Northwest Portland Area Indian Health Board—Methamphetamine

Northwest Portland Area Indian
Health Board
Methamphetamine Initiative
QuickTime™ and a
TIF F (Uncompressed) decompressor are needed to see this picture.
Dr. Linda Bane Frizzell, Ph.D.
QuickTime™ and a
TIFF (Uncompressed) decompressor are needed to see this picture.
The Northwest Portland Area Indian Health Board (NPAIHB or
Board) is a tribal organization comprised of the forty-three federally recognized tribes in Idaho, Oregon, and Washington. Formed in
1972, NPAIHB provides support in health promotion, disease prevention, health research, and legislative advocacy.
NPAIHB’s mission is ” to assist Northwest tribes to improve the health status and quality of life of member tribes and Indian people in their delivery of culturally appropriate and holistic health care.
”
The Methamphetamine Problem in Indian
Country
History of the Problem:
Methamphetamine (meth) manufacturing, trafficking, sales, and abuse are having a significant impact on
Indian individuals, children, families, and entire communities.
Indian Country’s meth problem stems from the drug’s origins in the central valley of California in the
1990s and its steady spread eastward across the United
States. Indian communities in state after state have been affected. The attraction of outside interests and the prospects of tremendous monetary profits started to find their way to reservations.
Today
Today, a number of tribes have reported serious meth problems among their citizenry, including the San Carlos Apache Tribe, White Mountain Apache
Tribe and Navajo Nation in Arizona, the Cherokee Nation and Chickasaw
Nation in Oklahoma, the Oglala Sioux Tribe in South Dakota, and the Eastern
Shoshone and Northern Arapaho Tribes of the Wind River Reservation in
Wyoming.
Tribal leaders have described in vivid detail the effect this dangerous and highly addictive drug is having in their communities. One example of the devastating impact meth has had on a tribal community was provided by San
Carlos Apache Chairwoman Kathleen Ketchiyan before the Senate Indian
Affairs Committee earlier this year. She testified that as recently as 2005 approximately 25 percent of reservation births resulted in babies born under the influence of meth.
Another tribal leader has stated that an “entire generation in my tribe is being lost to meth.”
Very Limited Data
• The 2003 National Survey on Drug Use and Health suggests that about 5% of the population 12 years of age and older report lifetime use of methamphetamine; use in the past year is about
0.7%.
• Methamphetamine prevalence is much higher in the Western US. Reports from the Community
Epidemiology Workgroup and the Arrestee Drug
Abuse Monitoring system suggest high indicators of use in Hawaii, California, Oregon, Washington,
Idaho, Montana, Nevada and Utah.
Data Continued
• Although, there is little empirical data on the prevalence of methamphetamine use among
American Indians and Alaska Natives, Jan Morley,
Assistant US Attorney, speaking to a gathering of tribal representatives stated:
"Methamphetamine has become an epidemic in our Indian Country. The actual scope of the effects of methamphetamine remains an unknown for most tribal communities . But more importantly it has become epidemic in Indian
Country” (Renee Ruble, Aug. 24, 2003, © 2003
Duluth News Tribune).
The Impact of Methamphetamine on Indian
Communities
• Meth impacts all aspects of a tribal community – culture, people, property, land – not just a few individuals.
• Natural resources on Indian lands such as lakes, public areas, and open fields are at risk due to the dumping of toxic waste that is a by –product of the meth manufacturing process.
• Violence associated with meth production, trafficking, sales and use, BIA and tribal law enforcement and tribal courts personnel have been overtaken by meth-related arrests and cases.
Impact Continued
• Meth also has an impact on every social and economic aspect of Indian communities. It has been closely linked to child abuse and neglect, domestic violence, suicide, reduced employability, degraded physical health, and reduced academic achievement.
• As a result, meth is overwhelming Indian social, economic, education, and health programs. Even more troubling, Indian Country’s isolated reservation and rural communities are viewed by foreign drug cartels as numerous enterprise zones with limited law enforcement and resident populations in need of income-producing opportunities.
The Federal/Tribal Response
• The first step taken to address the meth problem in
Indian Country was to acknowledge its existence.
• In October 2005, the U.S. Attorney General’s
Advisory Committee’s Native American Issues
Subcommittee met in Coeur d’Alene, Idaho, to discuss the problem of meth in Indian Country.
