12 Lead ECG Training Module 4
advertisement

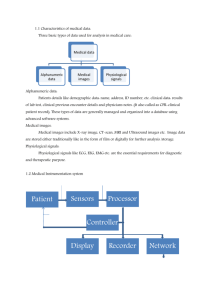
12 Lead ECG interpretation Ischaemic Changes Work Shop Hayley Coxon Topics covered • Recap on ECG format and basics • Normal ECG • ECG changes in myocardial ischaemia/infarction • ST segment • T wave • Q wave • Acute MI locations and reciprocal changes • Other causes of T wave and ST changes • Practice ECGs ECG Paper 1 large box = 0.2 seconds 5 large boxes = 1 second 10 mm/1mv Reference Time 1 small box = 0.04 seconds P, QRS & T Wave Isoelectric line Normal Intervals P-R interval: 0.12 - 0.20 sec (3 to 5 small squares) QRS width: 0.08 - 0.12 sec (2 to 3 small squares) PR interval QT interval QRS complex Q-T interval: 0.35 - 0.43 sec *The PR interval should really be referred to as the PQ interval, however it is commonly referred as the PR interval. Lead Groups Limb Leads Chest Leads (precordial leads) Lead I aVR V1 V4 Lead II aVL V2 V5 Lead III aVF V3 V6 Bipolar Unipolar Unipolar Standard Bipolar Leads I - II III I + Einthovens’ Triangle III II + + Augmented Unipolar Leads + + Augmented Voltage Right (aVR) aVR will always be negative if the limb leads are placed correctly Augmented Voltage Left (aVL) + Augmented Voltage Foot (aVF) Limb leads Left axis -90° -120° -60° -30° aV L -150° aV R 0° I +180° +-30° +150° Right axis +120° III +90° aV F +60° II R Wave Progression r R 1 V6 2 2 1 2 S V1 1 V1 V2 q V3 V4 V5 V6 12 Lead ECG Check List “Remember” Always treat the patient - not the ECG. 1. 2. 3. 4 1. 2. 3. 4. 5. 10 The PR interval is between 0.12 & 0.2 sec (3 -5 small squares). The QRS duration is <0.11 sec (<3 small squares). The QRS complex should be predominantly upright in leads I & II. QRS & T waves tend to have the same general direction in the limb leads. Confirm that aVR is negative (if not check limb lead placement). The R wave in the precordial leads must grow from V1 to at least V4. The ST segment should start isoelectric except in V1 & V2 where it may be slightly elevated. The P waves should be upright in I, II & V2 to V6 There should be no Q waves > 0.04 seconds (1 small square) in width in I, II, V2 to V6. The T wave must be upright in I, II, V2 to V6. Chamberlain DA. Personal communication Normal 12 Lead ECG ECG patterns of myocardial ischaemia and infarction • ST segment depression/elevation • T waves changes • Hyperacute • Inverted T waves • Biphasic T waves • Flattened T waves • Pathological Q waves • U-wave inversion – less well-known ST Segment ST Segment 1 2 3 J Point J point - starting point when measuring ST segment deviation. J Point Examples 1 2 3 4 5 6 T Wave Hyperacute T waves • Broad, asymmetrically peaked or ‘hyperacute’ T-waves are seen in the early stages of STEMI Inverted T waves Biphasic T waves • Myocardial ischaemia • Waves go up then down Flattened T waves • Dynamic T-wave flattening due to anterior ischaemia (left) • T waves return to normal once the ischaemia resolves (right) Q Wave The septum depolarises from left to right Q waves • Represents the normal left-to-right depolarisation of the • • • • interventricular septum Small ‘septal’ Q waves are typically seen in the left-sided leads (I, aVL, V5 and V6) Small Q waves are normal in most leads Deeper Q waves (>2 mm) may be seen in leads III and aVR as a normal variant Under normal circumstances, Q waves are not seen in the right-sided leads (V1-3) Pathological