Taking a sexual history
Ria Daly
ST5 GU Medicine/Clinical Teaching Fellow
Why can taking a sexual history be difficult?
• Sensitive issues
• Embarrassment (patient and ours)
• Unfamiliarity
• Need to remain unassuming
When would you take a sexual history?
• When patient presents to GU clinic
• When assessing need for screening
• If symptoms could be related to STI/BBV
– Could be related to a number of presentations
Overview
•
•
•
•
•
•
•
•
HPC
PMH/Prev STIs
O+G
DH
FH
SH – inc drug use/travel
SR
Detailed sexual history
HPC – Symptoms of STIs
• Start with an open question
• Asked closed questions regarding other symptoms
• Establish chronology
Common/important GU conditions
•
•
•
•
•
•
•
•
Chlamydia
Gonorrhoea
NSU
Genital warts
Herpes
Complications – PID, epididymo-orchitis, conjunctivitis
Syphilis
HIV
PMH/Prev STIs
• Usual PMH
• Prev STIs
– When, what, treatment, partner treated, abstain form sex as
advised?
O&G
• LMP – risk of pregnancy
• Contraception – are they taking it correctly?
• Previous pregnancies/miscarriages/TOP
• Smear
DH
• Regular medication
• Any recent antibiotics (may inadvertently treat/partially
treat STI)
• If skin problem – any topical treatments?
• Any new drugs?
• Allergies
SH
• Safeguarding/Fraser competence
• Job usually not relevant initially
• Travel/ IV drug use
SR
• Depends on presenting symptom/s
• Fever, rash, diarrhoea
• Joint pain
• Uveitis/conjunctivitis
Sexual history
• What do you need to know?
• Why do you need to know?
• Identify cause of symptoms/presenting complaint
• Identify if they need screening
• (risk of acquisition/transmission)
• Which specimens are required
• Assess whether tests will need repeating
• Identify areas for education/support
• Assess if emergency contraception/PEP is required
Tips
•
•
•
•
•
•
•
•
•
Ensure privacy to take history
See patient alone
Only ask what you need to know (and be able to explain this)
Allow patients time
Acknowledge difficulties
Don’t assume anything!
Respect differences
Be clear with your language
Clarify terms used by patients
• Remember confidentiality including between partners.
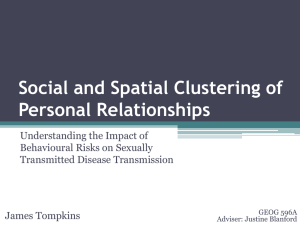
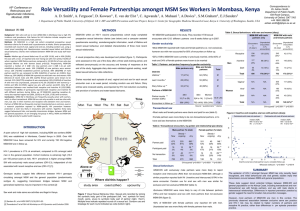
Last Sexual
Contact
Partner
Type of sex
Condom
2/7
RMP
O/A
For anal only
From UK
6/12
Active and passive
CMP
O
No
From UK
1/52
Active
No other partners last 3 months
Known HIV
positive
I need to ask you a few more personal questions if that
is ok…
• When was the last time you had any sexual contact?
• Was that with a regular partner or casual? (if regular – for how long have they
been in a sexual relationship with this person)
• Was that partner male or female?
• Where was that partner from?
• What type of sexual contact was that? Vaginal, oral , anal?
– Are you active or passive (give/receive)?
– Depending on response may ask specifically about use of sex toys, fisting, oral/anal contact
etc
• Any condoms? Sometimes, always, never?
• Prior to that person when did you last have sex with somebody different?
•
•
This very detailed history is the norm for patients presenting to GU clinic.
In other settings, you may not need all this information, or it may not be appropriate to ask due to a
lack of time or privacy. Often, doctors will take enough history to establish that the patient is at risk
then either go ahead with testing or refer to GU.
Further risk assessment
I have a few routine questions I need to ask …
•
•
•
•
•
•
•
Have you ever had a male sexual partner (male patient)?
Have you ever sex with a bisexual male partner (female patient)?
Have you ever paid or been paid for sex?
Have you ever injected drugs?
Had sex with someone who injects drugs?
Had sex with someone who is known to be HIV/Hep B/C positive?
Had sex with someone whilst abroad or someone who has lived/worked
abroad?
Summary
•
•
•
•
•
•
•
•
•
Ensure privacy to take history
See patient alone
Only ask what you need to know (and be able to explain this)
Allow patients time
Acknowledge difficulties
Don’t assume anything!
Respect differences
Be clear with your language
Clarify terms used by patients
• Remember confidentiality including between partners.
Thank you