote & located synchronisation Low-cost devices • One Child Per Laptop , Simputer, • Intel Classmate • RM Asus MiniBook - Linux • Open Source? • Interface • Open Source • Multi-wireless connectivity Human Factors: Social Issues • Doctors in South Africa (Banderker et al 2005) – Job relevance – Usefulness – Perceived User resources – Device Characteristics – Supports from Public National government & hospital administrators – Patient influence – Legal issues (Decision Support Systems, Drug directories) Organisational Issues Technology • • • • • Technology is not enough! Positive economic benefits Users led and focus Social and ethical issues Health workers’ responsibility • Device and applications development and regulation. (HealthService 24- 2006) Environment • Health Policies, regulation, structure and financing • Evaluation in real-life contexts • Multiple actors and structures • Health IT infrastructure (organisation). • Users’ Trust • Users’ led model (MOSAIC -2005) Organisational issues • Adequate mobile ICT access and equity procedure is necessary • Facility based technical support important • Re-engineering of organisational & work process required for mHealth-Libraries • Standards for data sharing & communication important for success- Different databases • Appropriate mobile devices for tasks i.e voice vs. data – Podcasting- Medical lectures – RSS feeds Organisational issues • • • • • Policies Telecommunication Health System reform Low-cost devices ( Digital World) HWs’ primary tasks should be protected from interferences • HWs’ views and empowerment is very important • Content development and adaptation very important • (HIFA 2015 project). Conclusion • mHealth-Libraries have is applicable for health development in developing countries • Barriers should be evaluated, understood and tackled Thank you Open University! Adesina Iluyemi CHMI, UK adesina.iluyemi@port.ac.uk Policy implications and Change Management in the implementation & use of mobile/wireless eHealth in Africa’s Health Systems