Chapter 11 Intervention strategies aimed at groups and

Chapter 11
Intervention strategies aimed at groups and individuals
‘Talking the talk and walking the walk’
‘The drama of behaviour change and resistance to it plays itself out across the full spectrum of daily life.’
(Rollnick, Mason and Butler 1999).
Chapter 11 objectives
• provide a framework for discussing interventions aimed at increasing physical activity levels
• summarise recent reviews that cover individual and group approaches
• give examples of studies that have used a group setting to promote physical activity
• give examples of studies that have used individuals as the focus for promoting physical activity
• discuss the use of pedometers as a tool to promote physical activity
• describe the process of physical activity counselling and show results of studies using this approach
• show how the primary care setting can be used to increase physical activity
• discuss limitations to the evidence base regarding groups and individuals
• draw conclusions about current research knowledge in this area
• make recommendations for researchers and practitioners.
Table 11.1 Summary of evidence from
‘review of reviews’ (Hillsdon et al.
2003)
• In healthcare settings:
• Brief advice from a healthcare professional can lead to modest short-term
(less than 12 weeks) increases in PA
• Referral to an exercise specialist can lead to longer term change (up to 8 months)
• Walking is the most frequent mode of
PA recommended
Table 11.1 Summary of evidence from
‘review of reviews’ (Hillsdon et al.
2003)
• In community settings:
• Short and medium term change in PA feasible
• Interventions based on behaviour change theory best
• Moderate intensity (walking) and nonfacility based interventions are best
• Contact with an exercise specialist can help sustain change
Table 11.1 Summary of evidence from
‘review of reviews’ (Hillsdon et al.
2003)
• Workplace settings
– No consistent evidence
•
•
• Gaps in the evidence:
Black and ethnic minority groups
– No evidence available
Policy interventions
– No evidence available
• Changing the built environment
– No evidence available
Systematic reviews
• a systematic review tries to capture all that is known in the literature on a particular topic and judge it according to specified criteria
• reviewers search all possible data bases
• In the UK the Cochrane reviews are a good source of what systematic reviews do..check out http://www.cochrane.org/
Systematic reviews- continued
• A recent systematic review of interventions to promote physical activity was conducted in the US by
Kahn et al (2002) [American Journal of
Preventive Medicine, 22(4), 73-108.]
• Evidence is rated as ‘strong’, ‘sufficient’ or ‘insufficient’
Evidence from the Kahn et al systematic review
• There was strong evidence that personalised health behaviour-change programmes tailored to an individuals specific stage of behaviour or interest were effective in increasing physical activity.
• There was strong evidence that improved access to opportunities and active environments
(e.g. walking or biking trails, local activities in local centres and workplaces, educational counselling, risk screening and workshops), along with educational activities which connected to these opportunities, increased physical activity.
Evidence from the Kahn et al systematic review
• There was strong evidence that the use of large scale, high visibility, multi-strand community wide campaigns that used a range of methods was effective in increasing physical activity.
• There was strong evidence that strengthening local support networks through buddy systems, walking groups and exercise contacts increased physical activity .
• There was insufficient evidence that familybased social support interventions effectively increased physical activity .
– Why do you think this may not work?
Steps (1-3) in a typical physical activity counselling session
• Step 1 Determine physical activity history
– Discuss the reasons that the person has for wanting to increase activity. Take note of when the person was last active, the kinds of activities they might like now and a measure of recent physical activity, e.g. 7 day recall.
• Step 2 Discuss decision balance
– Ask the person to consider what the ‘pros’ and ‘cons’ of increasing activity are for them. If there are more cons than pros ask them to consider how to minimize some of the cons.
• Step 3 Ensure social support
– Determine with the person what kind of support they might need and who can provide it.
Steps (4-6) in a typical physical activity counselling session
• Step 4 Negotiate Goals
– Help the person set realistic and time phased goals for gradually increasing activity up to a level they have determined, e.g. in 4 weeks time I would like to be walking for 30 minutes more on at least 3 days of the week. Write these goals down.
• Step 5 Discuss relapse prevention
– If there is time or if the counselling session is with someone who is already active then discussion on how to prevent relapse from regular activity should take place.
