Mod1revised
advertisement

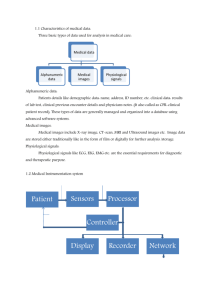
The 12 Lead ECG in Acute Coronary Syndromes Eric Lynn NREMT-P Clinical Education Specialist Amarillo Medical Services Sponsored by: 12-Lead ECG in ACS Course Module I Essential Interpretation Module II Acquisition & Transmission Module III Acute Coronary Syndromes Part 1 Module IV Acute Coronary Syndromes Part 2 Module V The High Acuity Patient Module VI Bundle Branch Block & the ACS Imitators MODULE 1 Essential 12-Lead Interpretation Essential 12-Lead ECG Interpretation Goals Recognize and localize AMI on the 12-Lead ECG Feel comfortable with 12-lead interpretation 12-Lead ECG 12-Lead ECG 12-Lead ECG 12-Lead ECG 12-Lead ECG 12-lead ECG 12-Lead ECG 080.0 0.080 80 milliseconds = 0.08 seconds 12-Lead ECG R Wave Q Wave S Wave QRS Q waves Physiologic Q waves < .04 sec (40ms) Pathologic Q >.04 sec (40 ms) QRS Q wave QS Complex J-Point ST Segment Practice Find J-points and ST segments Practice Find J-points and ST segments ST Segment Compare to TP segment ST TP ST Segment Analysis 12-Lead ECG AMI recognition Two things to know What to look for Where you are looking AMI Recognition What to look for ST segment elevation One millimeter or more (one small box) Present in two anatomically contiguous leads ST Segment Elevation Presumptive evidence of AMI Indication for acute reperfusion therapy Practice Lead “Views” Lead Groups I aVR V1 V4 II aVL V2 V5 III aVF V3 V6 Limb Leads Chest Leads Lead “Views” Anatomical Position Inferior Wall II, III, aVF Left Leg I aVR V1 V4 II aVL V2 V5 III aVF V3 V6 Inferior Wall I aVR V1 V4 II aVL V2 V5 III aVF V3 V6 Inferior Wall Lateral Wall I and aVL Left Arm I aVR V1 V4 II aVL V2 V5 III aVF V3 V6 Lateral Wall V5 and V6 Left lateral chest I aVR V1 V4 II aVL V2 V5 III aVF V3 V6 Lateral I, aVL, V5, V6 Lateral Wall I aVR V1 V4 II aVL V2 V5 III aVF V3 V6 Anterior Wall V3, V4 Left anterior chest I aVR V1 V4 II aVL V2 V5 III aVF V3 V6 Anterior Wall • V3, V4 I aVR V1 V4 II aVL V2 V5 III aVF V3 V6 Septal Wall V1, V2 Along sternal borders I aVR V1 V4 II aVL V2 V5 III aVF V3 V6 Septal • V1,V2 I aVR V1 V4 II aVL V2 V5 III aVF V3 V6 AMI Localization I aVR V1 V4 II aVL V2 V5 III aVF V3 V6 Anterior: Septal: Inferior: Lateral: V3, V4 V1, V2 II, III, AVF I, AVL, V5, V6 AMI Recognition I Lateral aVR II Inferior aVL Lateral III Inferior aVF Inferior V1 Septal V4 Anterior V2 Septal V5 Lateral V3 Anterior V6 Lateral AMI Recognition Know what to look for ST elevation > 1mm Two contiguous leads Know where you are looking Use pocket card as a reference You will soon have this memorized Practice Practice Evolution of AMI • Hyperacute Evolution of AMI • Acute Evolution of AMI • Acute Evolution of AMI • Age undetermined AMI Recognition A normal 12-lead ECG DOES NOT rule out AMI Practice Practice Practice Reciprocal Changes Reciprocal Changes II, III, aVF I, aVL, V leads Practice Practice AMI Recognition Reciprocal changes Not necessary to presume infarction Strong confirming evidence when present AMI Recognition AMI Recognition Imitators of infarct LVH BBB Ventricular beats Pericarditis Early Repolarization Others Summary AMI recognition Know what you are looking for 1mm of ST elevation Two contiguous leads Know where you are looking Positive electrode as an “eye” Pocket card Summary Reciprocal changes Not necessary to presume infarction Strong confirming evidence when present Summary ST segment elevation is presumptive evidence for AMI Other conditions may also cause ST elevation Summary A normal 12-Lead ECG DOES NOT rule out AMI ACS AMI is part of a spectrum of disease know as the Acute Coronary Syndromes