Document
advertisement

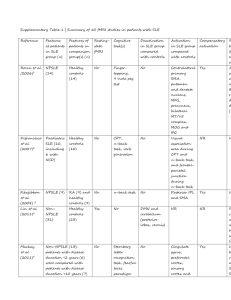
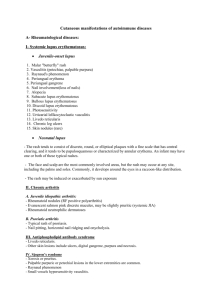
Connective Tissue Diseases Digital Lecture Series : Chapter 19 Dr. Vinitha Varghese Panicker Associate Professor, Department of Dermatology, Amrita Institute of Medical Sciences & Research Centre, Cochin CONTENTS Lupus erythematosus (DLE / SCLE / SLE) Scleroderma (Morphoea / Systemic Sclerosis) Dermatomyositis / Polymyositis Rheumatoid arthritis Sjogren’s syndrome Mixed connective tissue disease Antiphospholipid antibody syndrome MCQs Photo Quiz Lupus Erythematosus (LE)- Types Cutaneous lupus erythematosus is classified into three subtypes: Acute cutaneous lupus erythematosus (ACLE): Malar rash, Morbilliform rash, bullous lesions Subacute cutaneous lupus erythematosus (SCLE): Annular, Papulosquamous Chronic cutaneous lupus erythematosus (CCLE): Discoid Lupus Erythematosus Pathogenesis of Cutaneous LE Genetic Factors - HLA susceptibilty Environmental triggers UV exposure induces cytokine release and apoptosis. Immunologic factors Malfunction of T regulatory cells (T reg) Role of IL-18 Acute Cutaneous LE Localised ACLE Characteristic butterfly facial rash Generalised ACLE Widespread maculopapular rash in a photo-distributed pattern Subacute Cutaneous LE Non - scarring; papulosquamous / annular polycyclic lesions. Vesiculation, crusting, hypopigmentation, telangiectasia, alopecia, photosensitivity, Raynaud’s phenomenon. Sites : above waist, neck, arms. Systemic involvement 35%. ANA, anti - Ro, anti - La. Chronic: Discoid Lupus Erythematosus (DLE) DLE is a relatively benign disorder of the skin, characterized by well defined, reddish, scaly patches which tend to heal with atrophy, scarring and pigmentary changes. The histology is characteristic. Female : Male - 2 : 1 Onset - second-fourth decade of life Family history : 4% Genetic factors - HLA B7, B8 Discoid rash Diagnosis Histopathology : Epidermal atrophy, basal layer liquefaction, lymphocytic dermal infiltrate and ‘Civatte bodies’. Differential diagnosis : Polymorphous Light eruption, Morphoea, Lichen planus, Lupus vulgaris, Sarcoidosis. Systemic LE Definition : A systemic disease with immunopathological abnormalities affecting various organs particularly the skin, joints and vasculature. • Females > males • Onset: early adult life Clinical features Fever (52%), lymphadenopathy Arthritis (84%) and arthralgia Cutaneous lesions : specific and non -specific Raynaud’s phenomenon Renal - nephritis or as nephrotic syndrome. Lung-pleural effusion, alveolitis, interstitial lung disease Cardiac-pericardial effusion, myocardial infarction, Libman-sacks endocarditis CNS involvement : migraine, epilepsy, neuropathy. GIT and hepatic involvement : vasculitis of gut, ascites, pancreatitis, autoimmune hepatitis. Splenomegaly, hepatitis, cirrhosis. Hematologic-Anemia, leukopenia, Thrombocytopenia. Ocular - Conjunctvitis, episcleritis, Retinal vasculitis. Cutaneous lesions LE specific • ACLE – Malar rash • SCLE – Annular, Psoriasiform • CCLE – Plaque Lupus panniculitis Hypertrophic Tumid CCLE Chilblain CCLE Mucosal CCLE Malar rash Oral ulcer LE Non specific lesions Vascular: Telangiectasia, Purpura, Thrombophlebitis, Raynauds phenomenon, livedo reticularis, erythema multiforme Alopecia: Lupus hair, Alopecia Areata, Scarring Alopecia Mucus membrane lesions Nail changes Calcinosis cutis Bullous lesions Urticaria Pigmentary abnormalities Sclerodactyly and sclerodermatous changes Papulonodular mucinosis Anetoderma Lichen planus Porphyria cutanea tarda Contd… Special subsets of LE SLE in pregnancy Neonatal LE Drug induced LE Childhood SLE Rowell’s syndrome Investigations CBC : anemia , leukopenia , thrombocytopenia ESR : raised Urine analysis, BUN, S. Creatinine