Dig-Lecture4 - UMF IASI 2015
advertisement

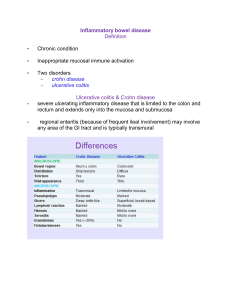
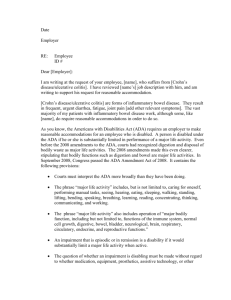
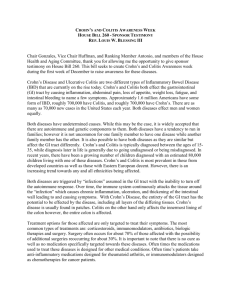
Everybody Loves Sanofi’s Giant Human Colon 20-foot long, walk-through model of a human colon in NYC’s Times Square Anathomy • The ascending colon, descending colon, rectum, and posterior surface of the hepatic and splenic flexures are fixed retroperitoneal structures. • The cecum, transverse colon and sigmoid colon are intraperitoneal and are prone to volvulus because of their location and relative lack of fixation. Anathomy • The longitudinal muscle is an incomplete layer and is seen as three bands of muscle, called teniae coli, located 120 degrees apart around the circumference of the colon. • Haustra coli are sacculations between the teniae and are separated by crescent-shaped folds called plicae semilunares. Sympathetic nerves inhibit and parasympathetic nerves stimulate peristalsis. Macro- and Micro• The colonic wall consists of mucosa, submucosa, inner circular muscle, outer longitudinal muscle and serosa . • The colonic mucosa is similar in organization to the small intestine mucosa except that it lacks villi. • There is no serosal layer in the rectum. Definition • Irritable bowel syndrome (IBS) is characterized by altered bowel habits and abdominal discomfort in the absence of organic disease. • No clear diagnostic markers exist for IBS; thus, all definitions are based on the clinical presentation. • The Rome II criteria for the diagnosis of IBS include at least 3 months of continuous or recurrent abdominal pain or discomfort that has two of the following features: relief by defecation, association with a change in the frequency and a change in stool form ROME II DEFINTION • Symptoms that cumulatively Support the Diagnosis of Irritable Bowel Syndrome: – Abnormal stool frequency (> 3 bowel movements/day and less than 3 bowel movements per week); – Abnormal stool form (lumpy/hard or loose/watery stool); – Abnormal stool passage (straining, urgency or feeling of incomplete evacuation); – Passage of mucus; – Bloating or feeling of abdominal distension DEFINITION -LIMITS• Symptoms based definition due to the absence of a specific biologic “marker”. • Overlap between the definition of irritable bowel syndrome and other functional disorders. • The present definition are not able to differentiate between the subgroups of IBS patients. • The present definition criteria seem to have a different gender sensibility. SYMPTOMS BASED DEFINITION Functional gastrointestinal disorders - a frequent cause for referral to gastroenterologist Epidemiology - Prevalence: 10%-20% (5 and 65%) - more frequent in women (2:1); - all age affected - 20 - 30% presented to doctor - 1%-3% - GP consultation Etiology PATHOPHYSIOLOGY -MECANISMS• Digestive motility disorders; • Visceral hypersensibility; • Involvement of intestinal infection; • Alimentary intolerance and allergy; • Alteration of perception due to psychiatric disorders. PATHOGENIC MECANISMS - Intestinal hypersensibility - Microscopy • irritable bowel syndrome does not involve intestinal inflammation • Research suggests that neuronal degeneration and myenteric plexus lymphocytosis may exist in the proximal jejunum. • Additionally, colonic lymphocytosis and enteroendocrine cell hyperplasia have been demonstrated in some patients. Symptoms Gastrointestinal Symptoms • abdominal pain • alteration in bowel habits • alteration in bowel habits Extraintestinal Symptoms • chronic pelvic pain • genitourinary dysfunction • chronic fatigue syndrome • co-morbidities Abdominal pain • According to the new Rome II criteria, abdominal pain or discomfort is a prerequisite clinical feature of IBS. • • • • hypogastrium 25% the right side 20% the left side 20% the epigastrium 10% Abdominal pain • Is generally crampy or achy, although sharp, dull, gaslike or nondescript pains. • It may be mild enough to be ignored or it may interfere with daily activities. • Defecation may provide temporary relief from the pain of IBS, while meal ingestion may exacerbate the discomfort usually 60 to 90 minutes postprandially. • Pain that is progressive, prevents sleep, leads to anorexia or inability to eat or is associated with weight loss warrants exclusion of organic disease. Alteration in bowel habits • constipation, diarrhea or constipation alternating with diarrhea • long periods of straining may be required for fecal evacuation both in constipation- and diarrheapredominant patients • constipation can persist for weeks to months, interrupted by brief periods of diarrhea • feelings of incomplete fecal evacuation may lead to multiple attempts at stool passage daily Alteration in bowel habits • In diarrhea-prone patients, stools characteristically are loose and frequent but of normal daily volume. • Generally, diarrheal stools occur only during waking hours, often early in the day and an urgent desire to defecate after a meal is reported by 36% of patients. • Fecal urgency and loose stools may develop during stress. Alteration in bowel habits In a 12-week trial study of 59 patients with IBS, Hahn and colleagues 38 found that the