Anti-infective Drugs
advertisement

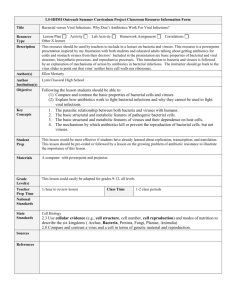
Anti-infective Drugs Jan Bazner-Chandler MSN, CNS, RN, CPNP Bacteria Bacteria Gram-positive bacterium has a thick layer of peptioglycan. Gram-negative bacterium has a thin peptioglycan layer and an outer membrane. Common Bacterial Pathogens Gram positive Staphylococcus aureus Streptocci Enterococci Gram negative Escherichia coli or E-coli Klebsiella Proteus Pseudomonas Empiric Therapy Administration of antibiotics based on the practitioner’s judgment of the pathogens most likely to be causing the infection; it involves the presumptive treatment of an infection to avoid treatment delay before specific cuture information has been obtained. Prophylactic Antibiotic Therapy Antibiotics taken before anticipated exposure to an infectious organism in an effort to prevent the development of infection. IV antibiotics given prior to surgery Superinfection An infection occurring during antimicrobial treatment for another infection, resulting from overgrowth of an organism not susceptible to the antibiotic used. A secondary infection that occurs due weakening of the patients immune system by the first infection. Examples of Superinfections Fungal or yeast infection Diarrhea due to diminished normal flora of the gastrointestinal tract. Laboratory Tests Gram stain – microscopic identification of organism Culture – identifies causative agent and susceptibility to specific antibiotics Serology – titers or antibodies measured CBC – looking at WBC Cultures Throat Wound Urine Sputum Blood Clinical Pearl Always collect culture: urine, sputum, wound drainage, or blood prior to starting antibiotic therapy. If technician is drawing blood make sure it has been done before starting antibiotics. Antimicrobials Drugs used to prevent or treat infection caused by pathogens Two Classifications Bactericidal drugs kill bacteria directly. Bacteriostatic drugs prevent bacteria from dividing or inhibits their growth. Two Types of Bacteria Aerobic – grow and live in presence of oxygen Staph & Strep Anaerobic – cannot grow in presence of oxygen Deep wounds Characterized by abscess formation, foul-smelling pus and tissue destruction Community-Acquired Infection Less severe and easier to treat, although drug resistant strains are increasing Remember Staph is everywhere – it is normal flora on skin and in the upper respiratory tract MRSA: methicillin-resistant-Staphylococcus aureus Nosocomial Infections More severe and difficult to manage because they often result from drug-resistant microorganisms and occur in clients whose resistance is impaired Pseudomonas Proteus Bacterial Resistance Bacteria develop the ability to produce substances which block the action of antibiotics or change their target or ability to penetrate the cells. What causes resistance? Widespread use of antimicrobial drug Interrupted or inadequate antimicrobial treatment of infection Type of bacteria – gram-negative strains have higher rates of resistance Re-occurring infections Condition of the host Location – critical care areas Opportunistic Host Compromised immune system Infants Geriatric population Cancer HIV positive – low T-cell count Burns Skin breakdown Client with total knee or hip replacement Client History / Assessment Allergies Previous drug reactions Baseline renal and liver function Review culture reports for appropriate antibacterial drug choice Patient response to antibiotics therapy Are they getting better? Any side effects? Antibiotics Sulfonamides Penicillins Cephalosporins Macrolides Fluoroquinolones Aminoglycosides Tetracyclines Sulfonamides Action: inhibit the growth of bacteria (bacteriostatic antibiotic) by inhibiting the growth of susceptible bacteria by preventing bacterial synthesis of folic acid. Usually used in combination drugs. Trimethoprim / sulfamethoxazole: Trade name Bactrim, Septra, TMP/SMX Indications Broad spectrum: can be used against gram negative and gram positive organisms Very useful in treating kidney infections since they achieve a high concentration in the kidneys. Susceptible organisms: Enterobacter, E.Coli, Klebsiella, Proteus Problem: organisms becoming more resistant Specific Use of Sulfa Drugs HIV patients with pneumocystis carinii’ May be given Bactrim or Septra prophylactically. Contraindications Drug allergy to sulfa Use of thiazide and loop diuretics Pregnant women Infants younger than 2 months of age Adverse Effects Most common is cutaneous reactions – can occur weeks after therapy started. Erythema multiforme (Stevens Johnson Syndrome) Toxic epidermal necrolysis Photosensitivity reactions: exposure to sunlight can result in severe sunburn B-Lactam Antibiotics Includes 4 major drug classifications penicillins cephalosporins carbapenes monobactams Penicillin Derived from mold fungus Penicillin First generation IM or IV Newer penicillins have been developed that increase gastric acid stability