File
advertisement

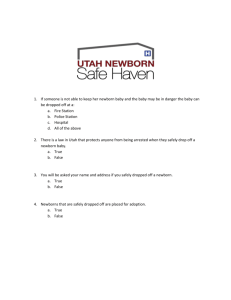
Growth and Development: The Newborn Baby 1 Fetal Circulation: Circulatory Pathways Placenta: 1. 2. 3. The organ responsible for Delivery of nutrients Removal of waste products Delivery of oxygenated blood to the fetus. 2 Circulatory Pathways: Fetal lungs: Are filled with fetal lung liquid not used to oxygenate blood. Because the alveoli are filled with liquid most of the arteries and arterioles are surrounded by liquid which increases resistance to blood flow through the vessel. This results in most of the blood flow bypassing the lungs and therefore directed to the systemic periphery. 3 Circulatory Pathways: Umbilical vein & Ductus Venosus: A vessel which delivers oxygenated blood from the placenta to the fetus. The umbilical vein enters portal venous system where it empties most of the blood flow into the ductus venosus which connects to the inferior vena cava. Average oxygen saturation of blood is 80% in the umbilical vein before it mixes with unoxygenated blood in the ductus venosus. After mixing, the oxygen saturation is approximately 67%. 4 Circulatory Pathways: Foramen ovale: The majority of inferior vena cava blood flow crosses the foramen ovale and into the left atrium bypassing the lungs, some blood flow enters the right ventricle. The foramen ovale is anatomical opening between the right atrium and left atrium which closes shortly after birth. 5 Circulatory Pathways: Ductus arteriosus: A vessel that connects the main pulmonary artery to the aorta. 6 Circulatory Pathways: The blood flow that does enter the right atrium (mainly from the superior vena cava) enters the right ventricle and then the main pulmonary artery where the blood flow then enters the ductus arteriosus which connects to the aorta. Once again, most blood flow bypasses the lungs and is directed to the systemic circulation. Blood flow is flowing in a right to left direction. The ductus arteriosus should functionally close within 15 hours and structurally within a few weeks (in mature infants). 7 Circulatory Pathways: Umbilical arteries: 2 vessels that allows unoxygenated blood to flow from the descending aorta back to the placenta. 8 9 Changes at Birth The First Breath: The lungs are filled with air instead of fluid. Higher oxygen levels in the blood and alveoli filled with air instead of fluid allows for vascular resistance to decrease. This results in a greater increase in pulmonary blood flow. 10 Changes at Birth Anatomical Changes: Placenta is removed from circulation. Higher pressure in the left atrium due to increased pulmonary blood flow cause the foraman ovale to close. Higher concentrations of oxygen in the blood, decreased prostaglandin levels and decreased pulmonary vascular resistance closes the ductus arteriosus. When the umbilical cord is clamped, the umbilical vein closes, systemic vascular resistance is increased and this causes the ductus venosus to close. 11 Figure 28.13 12 Physiologic adjustment to extrauterine life: First period of reactivity: Resting period: lasts for ½ hour, baby is alert & exhibit exploring searching activities, making sucking sounds, rapid H.R & R.R. lasts 90 minutes, baby generally sleeps, slower H.R & R.R. Second period of reactivity: between 2-6 hours of life. Baby is a wake, gagging and choking on mucus. Gain alert & responsive and interest to surrounding. 13 Assessment of well being: Apgar Scoring Is an assessment scale applied at 1 minute and 5 minutes after birth. Give a score (0,1, or 2) for each sign. It serves as a baseline for future evaluation. 14 InRev1 The Apgar Scale Score Characteristic Heart rate 0 Absent 1 2 Less than 100 beats per More that 100 beats minute per minute Efforts to breathe Absent Slow, irregular Good; baby is crying Muscle tone Flaccid,limp Weak, inactive Strong, active motion Skin color Body pale or blue Body pink, extremities blue Body and extremities pink Frown, grimace Vigorous crying, coughing, sneezing Reflex irritability No response 15 Apgar score A score under 4 is in serious danger and need resuscitation. A score of 4-6 may need clearing of the airway and O2 supplement. A score of 7-10 is good 16 The Newborn Baby Weight: differs depending on the race, nutritional, intrauterine and genetic factors. Normal rates 2.74.0 kg. Newborn loses 5-10% of birth weight during the 1st few days because of: No longer under the influence of salt & fluidretaining maternal hormones. Diuresis: to remove part of body fluids. Limited by low caloric content of colostrum. Time needed to establish sucking. Stools. 