population reported pain or discomfort on 50% of days. • on 33% of days bloating was reported • altered stool formation and passage were found, respectively, on 25% and 18% of days • for more than half of the study period 50% of the patients had at least one symptom • The symptoms lasted on average for 5 days or less, although pain/discomfort and bloating tended to last the longest. Gas and Flatulence • Patients with IBS frequently complain of abdominal distention and increased belching or flatulence, all of which they attribute to increased gas. • Quantitative measurements reveal that most patients who complain of increased gas generate no more than a normal amount of intestinal gas. • Studies have shown that most IBS patients have impaired transit and tolerance of intestinal gas loads. • In addition, patients with IBS tend to reflux gas from the distal to the more proximal intestine, which may explain the belching. Bloating Alteration in bowel habits Symptoms not associated with IBS that warrant exclusion of organic disease include: • • • • nocturnal diarrhea rectal bleeding malabsorption weight loss Upper gastrointestinal symptoms (25 and 50%) • • • • dyspepsia heartburn nausea vomiting • IBS symptoms are prevalent in noncardiac chest pain patients, suggesting overlap with other functional gut disorders Extraintestinal symptoms • Patients with functional gut disorders visit primary care physicians three times as often for nongastrointestinal problems as do healthy persons and undergo more appendectomies and hysterectomies. • chronic pelvic pain • genitourinary dysfunction: - dysmenorrhea - dyspareunia - impotence - urinary frequency - nocturia - a sensation of incomplete bladder emptying Extraintestinal symptoms • IBS symptoms are found in 42% of patients with fibromyalgia. • 63% of patients with chronic fatigue syndrome • higher incidences of peptic ulcer disease, hypertension, low back pain, headaches, and rashes than the general population and more commonly report fatigue, loss of concentration, insomnia, palpitations and unpleasant tastes in the mouth COMORBIDITY • About 50% of IBS patients from primary care and gastroenterology clinics have at least one comorbid somatic symptom. • Comorbidity substantially alters the quality of life of IBS patients and adds an additional cost for its treatment. • The presence of commorbidity was suggested to be a new diagnostic criterion. • Specific comorbide somatic condition are Fibromyalgia, Chronic fatigue syndrome, Chronic pelvic pain, Temporo-mandibular joint disorder. • Overlap with other functional gastrointestinal disorders: functional dyspepsia, non-cardiac chest pain, functional ano-rectal pain, fecal incontinence. COMORBIDITY • Overlap with psychiatric disorders such as: - depressive syndromes - anxiety disorder - somatisation Figure 5.33 - Visceral sensations ©Copyright Science Press Internet Services Alarm signs - onset in elderly – increasing intensity – waking up the patient – fever – weight loss – rectoragia Physical findings • The physical examination of the patient usually is normal • Abdominal compression may elicit tenderness that is vague and poorly localized. • Tender bowel loops are commonly palpable. • Masses, adenopathy, hepatosplenomegaly, ascites, blood in the stool or autonomic or peripheral neuropathy are suggestive of organic disease and are not consistent with IBS. Diagnosis • Confident diagnosis of IBS relies on recognition of characteristic symptom profiles as well as the detection of alarm findings (weight loss, bleeding, fever, or palpable masses) which are more suggestive of organic disease. • The symptoms that define IBS also are prominent complaints of many other conditions including malignancies, inflammatory diseases, infections, and ischemic diseases of the gastrointestinal tract as well as some nongastrointestinal conditions. In a questionnaire survey, Manning and colleagues defined four symptoms that were significantly more common in IBS than organic disease 1. 2. 3. 4. relief of abdominal pain upon defecation looser stools with onset of pain more frequent stools with the onset of pain abdominal distention Differential diagnosis • Abdominal Angina Hypothyroidism Anxiety Disorders Inflammatory Bowel Disease Bacterial Overgrowth Syndrome Lactose Intolerance Malignant Neoplasms of the Small Intestine Celiac Sprue Colon Cancer, Adenocarcinoma Endometriosis Food Allergies Postcholecystectomy Syndrome Gastroenteritis Giardiasis Ulcerative Colitis Hyperthyroidism • Fructose intolerance Gastrinoma Infectious colitis Medication adverse effects Secretory diarrhea VIPoma • Functional bowel disorders Functional abdominal bloating • This is characterized by symptoms of abdominal fullness or distension, awareness of audible bowel sounds and excessive flatus with no evidence of either maldigestion and malabsorption or excessive consumption of poorly absorbed fermentable carbohydrate. Functional constipation • This is arbitrarily defined as either persistently difficult, infrequent defaecation or the sensation of incomplete defaecation. • Usually, two or more of the following are present: straining at defaecation; lumpy or