• This historic meeting was attended by over 20
United States Attorneys, the White House Office of
National Drug Control Policy, the Bureau of Indian
Affairs Office of Justice Services (formerly the Office of Law Enforcement Services), the Drug
Enforcement Administration (DEA), the Federal
Bureau of Investigation (FBI), and over 30 tribes.
Federal/Tribal Response Continued
• Consensus was reached that a meth epidemic existed, that it was affecting most tribes in the United
States, and that the best way to tackle the problem from a law enforcement perspective was for federal, tribal and state/local law enforcement to work cooperatively together, by pooling resources and minimizing jurisdictional conflicts, in a common effort to combat meth in Indian Country.
• In January 2006, the federal government followed the lead of many states so that federal law now requires that cold medications containing pseudoephedrine be under lock-and-key or behind pharmacy counters.
New Challenges
• A new challenge for tribal, local, state and federal authorities is in combating the smuggling of illegal drugs from Mexico and Canada across tribal lands that border or are traversed by the U.S.-Mexico and
U.S.-Canadian borders, such as the Tohono
O’odham Nation in Arizona, the St. Regis Mohawk
Reservation in New York State, and the northern plains states (Montana, ND, MN).
• Approximately 80 percent of the current meth supply in the U.S. is due to illegal smuggling from
Mexico.
October 4, 2006: HHS AWARDS $1.2 MILLION TO
ADDRESS METHAMPHETAMINE ABUSE IN NATIVE
AMERICAN COMMUNITIES
HHS Assistant Secretary for Health John Agwunobi today announced the award of $1,175,100 in funds to the American
Association of Indian Physicians (AAIP) and its partners to address the outreach and education needs of Native American communities on methamphetamine (meth) abuse.
This initiative identifies a two-pronged approach, including a national education and information outreach campaign and a series of knowledge transfer activities that would help communities understand promising practices in combating methamphetamine abuse. It brings federal, tribal, state, and local resources together to reach urban and rural Native
American communities and families.
Collaborators
Choctaw Nation, Crow Nation, Navajo Nation, Northern
Arapaho Tribe, and Winnebago Tribe.
The five Tribes will provide technical assistance and document promising practices undertaken by their communities.
National Congress of American Indians, Washington, DC.
NCAI will work to provide technical assistance on a national tribal scale.
Northwest Portland Area Indian Health Board (NPAIHB),
Portland OR.
NPAIHB will contribute regional expertise and will track data and trends within its region.
.
Collaborators Continued
Oregon Health and Science University-One Sky Center,
Portland, OR. (OHSU-OSC).
OHSU-OSC will provide expertise for behavioral health, mental health and substance abuse regarding methamphetamine abuse.
United South and Eastern Tribes (USET), Nashville, TN.
USET will contribute regional expertise and will track data and trends within its region.
NPAIHB Objectives
Objective 1: To define objective data elements available in the IHS Resource Patient Management System (RPMS) and similar data systems, such as Veteran’s Administration and health maintenance organizations.
To explore data quality and identify barriers to effective data availability.
To develop strategies for data improvement in the
RPMS system to allow effective evaluation of methamphetamine use/abuse in Indian Country.
NPAIHB Objectives
Objective 2: Coordinate with the United South & Eastern
Tribes (USET) organization with regard to national survey development and implementation.
Activities: Act as lead agency to pilot questionnaire in
NPAIHB region and with NPAIHB partners in the
Methamphetamine Initiative. Test validity of questionnaire.
NPAIHB Objectives
Objective 3: To identify current treatment service availability, referral, and use by AI/AN populations by the end of the first project year.
Activities: During the data collection phase of the project, current effective prevention and treatment models will be identified. Appropriate protocol will be followed to acquire permission, from respective governing bodies to report these case studies for program development/replication in other communities. Qualitative assessment of the components of these models will be performed using content analysis of programmatic materials.
NPAIHB Objectives
Objective 4: To review products for methamphetamine tool kit.
Develop a logic model for data analysis to use in Indian
Country by the end of the first year.
Develop analytical model for RPMS query and description of RPMS for tool kit.
Develop representative review committee of NPAIHB board delegates to provide tribal review for tool kit.
Why is the Data So Important?
What Data do we have Now?
