Airgas template
advertisement

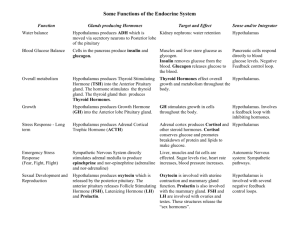
Essentials of Pathophysiology CHAPTER 32 DISORDERS OF ENDOCRINE FUNCTION PRE LECTURE QUIZ TRUE/FALSE Hypopituitarism is characterized by a decreased secretion of pituitary hormones. F Hypothyroidism is evidenced by an increased metabolic rate, restlessness, irritability, tachycardia, diarrhea, and heat intolerance. T Primary adrenal insufficiency, or Addison disease, is caused by destruction of the adrenal gland. T Moon facies, buffalo hump, obesity, amenorrhea, and increased facial hair are manifestations of Cushing syndrome. F Addison disease is a temporary condition. T PRE LECTURE QUIZ Acromegaly Cushing In children, _____________ hormone deficiency interferes with linear bone growth, resulting in short stature or dwarfism. When growth hormone excess occurs in adulthood or after the epiphyses of the long bones have fused, the condition is referred to as ______________. Precocious ______________ is the early activation of the hypothalamic-pituitary-gonadal axis, resulting in the development of appropriate sexual characteristics and fertility. ______________ disease is a state of hyperthyroidism that is often accompanied by goiter and exophthalmos. ______________ syndrome refers to the manifestations of excess cortisol. Graves growth puberty HYPOTHALAMUS- PITUITARY AXIS Releasing hormones from hypothalamus tell the pituitary what to release into the blood Trophic hormones from the pituitary tell specific peripheral glands to grow and produce their hormones Releasing Hormones Trophic Hormones HORMONE DISORDERS Tertiary: abnormality in stimulation from the hypothalamus Secondary: abnormality in stimulation from the pituitary Primary: abnormality in the gland PITUITARY HORMONES Growth hormone FSH and LH TSH stimulate gonads stimulates thyroid ACTH stimulates adrenal cortex QUESTION Which hormone(s) stimulate the ovaries and testes? a. GH b. FSH and LH c. TSH d. ACTH and GH ANSWER FSH and LH Rationale: Gonads are sex organs (ovaries and testes). These organs are stimulated by folliclestimulating hormone (FSH) and luteinizing hormone (LH). b. THE HYPOTHALAMUS CONTROLS GROWTH HORMONE RELEASE GH secretion stimulated by: Hypothalamus Hypoglycemia, fasting, starvation Stress Next Slide GHRH stimulates Somatostatin GHIH inhibits GH inhibited by: Increased glucose levels, free fatty acid release, and obesity Cortisol Anterior pituitary Growth hormone GROWTH HORMONE SITIMULATED BY ? Hypoglycemia, fasting, starvation, Stress ?? It would seem that adequate energy supply would be needed for Growth ? A baseline level of GH exists during normal nutrition mildly stimulated by Deep Sleep, Exercise, and Protein Consumption. GH stimulates IGF-1 During fasting etc. and increased release of GH occurs due to a decrease in GHIH. This produces a protective effect preventing muscle wasting by stimulating lipolysis and FFA metabolism maintaing blood glucose for the CNS Without GH significantly more muscle wasting occurs FUNCTIONS OF GROWTH HORMONE Promotes Growth Inhibits Insulin GROWTH HORMONE DEFICIENCY Idiopathic GH deficiency Lacks hypothalamic GHRH Pituitary tumors, agenesis of the pituitary Cannot produce GH Laron-type dwarfism Hereditary defect in IGF production GROWTH HORMONE EXCESS In childhood: gigantism In adulthood: acromegaly QUESTION Tell whether the following statement is true or false. GH deficiency may result in dwarfism. ANSWER True Rationale: Laron-type dwarfism is caused by a genetic inability to produce normal amounts of GH. Not True. Normal GH abnormal IGF THE HYPOTHALAMUS CONTROLS GONADAL HORMONE RELEASE Excessive GnRH secretion can be stimulated by: Hypothalamic tumors Pituitary tumors Giving high levels of GnRH causes the pituitary to become less responsive and reduces the effects of abnormal GnRH secretion hypothalamus GnRH stimulates anterior pituitary FSH LH production of gametes and gonadal hormones THYROID CONTROL Thyroid releases T3 and T4 Both are carried by binding proteins Why? T3 stimulates metabolism T4 is inactive until converted into T3 in the tissues Both exert negative feedback on the hypothalamus THYROID INSUFFICIENCY DUE TO LACK OF I T3 and T4 are not made There is no negative feedback to the hypothalamus TRH and TSH continue to be made If it is able, the thyroid will grow in response to the TSH THYROID IMBALANCES Hypothyroidism Congenital Acquired º Hashimoto thyroiditis º Thyroidectomy Hyperthyroidism (thyrotoxicosis) Graves disease Thyroid tumors QUESTION Tell whether the following statement is true or false. Simple goiter is caused by increased production of thyroid hormone. ANSWER False Rationale: Simple goiter is the result of iodine (I) insufficiency. Since I is necessary in order to produce thyroid hormone, a deficiency results in low serum levels of T3 /T4. This causes TSH to stimulate the thyroid gland to make more hormone (which it cannot do because it needs I). The cells of the thyroid gland hypertrophy in an effort to function (make thyroid hormone). MAJOR ADRENAL CORTICAL HORMONES • Cortisol • What can cause Cortisol Stimulation? • Hypothalamus releases ?? • Causes the Anterior Pituitary to release ?? • Causes the adrenal cortex to release ?? MAJOR ADRENAL CORTICAL HORMONES Hypothalamus Corticotropin-releasing hormone (CRH) Negative feedback Negative feedback Anterior pituitary Adrenal corticotrophic hormone (ACTH) Adrenal cortex Cortisol Testosterone Aldosterone ACTIONS OF CORTISOL cortisol Increases catabolism plasma proteins increased muscle breakdown free fatty acids increased immune/ inflammatory systems suppressed SNS response increased blood glucose increased ADRENAL CORTICAL DISORDERS Adrenal cortical insufficiency: inability to make all three hormones Primary adrenal cortical insufficiency (Addison disease) Secondary adrenal cortical insufficiency Acute adrenal crisis Excessive adrenal secretion Glucocorticoid hormone excess (Cushing syndrome) Hyperaldosteronism Congenital adrenal hyperplasia Decreased cortisol synthesis; other hormones may be increased or decreased CLINICAL MANIFESTATIONS OF ADDISON DISEASE (CHRONIC ADRENAL INSUFFICIENCY) CLINICAL MANIFESTATIONS OF CUSHING SYNDROME (HIGH LEVELS OF CORTISOL IN THE BLOOD) SCENARIO Three men have adrenal problems. One has hypoaldosteronism, one has an inability to make cortisol, and one has an inability to make testosterone. Question: Which of them is most likely to develop: Hypotension? High CRH levels? Hypoglycemia? Hypervirilization? Decreased libido? Hyperkalemia? SCENARIO Two women have benign pituitary tumors. One woman has lost weight and complains of being hot all the time; she presents as thin and nervous, with tachycardia and exophthalmos The second woman has gained weight in her abdomen and presents with a round face and thin arms and legs with stretch marks; she says that at her last checkup her doctor told her she was prediabetic Question: What hormones are being secreted by the pituitary tumors in these patients? Why?