hard stools; the sensation of incomplete evacuation; two or fewer bowel movements per week. Functional diarrhea • This is defined as the frequent passage of unformed stool without the presence of other features of irritable bowel syndrome. • Neither abdominal pain nor the frequent passage of formed stools are included in the symptoms. • The diagnosis of functional diarrhoea depends on the presence of two or more of the following: unformed stool; three or more bowel movements per day; increased stool weight, greater than 200 g/day. Functional abdominal pain • The relationship between the abdominal pain and a disturbance of gastrointestinal-tract function is difficult to ascertain. • Abdominal pain is frequent, recurrent or continuous, and characteristically persists for many months. • The relationship between pain and recognizable physiological events such as eating, defecation or menstruation is lacking and evidence of organic disease in the abdomen is absent. • Most of these patients show a major loss of daily functioning capacity and exhibit chronic illness behaviour. Investigations • Laboratory • Imaging studies • Procedures Laboratory • Cell blood count (anemia, inflammation, infection) • Metabolic panel (metabolic disorders, dehydration/electrolyte abnormalities) • Hemoccult test • H2 breaths (bacterial vergrowth) • Microbiologic studies - Ova and parasites (Giardia antigen) Enteric pathogens Leukocites Clostridium difficile toxins Imaging studies • Upper GI barium study with small bowel followthrough: Screen for tumor, inflammation, obstruction and Crohn disease. • Double-contrast barium enema: Screen for neoplasm and inflammation. • Abdominal ultrasonography: Consider this test if the patient has recurrent dyspepsia or characteristic postprandial pain. • Abdominal CT scan: Screen for tumors, obstruction and pancreatic disease. Colon spasm irregular shapes of the intestines ©Copyright Science Press Internet Services Other tests • Direct a lactose-free diet for 1 week in conjunction with lactase supplements. Improvement incriminates lactose intolerance, although the patient's clinical history and response to a trial may be unreliable. Therefore, some gastroenterologists recommend a formal hydrogen breath test. Fructose intolerance must also be considered. • Direct a 48-hour fast. Persistent diarrhea suggests a secretory etiology. • Anal manometry may reveal spastic response to rectal distention or other problems. Anorectal manometry • Anorectal manometry catheter • Distal balloon 320 ml Procedures • Endoscopy directed for many patients with irritable bowel syndrome includes flexible sigmoidoscopy to determine inflammation or distal obstruction. • Esophagogastroduodenoscopy with possible biopsy Indicated for a patient with persistent dyspepsia or if weight loss or symptoms suggest malabsorption or if celiac disease is a concern • Colonoscopy - Indicated for patients with warning signs, such as bleeding; anemia; chronic diarrhea; older age; history of colon polyps; cancer in the patient or first-degree relatives; or constitutional symptoms, such as weight loss or anorexia. A screening colonoscopy should be performed according to published guidelines. Showing characteristic triangular folds of the transverse colon. Conclusion Prognosis • Mostly good. • Not usually serious or life-shortening • IBS causes a great deal of discomfort and distress, but it does not cause permanent harm to the intestines and does not lead to intestinal bleeding of the bowel or to a serious disease such as cancer. • Often IBS is just a mild annoyance, but for some people it can be disabling. Definition • Inflammatory bowel disease (IBD) is an idiopathic and chronic intestinal inflammation. • Ulcerative colitis (UC) and Crohn’s disease (CD) are the two major types of IBD. 2 Specific IBD syndromes • • • • • Proctitis Proctosigmoiditis Left-sided ileitis Ileitis Ileocolitis Epidemiology 24 Geographical distribution of IBD (reproduced with permission, the AGA Teaching Project, 1992) 25 Ethnic prevalence of IBD 50 40 Prevalence (per 105) 30 20 10 0 White Whites (after Kurata et al, 1992) Black Blacks Hispanic Bedouin Arabs Asian Hispanics Other Asians Ethnic Group Incidence of IBD with respect to age and sex (reproduced with permission from Wells Medical Ltd, Binder 1993) 26 Patterns of IBD incidence in previous decades (reproduced with permission from Wells Medical Ltd, Binder 1993) 27 28 Etiological theories of IBD • • • • • • Genetic Smoking Dietary Infection Immunological Psychological? Recent controversies in the pathogenesis of IBD • Genetics • Mycobacterium paratuberculosis • Measles virus 29 30 Genetic factors • It is estimated that between 10 and 20 genes are involved • Susceptibility loci have been located on chromosomes 3, 7, 12 and 16 • The genetic contribution to the aetiology of both Crohn’s disease and ulcerative colitis is polygenic NOT Mendelian 23 Pathological and anatomical features distinguishing ulcerative colitis from Crohn’s disease Ulcerative colitis Crohn’s disease Distal Segmental, proximal Always 50% of cases Normal thickness Thickened Rare Common Superficial layers All layers Superficial Deep Denuded Cobblestones Granulomas 0–4% 50–70% Lymphocytic infiltration Rare Always Fistulae Rare Common Localisation Rectum affected Intestinal wall Adhesions Inflammation Ulcerations Mucous membrane 23 Pathological and anatomical features distinguishing ulcerative colitis from Crohn’s disease Macroscopy UC CD Microscopy UC Excessive active ulcerative colitis changes with cryptitis, cryptic abcesses and ulcers (H-E X200) CD Colonic granuloma in a patient with Crohn disease. Hematoxylin-eosin staining. Courtesy of Dr E. Ruchelli. 