• Step 6 Provide information on local opportunities
– All information on relevant local activities, such as walking paths, swimming pools and classes should be on hand to supplement discussion as required.
Advantages and disadvantages of different
PHC schemes for promoting physical activity
Practice-Managed Schemes
Advantages
• counselling can be made available on site
• available to larger percentage patients
• physical activity can be delivered within a 'healthy lifestyle' message
• greater flexibility for patients who can be directed to a choice of several outlets in the community
• better opportunities for record-keeping
Disadvantages
• facilities not often available on site
• finding trained personnel may be difficult
• may not provide sufficient motivational boost to get patients started
• difficult to provide support with patients left too much on their own
• difficult to create social atmosphere unless exercise class takes place on site
• the scheme may be perceived as medical rather than intrinsically worthwhile and enjoyable
Advantages and disadvantages of different
PHC schemes for promoting physical activity
Leisure Centre Managed
Advantages
• eases the burden of the GP
• no costs for PHC
• facilities readily available on site
• trained personnel are usually available
• motivation and support for the patient can be high
• social benefits for the patient can be high
Disadvantages
• sporty image has to be overcome in order to attract patients
• physical activity is restricted to discrete exercise sessions rather than lifestyle change
• facilities are often only available during slack day-time hours
• scheme often has an end-point with limited follow-up
• doctors may not be willing to refer patients
• currently schemes attract a very small percentage of patients
• some schemes could not cope with large numbers of patients
Examples of incremental goals
• GOALS SET IN MINUTES
• GOALS SET IN STEP
• Week 1 Aim : To
COUNTS accumulate an extra 15 • Week 1 Aim : To increase minutes of walking on at baseline step count by least 3 days of the week.
• Weeks 2 and 3 add days
1500 steps on at least 3 and minutes incrementally days of the week.
• Week 4 Aim : To add from
• Weeks 2 and 3 add days baseline an accumulated and steps incrementally
30 minutes of walking on • Week 4 Aim : To increase most days of the week by 3,000 steps per day from baseline most days of week
USE RE-AIM PRINCIPLES TO HELP PLAN,
EVALUATE, AND REPORT STUDIES
R
E
A
I
M
Increase
Increase
Increase
Increase
Increase
Reach
Effectiveness
Adoption
Implementation
Maintenance
Glasgow, et al. Ann Behav Med 2004;27(1):3-12 see also www.re-aim.org
Key point:
• Systematic reviews suggest that shortterm changes in physical activity are achievable but that long-term change is difficult to achieve.
Key point:
• ‘Project Active’ was the first study to show that promoting active living had similar fitness effects to promoting more traditional structured exercise.
Key point:
• Families have the potential to influence activity levels of all generations but there is currently limited evidence about the effectiveness of interventions that target families.
Key point:
• A large percentage of university students do not achieve minimum levels of physical activity but students are more likely to be active if they had attended PE classes in their final years of schooling.
Key point:
• Pedometers are cheap and accurate tools for measuring step counts but can they motivate people to walk more?
Key point:
• Motivational interviewing is a counselling style that holds much promise for changing physical activity levels.
Key point:
• Physical activity counselling/consultation offers a method of helping individuals change their physical activity levels
• Counsellors must develop appropriate counselling skills as well as knowledge about physical activity.
Key point:
• The primary care setting offers the opportunity to counsel people who are not achieving the minimum levels of physical activity and help them become more active.
Key point:
• Current evidence suggests that the most effective way of increasing physical activity in the primary care setting has not yet been developed.
Key point:
• GPs and other members of the primary care team should receive appropriate training in physical activity counselling.
Key point:
• The RE-AIM principles offer a public health perspective on how to evaluate interventions.
