English Post Partum Hemorrhage Dr A CME 2015
advertisement

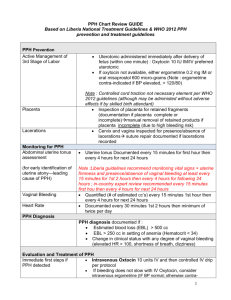
Postpartum Hemorrhage Dr. Alongkone Phengsavanh Objectives • Define and discuss risk factors and causes • Describe management and prevention Postpartum Hemorrhage • Leading cause of maternal deaths worldwide • Responsible for 1/3 of maternal deaths worldwide and 60% in developing countries • Majority of deaths within 4 hours of delivery Postpartum Hemorrhage (PPH) • Primary (immediate) – Hemorrhage in first 24 hours after delivery – 70% due to uterine atony • Secondary (delayed) – Hemorrhage after 24 hours up to 6 weeks postpartum – Caused by • Retained placental tissue • Infection • Definitions – Volume loss (Traditional) – Spontaneous vaginal delivery • >500 cc blood – C/Section • >1000 cc blood • Clinical – Any blood loss that has the potential to produce hemodynamic instability Clinical Findings & Blood Loss Mild Hypovolemia Moderate Hypovolemia Severe Hypovolemia Definition (blood volume) <20% 20 - 40% >40% HR Mild tachycardia >110 bpm tachycardia RR Normal >30 rpm tachypnea Clinical Cool extremities, decreased urine output, dizziness, normal neuro status Marked pallor, hypotension with sitting, anxious state Oliguria / anuria, agitation, confusion, loss of consciousness, BP unstable PPH Etiology • Tone • Tissue • Trauma • Thrombopathy - Uterine tone - Retained tissue / clots - Laceration, rupture, uterine inversion - Coagulopathy PPH Risk Factors - Tone • Overdistended uterus – Polyhydramnios – Multiple gestation – Macrosomia • Uterine muscle exhaustion – Rapid labor – Prolonged labor – High parity • Intra-amniotic infection – Fever – Prolonged Rupture of Membranes • Uterine abnormalities – Fibroid uterus – Congenital uterine abnormalities – Placenta previa / placental abruption • Uterine relaxing agents – Magnesium sulfate – Halogenated anesthetics – Nitroglycerin PPH Risk Factors - Tissue • Retained tissue, abnormal placentation (succinuriate lobe, retained cotyledon) – Incomplete placental delivery – Previous uterine surgery – High parity • Retained blood clots – Atonic uterus PPH Risk Factors - Trauma • Lower genital tract lacerations (cervix, vaginal wall, perineum) – Precipitous delivery – Operative delivery – Poorly timed or inappropriate episiotomy • Caesarean section – extensions / lacerations – Deep engagement of head – Malposition • Uterine rupture – Prior uterine surgery • Uterine inversion – High parity – Fundal placenta PPH Risk Factors - Thrombin • Pre-existing states – Hereditary conditions – History of liver disease • Therapeutic anticoagulation – History of thrombotic disease • Other (DIC, ITP, Pre-eclampsia, placental abruption, severe infection) – – – – – – – Intrauterine fetal demise Bruising Elevated blood pressure Fever Elevated WBC Antepartum hemorrhage Sudden collapse PPH Prevention • Active management of the Third Stage of Labor – Administer oxytocin with delivery of anterior shoulder or immediately after delivery of baby • Oxytocin 10 units IM or 5 units IV – Clamp and cut cord – Palpate uterine fundus & confirm uterus contracting – Perform controlled cord traction with suprapubic counter traction with next strong contraction – Perform uterine massage after delivery of placenta – Examine placenta for completeness Controlled Cord Traction PPH Management • Prevention – Active management of the third stage of labor – Identify patients at potential risk of PPH PPH Management • Primary PPH – Active management of third stage of labor – Call for HELP – ABC (Airway, Breathing, Circulation) – Estimate / measure blood loss – Closely monitor vital signs – Catheterize bladder (urine volume) – Give oxygen – Give oxytocin (IV/IM) or misoprostil (PR) PPH Management – Tone • Determine source of bleeding – Assess the uterine fundus – Do Internal Bimanual Massage of uterus PPH Management – Tissue Examine placenta for completeness Examine maternal side of placenta Examine fetal side of placenta PPH Management – Tissue Manual removal of placenta – if incomplete placenta 2 1 3 4 PPH Management - Trauma • If fundus firm & placenta complete, then examine for trauma – Upper vaginal tract - identify and repair tears – Lower & external genital tract – apply pressure and repair tears PPH Management • If bleeding continues consider – IV oxytocin • Oxytocin 40 units/1 liter Normal Saline run wide open – Misoprostil • 800 ug pr (4 tablets per rectum) – Correct hypovolemia • Normal Saline • Ringers Lactate • Blood products – RBC transfusion PPH Management • Consider transfer to center with additional resources – Surgery • B-Lynch Stitch • Hysterectomy PPH Management Consider aortic compression Uterine inversion • Rare • Caused by over vigorous cord traction • More common in grand multiparous women • Treatment – Replace uterus promptly – Replacement is “last out” is “first in” – Consider uterine relaxation with nitroglycerin Uterine rupture • Can occur with: – Prolonged or obstructed labor – Prior uterine surgery – caesarean section – Grand multiparous women being induced or augmented • Management – Vigorous resuscitation – Emergency laparotomy • Delivery of fetus / repair of uterus • Hysterectomy – Prophylactic antibiotics Secondary PPH • Cause – Retained tissue – Infection – Breakdown of uterine wound following C/S • Management – ABC – treat for shock – Antibiotics – Assess patient carefully for source of bleeding Secondary PPH • After bleeding controlled monitor woman for: – 24 – 48 hours for further bleeding • • • • Urine output Vital signs Uterine tone CBC • Educate patient and family about PPH and when to return to hospital Conclusion – Key message • PPH is a serious obstetrical emergency requiring urgent diagnosis and treatment. • PPH is prevented with Active Management of the Third Stage of Labor. • Patient may need to be transferred to referral hospital if local resources inadequate.