22 Differences in clinical presentation between ulcerative colitis and Crohn’s disease Ulcerative colitis Crohn’s disease * *** *** ** * * *** * Blood *** * Mucus * ** Pus * ** Symptoms Pain General malaise Fever Diarrhoea Stools The number of * symbols indicates the frequency with which each symptom is present Clinical presentation of ulcerative colitis • • • • • • • Bloody diarrhoea Fever Cramping abdominal pain Weight loss Frequency and urgency of defecation Tenesmus General malaise 12 Bloody diarrhea/Incontinence • If inflammation is confined to the rectum, blood is seen only on the surface of the stool. • If inflammation is more extensive, blood is mixed in with the stool. • Although bloody diarrhea is considered the dominant symptom in ulcerative colitis, urgency and fecal incontinence bother more. • Incontinence and the fear of incontinence are the most limiting aspects of their disease Physiscal findings • Minimal • tenderness over the affected area of the colon • Rectal examination may reveal tenderness or blood on the glove. • In severe disease, the patient is more likely to be febrile and tachycardic. • Prolonged episodes of severe disease lead to muscle wasting, edema and other signs of malnutrition. • Chronic blood loss results in pallor. • Children with severe disease may have retarded growth and development Initial attack • may be fulminant, with bloody diarrhea present from the beginning • more commonly, the disease begins indolently, with nonbloody diarrhea progressing to bloody diarrhea • symptoms often gradually worsen over the course of a few weeks • can present initially with any extent of anatomic involvement, from disease confined to the rectum to pancolitis and with any degree of activity, from mild diarrhea to toxic megacolon Initial attack • colitis extending to the cecum is seen in only about 20% of patients • limited colitis is more common, with 75% of patients having no disease proximal to the sigmoid • extraintestinal manifestations, most commonly arthralgias and mild arthritis, are present in fewer than 10% of patients at initial presentation • in mild ulcerative colitis, the rectal mucosa is erythematous and edematous on endoscopic examination • in more severe disease, edema is more marked, the mucosa bleeds spontaneously and there is an extensive purulent exudate • in the most severe cases, frank ulceration is seen Initial attack • The outcome of the first attack of ulcerative colitis can be predicted on the basis of the extent of the disease and the severity of the symptoms. • More than 90% of patients with mild disease go into remission after the first attack. • Among patients with more severe disease, a significant number require colectomy and a few worsen and die. • Death occurs primarily in patients who present with toxic megacolon Clinical evaluation • The frequency and severity of diarrhea is a good first guide to the severity of the disease. • Systemic signs and symptoms (fever, hypotension, tachycardia) are markers for the presence of severe disease and demand a more extensive evaluation. • Coexistence of irritable bowel syndrome with ulcerative colitis makes evaluation of the patient’s symptoms more difficult. Table 6: Ulcerative colitis disease activity index. 1. Stool frequency 0-3: normal 1-3: 1-2 stools daily > normal 2-3: 3-4 stools 3-3: 4 stools 2. Rectal bleeding 0-3: None 1-3: Streaks of blood 2-3: Obvious blood 3-3: Mostly blood 3.Mucosal appearance 0-3: Normal 1-3: Mild friability 2-3: Moderate friability 3-3: Exudation, spontaneous bleeding 4. Physician's rating of disease activity 1-3: Normal 2-3: Mild 3-3: Moderate 4-3: Severe Maximum score 3 13 Investigations • • • • Endoscopy Barium enema Laboratory Microbiological studies Endoscopy-Colonoscopy • is required at the initial presentation to help establish the diagnosis and to define the extent of disease • may be useful at presentation of subsequent attacks if there is any question as to whether the attack is a recrudescence of ulcerative colitis • In patients with a past history of ulcerative colitis who develop diarrhea, proctoscopy is a useful method for distinguishing recurrences of ulcerative colitis from infectious diarrhea. • may be indicated if a recurrence of ulcerative colitis is more severe than earlier occurrences, suggesting anatomic extension of the disease. • surveillance for dysplasia • response to drug therapy Colonoscopy • The characteristic findings of ulcerative colitis: • rectal involvement with a confluent distribution • friable mucosa • a blurred vascular pattern • ulcerations in areas of active inflammation Colonoscopy 3 Endoscopic features of ulcerative colitis (reproduced with permission, Schiller et al, 1986) Figure 4.1a - Endoscopic features of active ulcerative colitis ©Copyright Science Press Internet Services Figure 4.1b - Endoscopic features of active ulcerative colitis ©Copyright Science Press Internet Services Figure 4.2 - Ulcerative colitis in remission ©Copyright Science Press Internet Services Figure 4.3 - Severe ulcerative colitis ©Copyright Science Press Internet Services Figure 4.4 - Severe ulcerative colitis with pseudopolyps ©Copyright Science Press Internet Services Barium X-ray • Plain films of the abdomen demonstrate whether there is colonic dilation consistent with toxic megacolon. • Colonic dilation usually occurs without obvious abdominal distention. 