17 The Newborn Baby Recaptures birth wt within 10 days. Head-to-heel length: birth length is 48 – 53 cm. H.C: 33-35 cm. C.C: 2 cm less than H.C. 18 Classification of infants based on gestational ages and birth weights Preterm or premature: infant born before the end of 37 weeks, regardless of weight Term or full term: born between 38 & 42 weeks, regardless of weight Postterm: an infant born after 42 weeks regardless of weight Low birth weight: any infant at birth who weighs less than 2500 gm 19 Small for gestational age (SGA): any newborn whose weight is below the 10th percentile, This means that they are smaller than 90 percent of all other babies of the same gestational age (according to intrauterine growth curve) regardless of gestation Appropriate for gestation age (AGA): any newborn whose intrauterine growth has been normal (according to intrauterine growth curve) for that length of gestation Large for gestational age (LGA): any infant born whose weight is above the 90th percentile regardless of gestation Intrauterine growth restriction (IUGR): failure of fetus to grow as expected during gestation 20 21 Appearance of newborn Flexion posture. Looks , red or cyanotic. Body covered with varying amount of lanugo and vernix caseosa. 22 Vital signs Temp: 37.2 at birth fall because of heat loss, little s.c fat & immature tep. Regulating center (drying, wrapping, & put them under the radiant heat + kangaroo care). Pulse: 120-160 bpm. ↑ at the moment of birth to 180 bpm. 1 hour after birth ↓ to 120-140 bpm. 23 Vital signs Respiration: first few minutes 80 b/m↓ to 30-60 b/m when newborn at rest. Usually irregular with short periods of apnea Blood pressure: 80/60 mm/Hg ↑ at 10th day to 100/50 mm/Hg. 24 Head Large head, overridden sutures. Head molded to fit cervix. Caput succedaneum: Edema of the soft scalp tissue at the presenting part of the head. Accumulation of serum in the tissues above the bone Cross suture lines Disapear in few days Cephalhematoma: Localized collection of blood between the skull bone and its periosteum May involve one or both parietal bones Weeks to resolve Dose not cross sutures 25 26 Caput Succedaneum Cephalohematoma 27 Caput succedaneum 28 cephalheamatoma 29 30 Molding of infant’s head 31 Fontanelles 6 fontanelles. Anterior fontanelle, diamond shaped, 2.54 cm, will closes at 12-18 mon. Posterior fontanelle, triangular, 0.5-1.0 cm, closed at 2 mon. Pair of anteriolateral fontanelle close at 3 mon. Pair of posteriolateral fontanelle close at 12 mon. 32 Eyes: tearless cry (lacrimal ducts mature at 3 months) permanent eye color between 3-12 mon. Ears: pinna tends to bend easily. Nose: large for face. Mouth: prominent, large, & short tongue. Natal teeth are unusual. Thrush indicates candida infection. Neck: short & chubby with many folds. Head lags 33 Skeletal system Arms are slightly longer than legs. Hands clenched into fists. 3 normal creases. Flat sole of the feet Hips inspect for symmetry—skin folds should match ortolani maneuver for hip dysplasia Check for tufting of hair at base of spine (spina bifida, occulta) Clubfoot Absence of limb or digit 34 35 Skin Vernix casoesa Acrocyanosis Lanugo Bruising, petechiae from birthing Mongolian spots— generally back and buttocks Milia 36 Milia Small, whitishyellow papules found close to the skin surface Particularly common around eyes and midface 37 Skin Down syndrome— simian crease on palm Strawberry mark— nevous Vasculosus— hemangioma Erythema toxicumnewborn rash 38 Strawberry mark—nevous Vasculosus—hemangioma Vasculosus—hemangioma Erythema toxicum 39 Appearance of newborn Chest: looks small (compared to head), engorged breasts (maternal hormone). Ronchi because of mucus. Abdomen: protuberant. Bowel sound should be present within an hour. Umbilical cord white gelatinous structure with red & blue streaks for the 1st hour. Begin to dry breaks free by 6th10th day. Check for concave abdomen 40 Circulatory & hemopoietic Resting hr 100-160 Hr above 160 or below 100 should be reevaluated Blood volume: 80-85 ml/kg, average about 300 ml but can have an additional 100 ml if cord is not cut in reasonable length of time Fetus needs additional blood cells for O2 exchange Hgb 14-24 g/dl Infant Hgb F – higher O2 affinity Hgb A production largely replaces Hgb F by 4 months Iron stores good for 5 months Blood coagulation: born with long coagulation time (lower level of vit. K). 