Q Waves > 1 mm wide > 2 mm deep > 25% of depth of QRS complex Seen in leads V1-3 A normal 12-lead ECG DOES NOT rule out an acute myocardial infarction Acute Myocardial Infarction • ST elevation >2mm in V1-V3 and >1mm in all other leads in >2 contiguous leads1. • Myocardial injury presents as raised ST1. • Infarction can present as Q wave1. aVR V1 Septal V4 Anterior II Inferior aVL Lateral V2 Septal V5 Lateral III Inferior aVF Inferior V3 Anterior V6 Lateral I Lateral 1. The Task Force on the management of acute myocardial infarction of the European Society of Cardiology. Eur Heart J 2003;24:28-66 Evolution of an acute myocardial infarction A. Onset D. > 24 Hours B. 15 Minutes C. > 1 Hour E. F. Days Later Months later Location of infarctions Septal AMI V1, V2 Anterior AMI V3, V4 Lateral AMI Inferior AMI II, III, AVF V5, V6 - (I, AVL) Inferior AMI I aVR V1 II aVL V2 III aVF V3 II V4 V5 V6 III II aVF Right Sided Chest Lead Placement Move the standard left chest leads to the right side in the same position V3R Directly between V1 & V4R. V4R Fifth intercostal space, midclavicular line. V5R Level with V4R at left anterior axillary line V6R Level with V5R at midaxillary line (midpoint of the armpit). V4R is the most sensitive indicator of a right ventricular infarction RV Infarction (standard Leads) RV Infarction (Right Sided Leads) V4R V5R V6R Antero-septal AMI V1 V2 V3 V4 I aVR V1 II aVL V2 III aVF V3 V4 V5 V6 Antero-lateral AMI aVL V6 V5 V4 V3 V1 V2 I II I III aVR V1 V4 aVL V2 V1 V5 V4 aVF V3 V6 V2 V5 V3 V6 I Lateral AMI aVL I I aVR V1 V4 II aVL V2 V5 III aVF V3 V6 Reciprocal Changes • If a lead is looking directly at the infarct site it will produce ST segment elevation • When a lead sees the infarct from the opposite perspective, the ST segment may become depressed in that lead II, III aVF I, aVL, V leads Infarction Overview Site Indicative Leads Reciprocal Leads Inferior II, III & aVF I & aVL Septal V1 – V2 None Anterior V3 – V4 None Anteroseptal V1 – V4 None Lateral I, aVL & V5 - V6 II, III & aVF Anterolateral I, aVL & V3 –V6 II, III & aVF Posterior None V1 – V4 ? Posterior AMI V1-V4 Depression Posterior - Lead Placement V1 - V3 are moved round to become V7 - V9. They are placed on the same horizontal plane as V4 V7 Posterior axillary line V8 Midscapular line in between V7 & V9 V4 V4 V9 To the left of the spine V7 V8 V9 Posterior ECG Dynamic Changes in AMI Pre-hospital ECG showing possible hyperacute S-T changes in anterior leads Dynamic Changes in AMI 2nd ECG taken 20mins later, showing established antero-lateral S-T elevation Identify the following 6 ECG infarction sites ECG 1 ECG 2 ECG 3 ECG 4 ECG 5 ECG 6 ECG 7 Other causes of ST Segment Elevation • Pericarditis • Benign early repolarization • Left bundle branch block • Left ventricular hypertrophy • Ventricular aneurysm • Brugada syndrome • Ventricular paced rhythm • Raised intracranial pressure Pericarditis Benign early repolarisation LV Aneurysm Brugarda LBBB Pericarditis Benign early repolarisation Raised Intracranial Pressure Other reasons for inverted T waves • Normal finding in children • Persistent juvenile T wave pattern • Bundle branch block • Ventricular hypertrophy (‘strain’ patterns) • Pulmonary embolism • Hypertrophic cardiomyopathy • Raised intracranial pressure LVH Hypokalaemia Waves go down then up Raised Intracranial Pressure Thank you More practice ECGs?