4 Radiological features of acute ulcerative colitis (from Wilson et al, 1991) 5 Radiological features of chronic ulcerative colitis (from Wilson et al, 1991) 6 Anatomical location of ulcerative colitis Laboratory • stools – culture • blood: anemia, high sedimentation rate, low Na, K, high creatinine, ureea, renal failure Microbial agents • Intercurrent intestinal infections, either bacterial ( Clostridium difficile, Campylobacter species, Yersinia species) or viral (cytomegalovirus), have been implicated in inducing exacerbations. • Although one study reported high levels of recovery of C. difficile toxin from patients with symptomatic relapses, other studies have reported low rates. • Cytomegalovirus causes gastrointestinal infection and is fairly common in the immunosuppressed host (e.g., patients taking immunomodulators). Natural history • Most commonly, ulcerative colitis follows a chronic intermittent course, marked by long periods of quiescence interspersed with acute attacks lasting weeks to months • A small but significant percentage of patients suffer a chronic, continuous course with persistent symptoms and no complete remission • The risk of relapse after the first attack of ulcerative colitis is a function of the patient’s age at the time of the first attack. Older patients are more likely than younger ones to go long periods without relapse Intestinal complications of ulcerative colitis • • • • • • Fibrosis Shortening of the colon Bleeding Stricture Bowel perforation Toxic megacolon 7 Systemic complications of ulcerative colitis • • • • • • • Arthritis Iritis Erythema nodosum Pyoderma gangrenosum Sclerosing cholangitis Aphthous stomatitis Thromboembolic disorders 8 9 Risk of cancer with ulcerative colitis (reproduced with permission, the AGA Teaching Project, 1992) 10 Risk of colectomy with pancolitis Disease duration Risk of colectomy Year of diagnosis 9% Following 4 years 3% each year Following years 1% per year Relapse of ulcerative colitis during pregnancy 15 Relapse in pregnant 10 women with UC, who were remission at 5 conception (%) 0 1st 2nd (after Willoughby & Truelove, 1980) Trimester 3rd Post-partum 11 Prognosis • Those who present initially with proctitis have a more benign course than those who present initially with more extensive disease. These patients are likely to respond to local therapy and thus are spared the side effects of systemic therapy. • Mortality in patients with ulcerative colitis has decreased dramatically and now life expectancy is similar to that of the general population. • Ulcerative colitis has a significant lifelong impact on a patient’s quality of life. Most patients lead productive lives with 90% employed after treatment of the initial attack Crohn’s disease is a more complex and difficult clinical entity than ulcerative colitis - the diversity of anatomic locations in which it is detected - the effects of this diversity on presentation - clinical course - therapeutic options Definition • Crohn disease is an idiopathic, chronic, transmural inflammatory process of the bowel that often leads to fibrosis and obstructive symptoms, which can affect any part of the gastrointestinal (GI) tract from the mouth to the anus. • This condition is believed to be the result of an imbalance between proinflammatory and antiinflammatory mediators. • Most Crohn disease cases involve the small bowel, particularly the terminal ileum. Epidemiology • The prevalence of Crohn disease is approximately 7 cases per 100,000 population. • The incidence and the prevalence of Crohn disease (especially the colonic subset) seem to have steadily increased over the last 5 decades, mainly in northern climates. Registered number of patients and increased rates of patients with Crohn's disease (CD) and ulcerative colitis (UC) over 30 years in Japan. Epidemiology Race • Data on the racial incidence of Crohn disease seem to show that the condition is uncommon in nonwhites in underdeveloped regions; however, this is not applicable to nonwhites in urban settings, where the rate may even exceed that of whites.1 • Crohn disease is seemingly more common in whites than in blacks or Asians.1 Sex • Most reports show a female-to-male ratio between unity and 1.2:1. Age • The age of onset of Crohn disease has a bimodal distribution. The first peak occurs between the ages of 15 and 30 years, and the second peak occurs between the ages of 60 and 80 years. However, most