of penicillin Good drug since it enters most bodily fluids: joint, pleural, and pericardial. Not effective against intraocular (eye) or cerebral spinal fluid infection (CSF) Penicillin Bactericidal action against sensitive bacteria Action: binds to bacterial wall, resulting in cell death Susceptible Bacteria Gram-positive organisms Streptococcus Enterococcus Staphylococcus Adverse Reactions Most common reaction is GI (diarrhea) when administered orally. Urticaria (rash), pruritus (itching), and angioedema (swelling of the throat) Severe reaction: Steven’s Johns Syndrome Note: when giving IV or IM observe for ½ to 1 hour after giving for adverse reactions. Hives Anaphylaxis Combination Penicillin / B-lactamases Unasyn Augmentin Timentin Zosyn Ampicillin – Synthetic Penicillin Broad spectrum effective against several gram-positive and gram-negative bacteria E-coli, proteus, Salmonella, Shigella Not effective against staphylococci on gonococci Bronchitis, sinusitis, and otitis media Ampicillin Bactericidal action – spectrum is broader than penicillin Binds to bacterial wall resulting in cell death Nursing Implications Same as penicillin Ask client about oral contraceptive use – drug may cause transient decrease in effectiveness Advise to use additional BC – barrier protection during antibiotic therapy Amoxicillin Trade name: Amoxil, Trimox, Wymox Classification: aminopenicillins Indications: skin infections, otitis media (ear infection), sinusitis, respiratory infections. Inexpensive in generic form but required frequent dosing (q 8 hours) Amoxicillin Oral equivalent of Ampicillin Readily absorbed and reaches therapeutic levels rapidly Drug of choice in prevention of bacterial endocarditis Clients with total knee or hip replacement, heart valve replacement need to take prior to any dental work, endoscopy exams Dosing for Amoxicillin Adults: 250 to 500 mg q8h Infants and children less than 20 kg: 20 – 40 mg / kg / day divided into doses q 8 hours Cephalosporins • • • Widely used drug derived from fungus Used against gram–negative bacteria Widely absorbed and distributed in most bodily fluids – placenta and breast milk Cephalosporin First generation Cephalosporin drugs do not reach therapeutic levels in CSF (cerebral spinal fluid) but 2nd, and 3rd generation drugs do – especially important in treating meningitis. Meningitis First Generation Cephalosporins Bactericidal action – binds to bacterial cell wall, causing cell death Keflex (PO) still used extensively in treatment of skin infections Ancef – often ordered preoperatively Impetigo First Generation Cephalosporins Bactericidal action – binds to bacterial cell wall, causing cell death Keflex (PO) still used extensively in treatment of skin infections Ancef – often ordered preoperatively in clients undergoing orthopedic procedures Keflex First generation cephalosporin Action: binds to bacterial cell wall membrane, causing cell death Therapeutic effect: bactericidal action against susceptible bacteria Active against many gram-positive cocci – step and staph Client teaching May be taken with or without food but food may minimize the GI irritation Distribution: may cross placenta or enter breast milk in low concentrations. Excreted entirely by the kidneys. Keflex Dosing Adults: 250 – 500 mg q 6 hours Children: 25 – 50 mg / kg / day in divided doses q 6 h Cefazolin or Ancef Cefazolin – first generation cephalosporin Well absorbed following IM or IV administration Crosses to placenta and breast milk in small concentrations Minimal CSF penetration Excreted by kidneys Knee or hip replacement Ancef Dosing IV Used for UTI, bone and skin infections, endocarditis Not suitable for treatment of meningitis Perioperative prophylaxis 1 gram within 60 minutes of incision Post operatively every 8 hours for 24 hours (3 doses) Second-Generation Cephalosporins More active against some gram-negative organisms and anaerobic organisms than the first generation drugs. May be effective in infections resistant to other antibiotics Penetration into CSF is poor but adequate to be used in meningitis Action: bactericidal – binds to cell wall Third Generation Cephalosporin Drugs Similar to the second generation but has increased activity against gram-negative pathogens even for drug resistant pathogens. CSF penetration is better than the first two generation cephalosporin drugs. Drug / Drug Allergies If a client is allergic to penicillin there is a 1 to 18% chance they will be allergic to cephalosporin drugs. Carbapenems Has very broad antibacterial action Are often used for complicated body cavity and connective tissue infections in the hospitalized patient. imipenem-cilastatin (Primaxin) meropenen (Merrem): only drug in this class used in the treatment of bacterial meningitis. Macrolides Macrolides first developed in the 1950s with the drug: erythromycin. Four main drugs azithromycin * Zithromax Clarithromcin * Biaxin dirithromycin