11.1 Changes in maximum oxygen uptake in both lifestyle and structured groups in Project Active
31
30
29
28 ml/kg/min
27
26
25
24
0 6 12 months
18 24
Lifestyle
Structured
11.2 Changes in total energy expenditure in both lifestyle and structured groups in Project Active
35
34.5
34
33.5
Lifestyle
Structured
32.5
32
0 6 12 months
18 24
11.3 Study design for a postal intervention targeted at precontemplating and contemplating students (Woods, Mutrie, Scott 2002) baseline questionnaire completed at matriculation
(n=2943, first year intake) followed up at 7 and 19 months stage matched for precontemplators and contemplators
(n = 459) experimental
(n= 229) stage matched materials sent at 2 & 4 months control
(n=230)
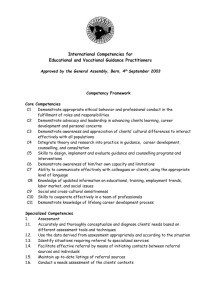
Stage of Change and Physical Education
35
30
25
20
15
10
5
0
50
45
40
PE
No PE
PC C P A M
Those who had participated in PE during their final two years in school were more likely to be in active categories of SOC (PE c
2 (4,
N = 2853) = 79.86, p < .001) and to intend to exercise in the future
(PE c
2 (4, N =2857) =93.58, p < .001) (Woods, Mutrie, Scott 2002)
11.5: Mean step-count comparison for each group at all time-points
Baker, G., Lowry, R., & Mutrie, N. (2008). International Journal of
Health Promotion and Education, 46 (1).
100000
95000
90000
85000
80000
75000
70000
65000
60000
Original pedometer group
Original control group
0 4 8 12 16 20 24 28 32 36 40 44 48 52
Time (w eeks)
11.6. Design for community trial of exercise consultation versus fitness assessment
(Lowther, Mutrie and Scott 1999)
Respondents to invitation to project ( n=370) measures taken at baseline, 4 weeks, 3, 6 & 12 months
Fitness assessment
(n=225) experimental
(n=112) control
(n=113)
Exercise consultation
(n=145) experimental
(n=73) control
(n=72)
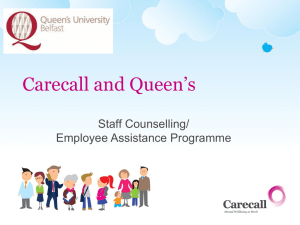
11.7. Percentage of the participants who opted for exercise consultation by physical activity status
Regularly active Not regularly active
53% 47%
FITNESS
ASSESSMENT
Regularly active Not regularly active
40%
60%
EXERCISE
CONSULTATION
Exercise consultations attracted significantly more not regularly active participants ( c
2 = 5.03, p<0.05)
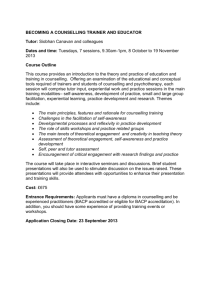
Figure 1:Barriers in developing and implementing evidence based practice
Evidence
Policy making is based on more than evidence
Poor design and implementation of current interventions
Selection of appropriate outcome measures
Ethical and pragmatic difficulties in designing evaluations
Lack of an evaluation culture
Difficulties in conducting systematic reviews
Desegregating knowledge from complex interventions
Model fidelity
Practice
Chapter 11: Conclusions
• It is possible to increase the physical activity levels of sedentary individuals
• short-term (3 – 12 weeks) increases in PA are relatively easy to achieve
• long-term change (6 – 24 months) is hard to achieve
Chapter 11:
Recommendations for researchers
• There is a clear need for research in the area of support for long-term exercise behaviour change
• More specific relapse prevention strategies for physical activity must be explored and tested
•
There is a need to explore different and new media for delivering the messages such as information technology, video conferencing and telephone contact
• Project Active is a good demonstration of how to promote physical activity and it must be repeated in other cultures and with more minimal intervention strategies
• The effect of physical activity counselling with a variety of follow-up options
(such as another consultation, telephone support, postal reminders) needs to be tested over the long term
• More work is required in primary care settings to establish how the primary care team can influence physical activity levels
• Research must focus on the ‘hard to reach’
• Researchers and practitioners must work together to get more of the evidence into practice
Chapter 11:
Recommendations for practice
• Promoting physical activity in the community should involve unsupervised activity opportunities as well as supervised classes
• Walking offers the simplest and most accessible mode of physical activity for the majority of the sedentary population
• All promotion should include cognitive behavioural principles of behaviour change
• Primary care teams should consider training of staff in physical activity promotion.
• Evaluation is central to increasing the available evidence base