cases begin before age 30 years. A greater proportion of colonic and distal Crohn disease has been diagnosed in older patients, whereas younger patients have predominantly ileal disease. Etiology • The exact cause of Crohn disease remains unknown. • Current theories implicate the role of genetic, microbial, immunologic, environmental, dietary, vascular, and even psychosocial factors as potential causative agents. • It has been suggested that patients have an inherited susceptibility for an aberrant immunologic response to one or more of these provoking factors. Etiology • Environmental influences such as tobacco use seem to have an effect on Crohn disease. Smoking has been shown to double the risk, whereas in people who smoke, the risk of developing ulcerative colitis is less than in those who have never smoked. • Infectious possibilities such as Mycobacterium paratuberculosis, Pseudomonas species, and Listeria species have all been implicated in the pathogenesis of Crohn disease, suggesting that the inflammation seen with the disease is the result of a dysfunctional but appropriate response to an infectious source. 31 M. Paratuberculosis and Crohn’s disease Mycobacterium paratuberculosis has been thought to have an aetiological role in Crohn’s disease as: • it causes a similar disease in the small intestine in cattle (Johne’s disease) • it can be found in milk • it can be found in Crohn’s disease tissue, although it is also found in other tissues 32 Measles virus and IBD Measles virus has been associated with Crohn’s disease due to: • good epidemiological links between perinatal measles infection and subsequent Crohn’s disease • a possible increase in the incidence of Crohn’s disease in children of mothers who had measles during pregnancy • tissue studies suggest a higher than expected proportion of patients with Crohn’s disease (Forbes, 1997) There are three major patterns of disease distribution • disease present in the ileum and cecum, a pattern seen in 40% of patients at presentation • disease confined to the small intestine, a pattern seen in 30% of patients at presentation • disease confined to the colon, a pattern seen in 25% of patients at presentation • Much less commonly, Crohn’s disease involves more proximal parts of the gastrointestinal tract—the mouth, the tongue, the esophagus, the stomach and the duodenum. Clinical presentation of Crohn’s disease • • • • • • • • Diarrhoea Abdominal pain Bleeding Pyrexia Weight loss Fistulae Perianal disease General malaise Any of these three symptoms may be most prominent, in contrast to ulcerative colitis, in which diarrhea is almost universally the most prominent complaint 21 Initial presentation • may not be dramatic • Patients may complain for months or years of vague abdominal pain and intermittent diarrhea before the diagnosis of Crohn’s disease is considered. Initial presentation • Can usually be characterized as either obstructing or fistulizing. • Obstructive disease is the result of inflammation narrowing the intestinal lumen and obstructing the flow of intestinal contents. Over time, fibrosis and thickening of the intestinal wall also contribute to obstruction. • Crampy abdominal pain, nausea, vomiting, and diarrhea are the major symptoms associated with obstructing disease. • Fistulizing disease occurs when the inflammatory process extends completely through the intestinal wall. The escape of bacteria through these defects in the wall can result in abscesses Diarrhea • The pattern varies with the anatomic location of the disease • In patients with colonic disease, especially with rectal involvement, diarrhea may be of small volume and associated with urgency and tenesmus. • Prolonged rectal inflammation and scarring in the rectum can leave it so rigid and nondistensible that the patient is incontinent. • In disease confined to the small intestine, stools are of larger volume and are not associated with urgency or tenesmus. • Patients with severe involvement of the terminal ileum and those who have had surgical resections of the terminal ileum may have elements of bile salt diarrhea or, in more severe cases, frank steatorrhea. Diarrhea • Strictures in the small intestine may lead to bacterial overgrowth with deconjugation of bile salts and fat malabsorption. • If diarrhea is a product of fat malabsorption, the timing and severity of the diarrhea are functions of the pattern of fat ingestion. • Internal fistulae are common in Crohn’s disease and can lead to diarrhea either by colonization of the small bowel with bacteria, as in enterocolonic fistulae, or through bypass of large segments of absorptive epithelium, as in enteroenteric or enterocolonic fistulae. Abdominal pain • One common pain pattern is cramping right lower quadrant pain in patients with ileocolonic disease. • This pain usually occurs after eating and probably is related to partial intermittent obstruction of a narrowed intestinal lumen. • Pain is caused by stretching of the wall in the dilated segment proximal to the obstruction and by powerful contractions of the small bowel musculature attempting to push intestinal contents through the obstructed segment. • Abdominal