False positive VDRL & RA factor LE cell test ANA Anti-DNA, anti-Sm, anti-histone, cryoglobulins, serum complement levels DIF – Lupus band test ANA Patterns ANA PATTERN PREDOMINANT ANTIGEN DISEASE PERIPHERAL nDNA SLE HOMOGENOUS nDNA, histones SLE NUCLEOLAR Nucleolar RNA SSc, SLE CENTROMERE Kinetophore CREST syndrome SPECKLED Various RNPs MCTD, SLE, SSc, Sjogrens syndrome American College of Rheumatology, ACR criteria Malar rash Discoid rash Photosensitivity Oral ulcers Non–erosive arthritis Serositis : pleurisy or pericarditis Renal disorder : persistent proteinuria (>0.5g/day) or cellular casts Neurological disorders : seizures or psychosis Contd… American College of Rheumatology, ACR criteria Haematological disorders - heamolytic anemia or leukopenia (<4000/mm3) or lymphopenia (<1500/mm3) or thrombocytopenia (<1,00,000/mm3). Immunological disorder - LE cells, or anti-dsDNA antibody or anti Sm antibody or false positive VDRL. Antinuclear antibodies. 4 or more criteria are required for definitive diagnosis. SLICC CRITERIA (Systemic Lupus International Collaborating clinics) Clinical and Investigative criteria Acute or subacute cutaneous lupus Chronic cutaneous LE Oral/nasal ulcers Non Scarring Alopecia Inflammatory synovitis Serositis Renal-Rbc casts, urine protein/creatinine atleast 500 mg protein/24 hr Neurologic Hemolytic anemia Leukopenia (<4000/mm) atleast once or lymphopenia (<1000/mm) atleast once. Contd… SLICC CRITERIA (Systemic lupus International Collaborating clinics) Thrombocytopenia Immunologic criteria – • ANA above reference range • Antids DNA above lab ref range • Anti-Sm • Antiphospholipid antibody • Low complement-C3,C4,CH50 • Direct Coombs test in absence of hemolytic anemia Patient may be classified as having SLE if: patient has biopsy proven lupus nephritis with ANA or ds DNA antibodies or if they satisfy 4 criteria including at least one clinical/ one immunologic . Treatment Mild disease NSAIDs, topical therapy, antimalarials Severe disease Systemic steroids Steroid sparing immunosuppressants - Azathioprine, Cyclophosphamide, Mycophenolate mofetil Biologics - Rituximab-monoclonal ab targeting CD20 receptor protein on surface of B cells-mainly for arthritis and proteinuria. Morphoea Definition : Sclerosis confined to the skin, localised or generalized is termed as ‘Morphoea’. Female : Male - 3 : 1 Onset : 20 - 40 years; Precipitating factors : Trauma, vaccination, radiotherapy, hormonal factors, borrelia infection, measles, silicone implants. Types of Morphea Plaque type - morphea en plaque, guttate morphea, keloid (nodular) morphea, atrophoderma of Pasini and Pierni. Generalised morphea Bullous morphea Linear morphea - linear type, en coup de sabre, progressive hemifacial atrophy. Deep Morphea - Subcutaneous morphea, eosinophilic fasciitis, morphea profundus, disabling pansclerotic morphea. Clinical features Plaque type - Round or oval indurated plaques with lilac border. Heals slowly with residual hyperpigmentation. Multiple, asymmetrical distribution. Sites : trunk, limbs, face. Linear Morphea Plaques of morphea in linear arrangement mainly on limbs Type on frontoparietal region - en coup de sabre En-Coup-de-Sabre Treatment Triamcinolone acetonide, 10 - 40 mg/ml intralesional injection Penicillamine : 300 - 600 mgs / day Diphenylhydantoin Systemic steroids Cyclosporine, Topical Vit. D3 analogues Topical tacrolimus Phototherapy, plasmapheresis, physiotherapy, plastic surgery Systemic Sclerosis Systemic sclerosis is a multisystem autoimmune disorder characterized by vascular abnormalities, connective tissue sclerosis and atrophy . Females : Males - 5.2 : 1 Onset : Fourth decade Etiology and pathogenesis : complex autoimmune disease charecterised by immune activation, fibrosis