erythromycin Macrolides Two of the new drugs in the macrolide classification: azithromycin and clarithromycin have longer duration and improved resistance to acid degradation in the stomach. Dosing is less frequent GI effects decreased Better absorption than erythromycin Macrolides Action: work by inhibiting protein synthesis in susceptible bacteria. Contraindications: drug allergy Adverse effect: new drugs have lower GI effects and are used in patients allergic to penicillin / cephalosporin drugs. Ketaloids Only one drug in this drug classification Generic: telithromycin Trade: Ketek Available for oral use only. Better acid stability and antibacterial coverage than macrolides. Tetracyclines Action: binds to divalent (Ca2 + mg2) and Al3 mettalic ions to form insoluble complexes. Why do you need to know this? When given with milk, antacids or iron there is a reduction in oral absorption. Contraindicated in children under 8 years of age because it can result in tooth discoloration. Tetracyclines When used? Syphilis and Lyme disease Antibiotics Used to Treat Serious Infections IM or IV administration Have more toxic side effects Blood levels may need to be monitored to determine therapeutic versus toxic levels of mediation in the blood. Serious Adverse Effects Nephrotoxicity: Toxicity to kidneys, often drug induced and manifesting in compromised kidney function. Ototoxicity: Toxicity to the ears, often druginduced and manifested by varying degrees of hearing loss than is likely to be permanent. Pseudomembranous colitis: a necrotizing, inflammatory bowel condition associated with antibiotic therapy. Aminoglycosides Pharmacologic classification: Bactericidal drugs Therapeutic classification: anti-infective Action: inhibits protein synthesis at the level of the 30s ribosome Work primarily on dosing due to concentration dependent killing of bacteria Concentration Dependent A property of some antibiotics, especially aminoglycosides and vancomycin, of achieving a relatively, high plasma drug concentration, results in the most effective bacterial kill. Blood Plasma Levels Peak levels: refers to amount of drug present in blood plasma within 15 to 30 minutes of IV drug administration 30 to 90 minutes of IM drug administration Trough levels: refers to lowest level of drug present in the blood plasma. Since the drugs can cause severe adverse effects the excretion of the drug needs to be monitored. Blood drawn just before the next dose given. Adverse Effects Aminoglycosides Nephrotoxicity occurs in 5 to 25% and ototoxicity (damage to VIII cranial nerve) occurs in 3 to 14%. Aminoglycosides gentamicin (Garamycin) tobramycin (Nobcin, TOBI) neomycin (Neo-Fradin) used to irrigate bowel before major bowel surgery Topical applied to eye and skin infections Floroquinolones Action: destroys bacteria by altering their DNA. Two most common drugs: ciproflxcin (Cipro) clindamycin (Cleocin) Used in treatment of chronic infections or deep (anaerobic) abdominal infections and MRSA. Major Adverse Side Effect Clindamycin or Cleocin can cause pseudomembranous colitis Signs and symptoms: abdominal pain and diarrhea MRSA Infections MRSA infection is caused by Staphylococcus aureus bacteria — often called "staph." MRSA stands for methicillin-resistant Staphylococcus aureus. It's a strain of staph that's resistant to the broad-spectrum antibiotics commonly used to treat it. MRSA can be fatal. MRSA Vancomycin Action: destroys bacteria by binding to the bacterial cell wall, producing immediate inhibition of cell wall synthesis and death. One of the drugs used in MRSA infections that are resistant to floroquinolones (cleocin). Adverse Effect Red man syndrome has often been associated with rapid infusion of the first dose of the drug and was initially attributed to impurities found in vancomycin preparations. Even after improvement in vancomycin's purity, however, reports of the syndrome persist. Flushing on upper chest, neck and face Intervention: slow the IV infusion rate. Drugs to help with the Flu Tamiflu and Relenza Uses: active against influenza virus types A and B. Shown to reduce the duration of influenza infection by a few days. Anti-viral Drugs Kill or suppress viruses by either destroying virons or inhibiting their ability to replicate. Does not irradicate the virus but helps the immune system to eliminate the virus. Herpes Zoster Herpes simplex virus type 1: cold sore Herpes simplex virus type 2: genital herpes Human herpesvirus type 3: chicken pox or shingles Human herpesvirus type 4: Espstein Barr Virus Human herpesvirus type 5: CMV or cytomegalovirus Cold Sore Herpes Zoster - Shingles Herpes Drugs Generic: acyclovir Trade: Zovirax Action: interferes with DNA synthesis. Therapeutic effects: Inhibition of viral replication, decreased viral shedding and reduced time for healing of lesions. acyclovir Comes in topical, po and IV preparations Should be started within 24 hours of outbreak.