distention, nausea, and vomiting may accompany pain in this circumstance Abdominal pain • A second common pain pattern in Crohn’s disease is visceral pain resulting from inflammation of the serosa, as seen in transmural Crohn’s disease. • The pathophysiologic basis of abdominal • pain in nonobstructed or stable patients with Crohn’s disease is less clear. • Crohn’s disease is associated with an increased risk of depression; pain management is more difficult in patients with depression. Weight loss • Weight loss of some degree occurs in most patients with Crohn’s disease, irrespective of anatomic location. • Loss of more than 20% of body weight is less common, occurring in 10% to 20% of affected persons. • Some weight loss is a product of malabsorption, but weight loss usually is a product of diminished intake. • Patients, especially those with small bowel disease, may avoid food because eating brings on pain or diarrhea or, more commonly, because they are anorectic. Crohn’s disease may rarely involve the stomach and duodenum • Epigastric pain similar to that of duodenal ulcer. • Upper gastrointestinal series may show ulceration and narrowing of the antrum and duodenum. • Aphthous ulcers and linear ulcers in the gastric antrum may be seen on endoscopy. Constitutional symptoms • Fever and chills often accompany Crohn’s disease activity • A low-grade fever may be the patient’s first warning sign of a flare of activity. • Fatigue and malaise can reduce the ability to function markedly and may impact work performance negatively. • Although they are more likely to complain of pain and diarrhea, patients may be more bothered by fatigue. In patients in whom fatigue is the dominant symptom, coexisting depression should be considered. EXTRAINTESTINAL MANIFESTATIONS • two major groups: • those in which the clinical activity follows the activity of the bowel disease • those in which the clinical activity is unrelated to the clinical activity of the bowel disease. • Most extraintestinal manifestations occur more commonly with ulcerative colitis or Crohn’s colitis than with Crohn’s disease confined to the small intestine. Extraintestinal manifestations • • • • • Peripheral arthritis Axial arthritis Osteoporosis Renal complications Dermatological manifestations (pyoderma gangrenosum and erythema nodosum) • Eye complications (uveitis and episcleritis) • Thromboembolic complications (arterial as well as venous events) • Hepatobiliary complications (fatty liver, pericholangitis, chronic active hepatitis and cirrhosis) Physical findings • When the disease is active, the patient looks pale, weak, and chronically ill. • Aphthous ulcers in the mouth are common in active Crohn’s disease. • The abdomen may be tender. • Fistulous openings, induration, redness, or tenderness near the anus suggest the presence of perianal Crohn’s disease. • The mucosa at the anal verge may appear purplish because of vascular engorgement. • Fissures in the anal canal can occur; bleeding from these fissures can be confused with active colitis Disease Activity Indices Natural history • Crohn’s disease, like ulcerative colitis, is a relapsing and remitting disease. • About 30% of placebo-treated patients with Crohn’s disease of mild to moderate activity go into remission within 4 months. • Conversely, in a group of patients with Crohn’s disease in remission and not receiving any type of therapy, about 70% remained in remission at 1 year and 50% at 2 years. • Within 10 years of diagnosis, 60% of patients with Crohn’s disease have surgery. • Postoperatively, endoscopic signs of recurrence are seen in 70% of patients at 1 year and recurrence of symptoms is seen in 40% to 50% within 4 years. • Of those patients who have one surgical resection for Crohn’s disease, 45% eventually require reoperation. • The younger the age at onset, the more likely the patient will have a complicated course and the more likely surgery will be required. Investigations • • • • • • Endoscopy Barium X-ray CT MRI Ultrasonography Laboratory Endoscopy • to distinguish between ulcerative colitis and Crohn’s disease • to determine the extent and severity of disease • to assess response to treatment • to screen for dysplasia • Due to its ability to visualize the mucosa directly and obtain biopsies, endoscopy has become established as the primary diagnostic tool. Endoscopy • rectal sparing • areas of active disease interspersed with normal mucosa • sharp, punched-out ulcerations surrounded by normal mucosa • “cobblestoning,” or nodular mucosa often intersected by crossing linear ulcerations. Multiple linear ulcerations are seen on colonoscopy in this patient with Crohn's disease. Crohn's disease can mimic ulcerative colitis on endoscopy. 