Case study 1 OMED00074
advertisement

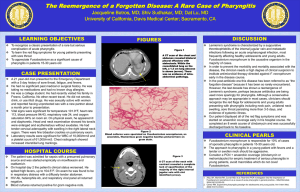
Case study 1 OMED00074 2010 Case study 1 The patient is a 6 years old male who had been in good health with no significant medical problems. In late September he presented to his paediatrician’s office with a complaint of sore throat, fever, headache, and swollen glands in his neck for the past 36 h. On physical examination (PE), he had fever of 38ºC, a red posterior pharynx, yellowish exudate on his tonsils, and multiple, enlarged, tender cervical lymph nodes. Although a definitive diagnosis cannot be made without various tests being carried out, a brief analysis of the patient’s symptoms such as fever, headache, and swollen glands in the neck suggests, or is linked with flu or cold. The evidence of sore throat (usually caused by viral infection and bacteria), inflammation of the pharynx (red posterior pharynx), yellowish exudate on the patient’s tonsils, and multiple, enlarged, tender cervical lymph nodes eliminates the possibilities of a common flu or cold, therefore indicates a more underlining pathology. Whilst sore throat may be associated with various conditions such as influenza, however, tonsillitis, laryngitis and pharyngitis are most prevalent. The term sore throat is medically termed as pharyngitis and can cause exudate, which is infected with bacteria or viruses, as well as dead cells (A. Summers, 2005; Home health UK. 2007). The funnel-shaped tube (pharynx) involves the nasal and oral cavities, the oesophagus, larynx, and trachea. The pharynx has various functions including respiratory and digestive functions, makes allowance for sounds or speech to be produced, and contains the tonsils, immunocompetent tissues responsible in the defence against foreign particles or antigens. Involvement of the tonsils in the patient’s physical examination further highlights the possibility of pharyngitis, but even more-so is the multiple, enlarged, tender cervical lymph nodes. Lymph nodes are constituents of the immune system and function as a filter by destroying foreign substances such as viruses (for e.g., rhinovirus that cause common cold) and bacteria (e.g. group-A β-haemolytic streptococcus in sore throat). Whilst swelling of the lymph nodes signify active lymph against either a bacterial or a virus infection, an enlarged lymph node (in this case, the cervical lymph nodes) is not very common and may suggest a sinister infection, which again, lingers towards pharyngitis (Tortora & Derrickson, 2006; Wikipedia, 2010). 1|Page Author: GG Case study 1 OMED00074 2010 Acute pharyngitis (Fig.1) refers to an inflammation of the pharynx and adjacent lymphoid tissues and affects 25-30 million adults and children in the US each year. The condition is mostly caused due to viral infection such as adenovirus, coronavirus, and Epstein-Barr virus etc. Acute pharyngitis can also be caused by bacteria such as Mycoplasma pneumonia, Arcanobacterium haemolyticum, and group A – hemolytic streptococcus (streptococcus pyogenes) (GABHS), which is the common cause of the illness. The condition may present itself with symptoms such as fever, exudate, erythema (abnormal redness of the skin due to dilation of blood vessels), swallowing and breathing difficulties, and tender cervical lymph nodes. These symptoms are synonymous with that observed in the patient in question. Whilst adult sufferers are restricted to the infection and may not need supportive treatments, however, the condition is most common in children (the patient in this case is 6 years old) and need medical needs (Tasar et al, 2008; DuBose, 2002, Wikipedia, 2010) . Fig 1: Acute Pharyngitis As the symptoms demonstrated by the patient correlates or are in conjunction with that of an acute pharyngitis sufferer, it can be proposed that this patient suffers from acute pharyngitis. However, this is not a definitive diagnosis as treatments or therapy would depend on the type of virus or bacteria involved. As a result, laboratory tests would be assigned and includes; Throat culture – in the case of GABHS for example, the specimen is taken in the tonsillar pillars and the posterior pharyngeal wall, and then grown in a specific medium and left to incubate 2|Page Author: GG Case study 1 OMED00074 2010 overnight. Another test is the Streptococcal test – this involves the identification of specific carbohydrate that constitutes the cell wall of the bacteria (GABHS), and Rapid antigen – which is similar to throat culture but with the advantage of obtaining the culture more faster, hence reducing the risk of contaminating or spreading GABHS, therefore allowing the patient to carry on with their normal duties such as attending school etc (A. Gerber, 1998). REFERENCES Summers, (2005) ‘Sore throats’, Accident and Emergency Nursing, pp.13, 15–16 Gerard J. Tortora and Bryan Derrickson (2006), Principles of Anatomy and Physiology, The United States of America, John Wiley & Sons, Inc, pp. 811, 850, 908. DuBose, (2002) ‘Group A streptococcal pharyngitis’, Honorable Mention, pp.222-224 Tasar et al, 2008 ‘Clinical efficacy of Dexamethasone for Acute Exudative Pharyngitis’, The Journal of Emergency Medicine, pp.363-364 A. Gerber, 1998 Diagnosis and Treatment of Group A Streptococcal Pharyngitis’, Seminars in Pediatric Infectious Diseases, pp. 42-43 Home health UK, 2007. Sore throats. [Online] Available at: <http://www.homehealthuk.com/medical/sorethroat.htm > [Accessed 11 October 2010] Wikipedia, 2010. Acute pharyngitis. [Online] Available at: <http://en.wikipedia.org/wiki/Acute_pharyngitis > [Accessed 11 October 2010]. 3|Page Author: GG Case study 1 OMED00074 2010 4|Page Author: GG