41 GI SYSTEM Baby learns to coordinate breathing, sucking and swallowing Bacteria not present in gut vitamin k Digestion-simple CHO and protein. (Starches and fats are not easily digested at this time) Feeding varies—cues hand to mouth movement and sucking fingers intensify when hungry Prevent regurgitation by not overfeeding, frequent burping and positioning the head slightly elevated 42 GI 2 Stool—meconium—greenish black Stools change and the stooling pattern change indicates good bowel functioning Color time and character of first stool should be documented. Diarrhea stool—loss of fluid quickly 43 Immune system Passive immunity from mom Immunoglobulins gradually develop High risk of infection in first few month—abnormal discharges or rashes should be evaluated 44 Renal system Should void in first 24 hour Frequency depends on intake Not able to concentrate urine May see blood in diaper of female Hypospadias Extrophy of bladder 45 Hepatic system Iron storage Conjugation of bilirubin—function not well developed at birth— Physiologic jaundice—after 24 hours— preterm increase and more severe Pathologic jaundice—before 24 hours Kernicterus—billiruben higher than 25 Breastfeeding—may occur up to 2 weeks pp 46 Anogenital Patent anus (check for imperforate anus). Meconium within 24 hour. Male genitalia: edematous scrotum, check for undescended testicles, epi or hypospadias. Female genitalia: swollen vulva (maternal hormones), pseudomenstruation. 47 Neuromuscular system The newborn is born with certain specific responses that are triggered by specific stimuli. Some of these reflexes, such as rooting and sucking, appear to have survival implications. Other reflexes appear to be precursors for later voluntary motor behavior. The newborn’s reflexes may also give information about the health of the child’s nervous system. 48 Sucking Onset: ~28weeks GA Well-established: 32-34 weeks GA Disappears: starting around 12 months Elicited by the examiner stroking the lips of the infant. 49 Rooting This reflex begins when the corner of the baby's mouth is stroked or touched. The baby will turn his/her head and open his/her mouth to follow and "root" in the direction of the stroking. This helps the baby find the breast or bottle to begin feeding. 50 Moro Reflex The Moro reflex is often called a startle reflex because it usually occurs when a baby is startled by a loud sound or movement. In response to the sound, the baby throws back his/her head, extends out the arms & legs, with fingers extended in “c” shape, cries, then pulls the arms and legs back in. lasts about five to six months. 51 Grasp reflex Stroking the palm of a baby's hand causes the baby to close his/her fingers in a grasp. The grasp reflex lasts only a couple of months and is stronger in premature babies. 52 Tonic Neck Reflex When a baby's head is turned to one side, the arm on that side stretches out and the opposite arm bends up at the elbow. lasts about six to seven months. 53 Babinski reflex When the sole of the foot is firmly stroked, the big toe bends back toward the top of the foot and the other toes fan out. This is a normal reflex up to about 2 years of age. 54 Step reflex This reflex is also called the walking or dance reflex because a baby appears to take steps or dance when held upright with his/her feet touching a solid surface. 55 Senses Hearing: able to hear in utero, within days after birth hearing become acute. Vision: see as soon as they are born (blinking reflex). Can’t follow objects past the midline. Best focus on black & white. Newborns see best using peripheral vision, out of the corner of their eyes, and when objects are about 9-12 in. (22.86-30.48 cm) away. 56 Senses Touch: The sense of touch in newborns is well developed, particularly around the mouth. They are sensitive to temperature, pressure, and pain. Smell: well developed, newborns are often able to recognize the smell of their mother within the first few days of life. Taste: prefer sweet tastes and usually do not like sour, bitter, and salty tastes. 57 58 The Newborn’s States Sleeping Newborns sleep an average of 16-18 hours daily. Newborns usually follow a sleep-wake cycle of around 4 hours of sleep followed by 1 hour of wakefulness. By 3 or 4 months newborns usually sleep through the night. 59 The Newborn’s States Crying Basic Cry Mad Cry More intense and louder. Pain Cry Starts softly and builds in volume and intensity. Often seen when the child is hungry. Starts with a loud wail, followed by long pause then gasping. Be calm and patient Do not shake baby Know signs of emergencies 60 61