13 Endoscopic appearance of Crohn’s disease (reproduced with permission, Schiller et al, 1986) Figure 4.15 - Severe Crohn`s colitis ©Copyright Science Press Internet Services Figure 4.19 - Cutaneous opening of a perirectal fistula ©Copyright Science Press Internet Services Figure 4.20 - Typical perianal changes of Crohn`s disease ©Copyright Science Press Internet Services Radiology • Contrast radiology and computed tomography (CT) are both important in the management of Crohn’s disease • Air-contrast radiography is better for assessing mucosal detail, colonic distensibility and the presence of strictures. • In an acutely ill patient with Crohn’s disease, a CT scan is often the preferred initial diagnostic test to answer urgent clinical questions concerning the presence of abscesses or possible obstruction. • Both techniques may be useful to detect the presence of fistulae. 18-year-old woman with Crohn's disease involving colon. Image from double-contrast barium enema obtained 2 days after A reveals longitudinal and perpendicular ulcerations (arrows) in right colon. 36-year-old woman with Crohn's disease. CT enteroclysis image clearly shows small fistula (arrow) between terminal ileum and adjacent ileal loop with severe stranding of surrounding fat tissue. Active Crohn disease and sampling method used for attenuation measurements in 55-year-old woman with endoscopic and pathologic diagnosis of active Crohn disease. (a) Transverse CT scan shows mural thickening and hyperenhancement (arrows) relative to normal ileum (arrowhead). Attenuation for diseased ileum was 122 HU ± 12. Attenuation for normal ileum was 55 HU ± 22. (b) Line profile tool (white line) was placed across the terminal ileal wall to measure attenuation at 1-mm intervals. Sampling is performed across entire bowel wall (from mesenteric fat to water-filled lumen) in the direction of the arrow. (c) Histogram derived from b shows attenuation measurements across small-bowel wall, demonstrating maximal attenuation (arrowhead), perienteric fat (long arrow), and contrast material–filled lumen (short arrow). CROHN’S DISEASE -Radiology- Radiological features of Crohn’s disease (reproduced with permission from McGraw-Hill) (courtesy of Dr Sten Norby Rasmussen, Denmark) 14 15 Anatomical location of Crohn’s disease Investigations • Magnetic resonance imaging (MRI) can be superior to CT scanning in demonstrating pelvic lesions. Because of differential water content, MRI can differentiate active inflammation from fibrosis, and it can distinguish between inflammatory and (fixed) fibrostenotic lesions in Crohn disease. • Radionucleotide scanning may be helpful in assessing the severity and extent of the disease in patients who are too ill to undergo colonoscopy or barium studies Ultrasound • Ultrasonography is helpful in differentiating tubo-ovarian pathology. However, this modality can also detect enlarged lymph nodes, abscesses, stenoses, and even fistulae, and ultrasonography is regarded as a quick and inexpensive screening method to aid in the diagnosis of IBD or to repeatedly evaluate patients for complications. • Rectal endoscopic ultrasonography has been used as an alternative to MRI in the assessment of perianal disease. This technique allows the differentiation of simple from complex fistulae, as well as the assessment of the tracts of the fistulae in relation to the sphincter muscle. Laboratory • • • • • • • • Laboratory findings in Crohn’s disease are largely nonspecific. Anemia resulting from chronic disease, blood loss Nutritional deficiencies (iron, folate, or vitamin B 12) A modestly elevated leukocyte count is indicative of active Crohn’s disease, but a marked elevation suggests the presence of an abscess or other suppurative complication. Thrombocytosis may occur with active disease. The erythrocyte sedimentation rate has been used to monitor disease activity in Crohn’s disease, and it tends to be higher in colonic disease than ileal disease. Hypoalbuminemia is a good indication of disease severity and malnutrition. Ileal disease or resection of more than 100 cm of ileum results in a diminished serum vitamin B 12 level because of malabsorption. Differential diagnosis • Crohn’s Disease and Ulcerative Colitis • Inflammatory bowel disease VERSUS other diseases Intestinal complications of Crohn’s disease • • • • • Fistulae Abscesses Adhesions Strictures Obstruction 16 17 Perianal complications of Crohn’s disease 18 Risk of cancer with Crohn’s disease and ulcerative colitis (adapted from Hamilton, 1985, with permission) Prognosis • Although Crohn disease is a chronic condition with recurrent relapses, appropriate medical and surgical therapy helps patients to have a reasonable quality of life. • Medical therapy becomes less effective with time and surgery for underlying complications is required in nearly two thirds of patients at some point in their disease. • The mortality rate increases with the duration of the disease and GI tract cancer is the leading cause of disease-related death, including colorectal, small bowel adenocarcinoma, lymphomas, and squamous cell carcinomas arising in association with a chronic fistula to the skin. Some studies have also shown an association between Crohn disease and respiratory cancers. • Acute regional enteritis, which is often discovered during laparotomy for suspected appendicitis, has an excellent prognosis. The acute episode is treated conservatively, and two thirds of patients may not have subsequent evidence of regional enteritis. Intestinal Semiology “As you could kill time without injuring eternity” Henry David Thoreau