Process Recording Guidelines
Process Recording: A Process recording is a tool to help the student analyze their interpersonal interactions with assigned clients. Through a
retrospective, reflective process of recreating verbatim interchange between the student and the client making inferences regarding the meaning of the client’s
behavior, noticing patterns of the student’s own behavior and offering alternative approaches, the student will learn more effective communication strategies to
use in a variety of situations.
Purpose: The purpose of a process recording is to improve care and interaction with competency in the collection, interpretation, and synthesis of raw data
obtained. This recording assists the student develop a plan, intervene, and evaluate nursing actions based on client outcomes.
Students develop the ability to identify their own thoughts and feelings in relation to self and others, and better understand how their own behavior and the
client’s behavior impact upon each other. Students learn to identify the client’s unmeet needs, and core problems which are influenced by the client’s actions
and thoughts. Students may then alter or modify their nursing approaches based on insights into the client’s needs, feelings and or difficulties.
Nursing faculty use process recordings to assist students to develop skills in observing, communicating, and apply theories and concepts to the nurse/client
interactions. Faculty will provide feedback to students through written comments. Feedback is an important tool that can guide students to question, explore
and develop skills, without faculty being present during the therapeutic interaction. Students are encouraged to view comments as constructive feedback rather
than criticism.
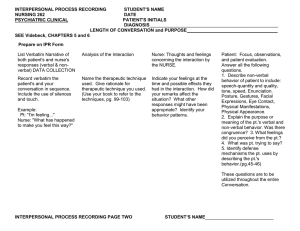
Format for Process Recording:
Interaction data: Client’s behavior, verbal and non-verbal, Nurse’s behavior, verbal and non-verbal.
Interpretation: Use psychosocial theories to explain the meaning of the client’s behavior, communication, developmental and adaptations, anxiety or
defenses.
Identify unmet needs, student’s response or approach to the interventions used, your own feelings or thoughts, and any theoretical basis for interventions used.
Evaluation: Were the desired outcomes achieved? What changes you might make, or how you would do things differently.
Requirements: Each process recording will consist of one background data sheet, including information about where and how the interview took place, or
what influenced the interaction, and the interaction data sheets. Students are to use the template provided via Blackboard and type the content, and submit it
via email by the due date.
1. Collection of data: In column #1 the student shall record verbal and non-verbal communications of both the nurse and the client. Record this as
accurately as possible. Data is precisely what you and the client state. It is not an expression or opinion about the behavior that transpired.
2. Interpretation of Data: In column #2 write your interpretation of the client’s behavior. This recording should include psychosocial theories of references
from your text to explain the meaning of the behaviors exhibited, or the defense mechanism displayed. The developmental status and personality of the client
may be explained here. You are expected to use theory in this column, with appropriate citations.
3. Analysis of Nursing Approaches: In column #3 you should state the rationale for your responses to the client. This should include rationale for
your questions and statements, but also incorporate self-critique. You should reflect whether your own statements were therapeutic, and evaluate your feelings
of how your behavior influenced your behavior.
4. Evaluation: Column #4 should include how you would have intervened differently based on your new understanding of the client interaction. Would you
have asked different questions, or made a different statement. Evaluate whether outcomes were achieved, and how you plan to intervene with this client in the
future.
NUR 202
Client initials: KM
Process Recording
Date: July 17, 2014
Name: Amanda Twining
DATA COLLECTION
DATA INTERPRETATION
RATIONALE/ANALYSIS
SYNTHESIS/EVALUATION
Nurse/Client interactions, including
verbal and non-verbal
Analysis of the client behavior,
examples: behaviors, defense
mechanisms
Nurse’s self-critique: why you
said what you said. Evaluation
of your own feelings
Were outcomes achieved? What would you
do differently if you had to do this interaction
again? What did you learn about how you
communicate? What did you learn about
how the client communicates?
I conducted this conversation for the
purpose of gathering information for Project
3, which was successful. However, in the
future, I would move the conversation to a
quieter location, because it was obvious the
client was getting nervous.
Me: Hi! Is it okay if I sit down and talk with
you for a couple minutes?
Client: Yeah, I guess.
He is sitting at a table in the dining room;
he goes between looking around and
holding his head in his hands. I take a seat
to his left. My head rests on my left hand.
Me: How are you feeling today?
Client: I’m okay. They’ve got me on so
many meds I can’t keep ‘em straight.
Me: Do you think the meds are helping?
Client: They help. I feel okay right now in
here. Once I’m out, I’m afraid of how I’ll
act. You know, I’m schizophrenic, and I’m
what they call “antisocial”.
He folds his arms.
Therapeutic: Offering self, giving
recognition.
I was pleased he was willing to try
to talk with me.
Motor agitation
Paranoia
His speech became pressured at
this point, and he spoke very
rapidly. He wasn’t looking at me.
Silence
Folding his arms indicated to me
that he was getting defensive.
I can’t take being around people. I’m a
threat to other people.
Me: Do people make you anxious?
Therapeutic: Attempting to
translate into feelings.
I wish I had made this into a
statement.
My voice remains calm.
Mental Health Worker: [Client], your lunch
is ready.
Client: I can’t do this right now. Can we
finish this later? I can’t do this. I gotta go.
You gotta go.
Therapeutic: Giving broad
opening.
I allowed the client to steer the
conversation.
Therapeutic: Reflecting
Inability to maintain
attention/Paranoia
I get up from the table. The mental health
worker sets the tray on the table.
Me: That’s okay. Enjoy your lunch.
Client: Yeah.
Not sure if this was therapeutic or
not. It was clear he did not want
to speak with me anymore, and I
did not want to make him
uncomfortable.
I learned that I don’t speak much in
conversation, and I could use more practice
in directing conversations.
This client is agreeable in the beginning of
conversations, and becomes more agitated
the longer the conversation continues.
Small chunks of communication would be
beneficial for this client.
 0
0