Liver Transplant
advertisement

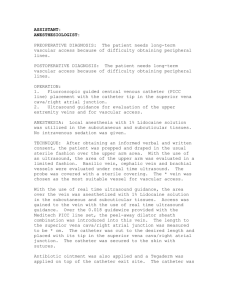
D&C Case Presentation January 26, 2012 Malpositioned central venous catheter Right subclavian vein laceration Right subclavian artery laceration Procedure: Central venous catheter insertion Deceased donor liver transplant 63yo woman Cirrhosis due to Hepatitis C Moderate/Severe decompensation: MELD 24 – Cr 1.76 ; Bilirubin 5.2; INR 1.4; Na 138 Weekly paracentesis for refractory ascities Encephalopathy Presented for Liver transplant on Jan 14 Donor – 34yo man – DCD donor Taken to the operating room for deceased donor liver transplant Central venous catheter MAC (9.0 Fr) Swan-Ganz catheter Chest X-Ray Arterial puncture Pneumothorax Arrythmia Thoracic Duct Injury Guidewire Loss Cardiac Perforation Evens SRT. Surgical Pitfalls: Prevention and Management. Philadelphia: Saunders. 2009. 1. Denys BG, Uretsky BF, Reddy PS. Ultrasound-assisted cannulation of the internal jugular vein. A prospective comparison to the external landmark-guided technique. Circulation. 1993;87:1557-1562. 2. Gualtieri E, Deppe SA, Sipperly ME, Thompson DR. Subclavian venous catheterization: greater success rate for less experienced operators using ultrasound guidance. Crit Care Med. 1995;23:692-697. 3. Mallory DL, McGee WT, Shawker TH, Brenner M, Bailey KR, Evans RG, et al. Ultrasound guidance improves the success rate of internal jugular vein cannulation. A prospective, randomized trial. Chest. 1990;98:157-160. 4. Troianos CA, Jobes DR, Ellison N. Ultrasound-guided cannulation of the internal jugular vein. A prospective, randomized study. Anesth Analg. 1991;72:823-826. 5. Hilty WM, Hudson PA, Levitt MA, Hall JB. Real-time ultrasound-guided femoral vein catheterization during cardiopulmonary resuscitation. Ann Emerg Med. 1997;29:331-336. BG Denys et al from Pitt, 1993 Prospective study, 1230 patients Landmark versus Ultrasound guided: Longer access times (44 sec versus 10 sec) More attempts (2.5 versus 1.2) Decreased successful cannulation on first attempt (38.4 versus 82%) More carotid punctures (25 versus 8) French JLH, Raine-Fenning NJ, Hardman JG, Bedforth NM. Pitfalls of ultrasound guided Vascular access: the user of three/four-dimensional ultrasound. Anaesthesia, 2008:63; 806-813. Liver transplant proceeds Pause prior to bile duct to check for bleeding Abdomen dry Chest tube with minimal output ~30 minutes later – hypotension Chest now has high output Thoracic consulted – Sternotomy Subclavian ligation is well tolerated Thoracic EndoVascular Aortic Repair (TEVAR) Left subclavian may be occluded with or without bypass from left carotid WWII – ligation resulted in 25% gangrene Vietnam registry: Mortality 5 to 10% (earlier series up to 30%) ▪ All due to hemorrhage 5-10%: distal ischemia, gangrene, pseudoaneurysm formation, AV fistula, limb loss Graham et al – 1980 93 patients from 1955 to 1978 Mortality 4.7%; Neurological deficit accounted for major early and late morbidity Intimal flap found at reoperation Left subclavian Right subclavian