Heterogenity of AF - The Egyptian Cardiac Rhythm Association
advertisement

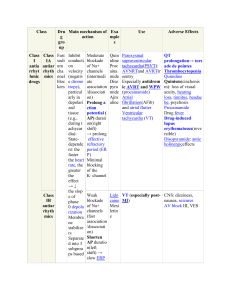
Heterogeneity Of AF Not all AF are the same!!!!!! Dr.Mervat Aboulmaaty Prof. of cardiology Ain Shams university 2008 Heterogeneity Of AF Not all AF are the same!!!!!! Heterogeneity Of AF Not all AF are the same!!!!!! AF with fast vent response & aberrancy AF with controlled vent. response AF WITH LBBB AF with IVCD AF regular because of VT Atrial Flutter/AF AF and AT Flutter AF WITH SLOW VR AF with CHB AF with WPW syndrome AF with WPW syndrome AF degenerating to VF AF in Patient with CHF and CRT AT Flutter and 1:1 conduction After CV A-Pacing Native Conduction AF Heterogeneity Prevalence AF prevalence doubling with each decade ◦ 0.55 at age 50-59 years ◦ 9% at age 80-89 years 3-fold increase in men New onset AF: men are 1. 5 times as likely as women to develop it Incidence of AF in Men and Women Associated conditions with AF Reversible Causes of Atrial Fibrillation alcohol intake (“holiday heart syndrome”), surgery, electrocution, MI, pericarditis, myocarditis, PE, pulmonary diseases, hyperthyroidism with Atrial flutter, WPW,AVNRT, AVRT complication of cardiac or thoracic surgery Associated conditions with AF Acute and chronic coronary disease HTN Hypertrophic ,dilated & restrictive CM ASD Valvular Rheumatic 40% MS 75% MR Cardiac conditions increasing the risk of AF Men Women 20% 31% HF 4.5% 5.9% Valve disease 1.8% 3.4 % Myocardial infarction 40% 20% Atrial Fibrillation Without Associated Heart Disease lone AF Lone AF before age 60 yrs without HTN or overt structural HD (clinical exam, ECG and echo) 30% to 45% of paroxysmal AF and 20% to 25% of persistent AF occur in younger patients without underlying disease AF can present as an isolated or familial arrhythmia In elderly, ◦ myocardial stiffness may be associated with AF, ◦ Heart disease may be coincidental and unrelated to AF. AF and autonomic influence Vagal predominance in the minutes preceding the onset of AF Vagally mediated AF occurs at night or after meals Cholinergic agents such as disopyramide are helpful to prevent recurrent vagally mediated AF Adrenergically induced AF occurs during daytime in pts with organic HD Beta blockers for adrenergically induced AF Autosomal dominant hereditary AF Mapping analysis of the AF family ECG and missense mutation DNA and amino acid sequence of KCNQ1 missense mutation associated with affected members in the AF family. DNA sequence analysis revealed an A to G substitution causing an S140G mutation in the S1 segment of KCNQ1. AF family with an autosomal recessive inheritance pattern AF in the family manifests with early onset at fetal stage and is associated with neonatal sudden death Some cases ventricular tachyarrhythmias and cardiomyopathy. Heterozygous carriers have significant prolongation of P-wave duration compared with non-carriers The maximum multipoint LOD score of 4.10 was obtained for 4 markers: D5S426, D5S493, D5S455, and D5S1998. Circulation. 2004;110:3753-3759 Genetic map with chromosome 5p13 markers and location of putative arAF1 gene Patterns of AF Mechanisms of AF Rapidly firing atr automatic foci PV triggers Anatomical substrate for reentry within the PV Symptoms of AF Embolic complication Exacerbation of HF Palpitations, chest pain, dyspnea, fatigue, lightheadedness Syncope. ◦ upon conversion in patients with SSS ◦ rapid ventricular rates in patients with HCM, AS, WPW Polyuria with the release of ANP as episodes of AF begin or terminate. Tachycardia-mediated cardiomyopathy Pharmacological and non pharmacological Treatment Drugs and ablation are effective for both rate and rhythm control Ryhtm control vs Rate control For rhythm control, drugs are typically the first choice and LA ablation is a second-line choice ( symptomatic lone AF young pts , no structrual HD) RF ablation for WPW, AVRT, Atrial Flutter RF ablation in association with cardiac surgery face a unique opportunity during MV Replacement, LAA obliteration Standalone Surgical procedure (maze III or LA ablation) Circumferential Pulmonary-Vein Ablation RF Pulmonary Vein Isolation Oral, H. et al. N Engl J Med 2006;354:934-941 Pharmacological and NonPharmacological Treatment “Ablate and pace” strategy that often yields remarkable symptomatic relief ( the negative effect of long-term RV) BIV Pacing Atrial pacing, either in RA alone or Biatrial to prevent recurrent paroxysmal AF in pts with Bradycardic indication for Pacing (SSS AAI vs VVI) Atrial pacing IS Not a primary therapy for prevention of AF Atrial defibrillators for patients with LV dysfunction who are candidates for implantable ventricular defibrillators Mortality and Morbidity with AF Death AF Increases Mortality with AMI AF Increases mortality 50% Men 90% Women Highest death 1st yr after AF diagnosis Stroke Risk 35% 1.5% at age 50-59 y 23.5% at age 80-89 AF+HF+CAD increase risk of a stroke 2 fold Risk of Stroke CHADS2 Risk Criteria Score ◦ ◦ ◦ ◦ ◦ Prior stroke or TIA Age 75 y Hypertension Diabetes mellitus Heart failure 2 1 1 1 I aspirin (325 mg) associated with 44% stroke rate reduction Warfarin 50% more effective than aspirin for prevention of ischemic stroke Thank you السالم عليكم AF in Patient with CHF and CRT General schema representing AF mechanisms Predictors of AF HTN and DM were significant independent predictors of AF increasing the risk 1.5 fold. (Framingham Study) HTN is responsible for more AF (14%) than any other risk factor Predictors of AF Independent ECHO predictors of AF : ◦ LA enlargement, ◦ LV fractional short. ◦ LV wall thickness ( 5mm ( 5% ( 4mm AF 39%) AF 34%) AF 24%) ECG evidence of: ◦ LVH was also a powerful age adjusted predictor Mortality results Cumulative mortality (%) Rhythm control Rate control 25 20 15 10 5 0 Year 1 Year 2 Year 3 Year 4 Year 5 N Engl J Med 2002;347:1825-33.