Literally None: National Data sets do not have American
Indian/Alaska Native samples large enough to statistically base the size of Meth issues in our communities.
Most national surveys include AI/ANs in the “Others” category.
Most national surveys use methods that are “not friendly” to Indian Country, such as: telephone interviews, questions that are not applicable to AI/Ans, no consideration of diversity between tribes.
Universal Behavioral Health Data Issues
• Much of the data is based on paid episodic encounters.
• There are vast limitations for access to behavioral health services.
• There are more limitations on “covered” (insurance) services.
• There remains much stigma attached for individuals who need behavioral health services
• Research to conduit primary epidemiological studies is expensive.
RPMS and Methamphetamine
Coding
Wendy Wisdom, MSW wendy.wisdom@ihs.gov
Phoenix Indian Medical
Center/Division of Behavioral
Health
Background
In the Spring 2005, the IHS/SAMHSA
Methamphetamine Initiative Workgroup was established to help coordinate, collect, analyze, and report information concerning Meth use in
Indian Country.
-Based on discussions by Service Matter
Experts across the country, the decision was made to track with ICD-9 codes.
How are we documenting now?
Documentation of Meth Activities by Clinicians/Data Entry
Diagnosis/Purpose of Visit-ICD9 codes
-only the Amphetamine codes
-discourage clinicians from using Drug Abuse and/or Poly-substance Abuse codes
For local data collections within the BH applications:
-Personal History Factors
-Patient and/or visit flags
What is RPMS?
RPMS is an integrated Public Health information system
Composed of over 50 component applications
Patient and Population based clinical applications
Patient and Population based administrative applications
Financially-oriented administrative applications
www.ihs.gov/CIO/RPMS
Resource Patient Management System
Surgery
Elder Care
Patient
Registration
Laboratory
Emergency
Room
Public Health
Nursing
Pharmacy
Case
Management
PCC
Patient
Database
Appointment
System
RCIS
PCC Data Entry
Behavioral
Health System
Dental
Women’s
Health
Immunization
CHR
Radiology
Data Entry
BHS Data Movement
Third Party
Billing
Local RPMS
BHS
Database
Site-selected links to PCC
PCC
Database
BHS
Export
Reports
Area
National BHS
Database
Web-based
Reports
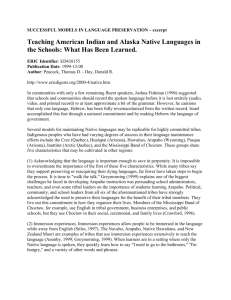
How representative are these reports?
Multiple Data Sources
Data electronically exported to IHS National
Data Warehouse
Resource Patient Management System (RPMS) clinical application exports
Behavioral Health System (continue to track per site)
Mental Health/Social Service (“old” application; all sites should be using BHS)
Patient Care Component
Alaska
4
RPMS BH Sites by Area
Portland
12
Billings
29
Aberdeen
13
Bemidji
25
California
41
Navajo
23
Phoenix
37
Oklahoma
Albuquerque 20
Tucson
24
3
Nashville
23
Programs Using RPMS BHS
IHS
41%
Urban
6%
Tribal
53%
Monitoring your own BH export
Wendy encourages sites to check the website to make sure their BH exports are being received.
www.ihs.gov/cio/bh/ibh-bhs-v3-exports.asp
Data Issues in IHS
In the future, ICD-10 standard code set will include specific codes for methamphetamine-related disorders and death. It will not be adopted until at least 2011.
Funding and reporting are centralized, but administration and governance are decentralized
Over half of Indian health programs are administered autonomously by tribes. Submission of health data from tribes is voluntary
We (IHS) must provide tools for quality care and data collection that are attractive and meet the needs of all constituents, Tribal and Federal. Various needs and priorities by all.
More Information
Northwest Portland Area Indian
Health Board
www.npaihb.org
Project Director-Dr. Linda Bane Frizzell, Ph.D.
Lfrizzell@npaihb.org
527 SW Hall Street Suite 300 Portland, OR 97201
Phone: 218-821-6774 cell
Phone: 503-416-3270 Portland Office
Phone: 218-224-2639 MN Office
Fax: 503-228-8182
Safe Travels Home
QuickTime™ and a
TIFF (Uncompressed) decompressor are needed to see this picture.