Tips & Tricks: Scrotal disease
advertisement

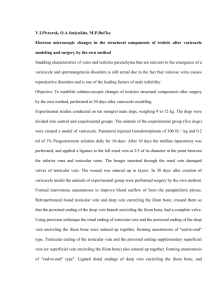
Tips & Tricks: Scrotal disease - Varicocele Woo, Seung Hyo Dept. of Urology, Eulji university College of Medicine, Daejeon, Korea Introduction • First description by Celsus – “… veins that are swollen and twisted over testicle, which becomes smaller that fellow ….” • Prevalence – Adolescent: 15% – P° (35-50%) / S° (69-81%) : progressive Need early intervention ! Introduction (Cont’) • WHO : Varicocele is ass with • Decreased testicular volume • Impaired sperm quality • Decline in Leydig cell function • Several studies results – 70% of healthy palpable varicocele men • Abnormal S/A – Progressive & duration dependent testicular damage – Randomized, controlled, cross-over study • Varicocelectomy significantly improved pregnancy rates Anatomy • Artery – Internal spermatic a. : gonadal artery – External spermatic a. : cremasteric a. – Vasal artery • Vein – Internal spermatic (gonadal) v. : one in 60% – External spermatic vein – Gubernacular vein • Lymphatics – 3.6 in spermatic cord Three compartments Vas & vasal vs. Pampiniform plexus External spermatic vessels Pathophysiology 1. Hyperthermia 2. Reflux of metabolites 3. ‘Hot Rock’ theory 37℃ 33~34 ℃ • Formula – Vol ∝ r2 , R ∝ 1/r4 , Vel ∝ 1/r2 Venous diameter ↑ Venous wall thickening Venous volume ↑ ↓ Resistance & velocity Testicular temperature ↑ Wash out phenomenon (dilution of intratesticular testosterone) Impaired countercurrent heat exchange Impaired spermatogenesis Alteration of germ cell metabolism and function, induce arteriovenous shunting, decreasing activity of enzymes of DNA synthesis, increase apoptosis, induce hypoxia Prognostic indication • (+) predictive value – Grade III – Normal FSH – Lack of testicular atrophy – Motility > 60% – (+) GnRH stimulation test – Total motile sperm > 5 x 106 • Indication for surgery – Ipsilateral growth arrest/atrophy Absolute – Multiple etiology of testicular dysfunction – Abnormal S/A – Bilaterality – Grade III – Soft ipsilateral testis – Pain – Abnormal GnRH stimulation test – Patient/parent anxiety – Abnormal scrotal appearance Minor VARICOCELECTOMY Retroperitoneal Inguinal Subinguinal Management : ‘Palomo’ • Palomo technique – Ligation of gonadal vessels • Modified Palomo technique – Ligation of gonaldal vein • Complication – Recurrence: 11-15% – Hydrocele: 7% – 국내 보고 • Hydrocele: 5-9% • Recurrence: 5-14% Laparoscopic varicocelectomy Management : ‘Ivanissevich’ • • • • • Inguinal approach Familiar region Ease to approach to cord Recurrence rate: 9-16% (국내: 5-15%) Hydrocele: 3-39% (국내: 0-7%) Management : ‘embolization’ • Recently popularized method – Not need an anesthesia – Less invasive – Failure rate: 27% – Recurrence: 4-11% – Hydrocele: 0% Cayan S, et al. J Androl 2009 Management : ‘microsurgical’ • Best way of varicocele management – Inguinal Vs. Subinguinal – Recurrence: <1% (inguinal: 1-2%) – Hydrocele: nearly 0% • 1994, Marmar & Kim – Subinguinal approach • • • • Less morbidity (reserve fascia & muscle) Short recovery time Less post-op pain More complex Surgical technique Comparison of different techniques used for varicocele repair technique Artery preserved Serious Hydrocele Failure (%) morbidity (%) potential Radiographic occlusion Retroperitoneal Yes 0 4-11 Yes No 7 15-25 No Laparoscopic Yes 12 5-15 Yes Conventional inguinal No 3-30 5-15 No Microscopic inguinal Yes 0 1 No Tips-1 • Incision length – Width of testis – 2~3cm • Incision site – Inguinal – Subinguinal Tips-2 • Ligation of external spermatic vein & gubernacular veins Tips-3 • Division into two compartments – Pampiniform & vasal compartment – Zini et al. • Rt : 22 min ↓ • Lt : 6 min ↓ Zini et al. Urology 2006 Tips-4 Identification of arterial pulse 1. Using micro probe 2. Dripping papaverine 3. Shift downward : ext. ring prepubic Tips-4 (cont’) 4. Identification of pulse by anatomy Above all, ligate bridge vessels Then, dissect large veins vertically Don’t ligate large vein till isolation of artery if possible Tips-4 (cont’) 4. Identification of pulse by anatomy Above all, ligate bridge vessels Then, dissect large veins vertically Don’t ligate large vein till isolation of artery if possible Tips-5 • Prevention to risk of hydrocele 1. Save lymphatics 2. Prophylactic hydrocelectomy (plication) • Not saved lymphatics • Not identified lymphatics Conclusions • Unique purpose of varicocelectomy – Optimization of testicular environment – Improvement of spermatogenesis • Selection of technique – Higher success rate – Lower complication – Less invasive “Microsurgery” Conclusions (cont’) • Considerations in Microscopic varicocelectomy – Completely understanding of anatomy – The Site of Incision – Identification of Arterial Pulse • Alter the site of incision • Using papaverine or micro probe • Disconnecting crossing-vessel at first – Prevention of Hydrocele 경청해 주셔서 감사합니다 !