of skin and obliterative vasculopathy. Classification According to Skin sclerosis Limited Cutaneous Scleroderma - skin sclerosis of fingers (sclerodactyly) with or without mild sclerosis of face, neck and armpits. Diffuse cutaneous Scleroderma - Diffuse and truncal sclerosis. Immediate cutaneous scleroderma - Sclerosis of upper and lower limbs, neck and face without truncal involvement. Sine scleroderma SSc - Absence of cutaneous sclerosis with typical visceral organ involvement, capillaroscopy changes and serum autoantibodies. Cutaneous features Raynaud’s phenomenon ‘Hide-bound’ skin Classical sclerodermoid facies- “mask-like” face, pinched or beak-like appearance of nose, radial furrows around the mouth and thinning of the upper lip Pigmentation – mottled or hyperpigmentation Swelling of hands & joints, atrophy Finger and leg ulcers, digital gangrene, stellate scars Nail fold telangiectasias Calcinosis Features of syctemic sclerosis Classical sclerodermoid facies Pitted scars Systemic Features Gastrointestinal and Hepatic - Esophageal Dysfunction, malabsorption, primary biliary cirrhosis, Autoimmune hepatitis. Arthritis, tendon friction rubs. Renal-scleroderma renal crisis (most severe). Lung-Interstitial lung disease, Pulmonary hyertension. Cardiac-myocardial disease, pericardial involvement. Muscle-SSc Associated myopathy more common in diffuse SSc. Diagnosis 2013 ACR/EULAR criteria Skin thickening of the fingers extending proximal to MCP jts is sufficient to diagnose the patient as SSc. If this is not present seven other features apply with for varying weights for each • Skin thickening of fingers • Finger tip lesions • Telangiectasia • Abnormal nail fold capillaries • Interstitial lung disease or pulmonary artery hypertension • Raynaud’s phenomenon • Ssc related autoantibodies (anticentromere, antitopoisomerase, antiRnp-3) Investigations Serology - ANA, anticentromere antibodies, anti-Scl 70 antibody Pulmonary Function test -Detect fibrotic changes Histopathology - Hyalinization and homogenisation of collagen, dermal lymphocytic infiltrate. ECG- To detect rhythm and conduction abnormalities. ECHO- Detect pulmonary artery hypertension. GI involvement- Esophageal manometry, endoscopy, barium studies. Contd… Treatment Use of gloves For Raynauds - nifedepine (mild cases), sildenafil, iloprost, low molecular weight dextran. Corticosteroids Immunosuppressants : Methotrexate, Cyclophosphamide Penicillamine, colchicine, interferons. Symptomatic treatment for pulmonary, cardiac, renal and GIT symptoms. Dermatomyositis An idiopathic inflammatory myopathy characterised by muscle weakness and cutaneous eruption. Females > males Bimodal peak during childhood and then between 50-70 yrs ETIOLOGY HLA-B8, DRB1*0301, DQA1*0501, DQA1 *0301 Infections - Gr A Beta hemolytic streptoccoci, toxoplasma, coxsackie UV radiation exposure Drugs-d penicillamine, tamoxifen, INH, penicillins Cutaneous features Pathognomic skin manifestation - Gottrons papules and Gottron’s sign. Gottrons papules - violaceous papules overlying the dorsal interphalangeal and metacarpophalangeal joints, elbows and knees. Gottrons sign - erythematous or violcaeuos erythema with or without edema. Characteristic skin lesions - heliotrope erythema and macular violaceous erythema over the deltoids, posterior shoulders, nape of neck, upper chest (V sign), forehead and dorsa of hands. Cutaneous calcinosis more common in JDM, 40-75% cases. Heliotrope Gottron’s papules Systemic manifestations Muscle : Progressive symmetric proximal myopathy; pharyngeal and respiratory muscles may be involved. Joints : Non erosive arthritis, usually an early manifestation. Pulmonary : Aspiration pneumonia, Interstitial lung disease, Hypoventilation. Cardiac : Arrythmia , conduction abnormalities myocarditis. Gastrointestinal : Dysphagia, esophageal reflux. Criteria for diagnosis (Bohan and Peter) Symmetric muscle weakness Elevation of skeletal muscle enzymes Abnormal EMG results Muscle biopsy results Typical rash of DM Definite diagnosis : characteristic skin rash + ¾ remaining criteria . Investigations Muscle enzymes : CK, SGOT, SGPT, LDH, S. Aldolase CK - MM fraction most specific for skeletal muscle Muscle biopsy - definitive diagnosis EMG MRI - may detect subclinical muscle involvement . Serology : ANA, anti Jo - 1, anti - Mi 2 Treatment Corticosteroids Immunosuppressants : Methotrexate, Mycophenolate mofetil Cyclophosphamide, Azathioprine Methotrexate considered first choice among adjuvants IV Ig - refractory cases Rituximab Exercise and physical therapy Cutaneous lesions - Sunscreens, Hydroxychloroquine, Calcinosis - alendronate, diltiazem, excision of large lesions Mixed Connective Tissue Disease Affects predominantly females Features of SLE, systemic sclerosis, dermatomyositis, polymyositis Specific antibody to U1-RNP. Raynaud’s phenomenon, arthritis, arthralgia, sausage shaped fingers, swelling of hands, photosensitivity, SCLE like rash. Abnormal oesophageal motility, impaired pulmonary diffusing capacity, myositis, aseptic meningitis, psychosis, trigeminal neuropathy. Sjogrens Syndrome Xerostomia with keratoconjunctivitis sicca Cutaneous features : Xerosis, Generalised pruritus, Loss of sweating, Diffuse alopecia, Recurrent annular erythema. Raynaud’s phenomenon, Non thromobocytopenic Purpura, Urticarial vasculitis, necrotising vasculitis, splinter hemorrhages, gangrene. Cutaneous Manifestations of Rheumatoid Arthritis Specific manifestations : Rheumatoid Nodules - most frequent extra-articular manifestation. Granulomatous dermatitis - linear erythematous to violaceous subcutaneous bands in axilla, trunk, inner aspect of thighs. Rheumatoid Vasculitis - Ulcers, digital infarcts, nail fold infarcts (Bywaters lesions) Pyoderma gangrenosum Feltys syndrome Juvenile onset RA Non Specific Manifestations : Palmar erythema, sclerodactyly like changes, periungual erythema, splinter hemorhages, bluish discoloration of fingers. Antiphospholipid Antibody Syndrome Primary and Secondary Secondary causes include - autoimmune connective tissue diseases, Takayasu’s arteritis, bacterial and viral infections, malignancies, dialysis in renal failure. Approx 40% have cutaneous manifestations. Livedo reticularis most common. Others - necrotising vasculitis, thrombophlebitis, cutaneous ulcers, gangrene, necrosis, purpura, erythematous macules, ecchymoses, painful skin nodules, anetoderma, atrophie - blanche like lesions, subungual splinter hemorrhages. MCQs Q.1) A. B. C. D. Carpet tack sign is seen in SCLE DLE SLE Bullous LE Q.2) A. B. C. D. Rowells syndrome is Lupus panniculitis LE and EM like lesions LE and Scleroderma Neonatal LE MCQs Q.3) A. B. C. D. Pathognomic skin lesion of Dermatomyositis Gottron’s papules Heliotrope erythema Shawl sign Poikiloderma vasculare Q.4) A. B. C. D. Water melon stomach is seen in SLE Systemic Sclerosis Dermatomyositis MCTD MCQs Q.5) 53 year old lady presents to the medical assessment unit with a flu-like illness and myalgia. In the last few days she has noticed a rash across her back. She has no other symptoms. On examination she looks unwell. There is an erythematous rash across her back. She has grade 4/5 weakness proximally. Her CK which is elevated at 1052 IU/l. Her renal function is normal. What is the diagnosis? A. SLE B. Systemic Sclerosis C. Dermatomyositis D. Antiphospholipid antibody syndrome Photo Quiz Q. Identify the condition. Photo Quiz Q. Identify the condition. Photo Quiz Q. Identify the condition. Thank You!