A Platform for Collaboration PPT

The Cardiac Hybrid OR
A Platform for Collaboration
Objectives
• Summarize key steps in the development and operation of a Cardiac Hybrid OR
• Highlight Hybrid OR best practices
• Provide resources and references for additional information about Hybrid ORs
Table of Contents
• A Paradigm Shift in Cardiovascular Care
• The Cardiac Hybrid OR
• A Platform for Collaboration
• Key Steps in Building and Operating
• References & Resources
A Paradigm Shift in Cardiovascular Care
Image courtesy of Maquet
Hybrid Cardiovascular Procedures
The number of hybrid and minimally invasive cardiovascular procedures is expanding rapidly
• Hybrid and minimally invasive procedures have resulted in decreased morbidity and mortality of elderly patients
• Minimally invasive procedures reduce hospital stays and recovery time
Most Common Targets of Hybrid
Cardiac Procedures
The success of these procedure has increased the need for increased collaboration between cardiothoracic surgeons, vascular surgeons, and interventional cardiologists
References: Byrne 2008, Kpodonu 2009, Nollert 2010
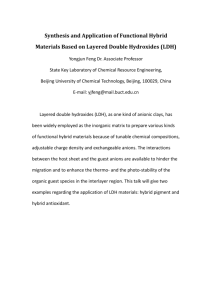
Multidisciplinary Cardiovascular Team
To ensure the success of the hybrid approach, the multidisciplinary team approach has developed
– Facilitates joint pre-operative decision-making and intra-operative collaboration between surgery and cardiology
Old Paradigm
Interventionalist
Emerging Paradigm
Interventionalist
Patient
Cardiologist Surgeon
Reference: Maisano 20120
Cardiologist
Patient
Surgeon
Image courtesy of Maquet
The Cardiac Hybrid OR
What is a Hybrid OR?
• Fully equipped surgical suite that facilitates collaborative and efficient patient care
– Combines all components of a cath lab and surgical OR
– The ideal setting to enable hybrid procedures to be done singly, sequentially, or concurrently
Potential Benefits
• Facilitates interdisciplinary approaches to care
• May improve outcomes and safety
• Streamlines patient flow by eliminating patient transfers and staging
• May increase access to care by expanding population for specific procedures
• Flexibility for future innovation in care delivery and procedures
Reference: Kpodonu 2009, Odle 2011
Potential Challenges
• Requires cross-specialty alignment
• Increases operational complexity
(including staffing and training)
• Large capital investment
2012 ACCF/SCAI Expert Consensus highlights the benefits of a hybrid suite:
• A Platform for Collaboration
– “Although the hybrid suite is designed to meet the needs of an increasingly complex patient population, it also serves as a platform for collaborative work between subspecialists.”
• Multi-functionality
– “In some hybrid suites, operators can perform cardiovascular procedures ranging from the most straightforward PCI to aortic arch reconstruction. As a result, different teams across different subspecialties can benefit from the hybrid suite
.”
2012 American College of Cardiology Foundation/Society for Cardiovascular Angiography and Interventions Expert
Consensus Document on Cardiac Catheterization Laboratory Standards Update
“With the hybrid room, you have something that’s much greater, much larger than each piece.
It really is amazing to see, once it comes together, how the thought process of everybody involved changes. You’re no longer thinking in terms of what any individual person or discipline does but really more in terms of what we do together and that in the end is a clear benefit to the patients.”
Newell Robinson, M.D.
Chairman, Department of Cardiothoracic and Vascular Surgery
St. Francis Hospital, Roslyn, NY
The Cardiac Hybrid OR
Key Steps in Building and Operating
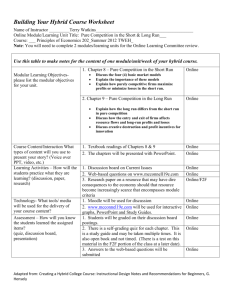
Key Steps in Building & Operating a Hybrid OR
Phase I
Planning
•
Institutional Fit
• Financial Analysis
•
Planning Team
• Vendor
Collaboration
•
Site Visits
Phase II
Design &
Construction
•
Location & Space
• Room Design
•
Table
• Imaging
•
Audiovisual &
Communications
• IT System
Phase III
Staffing &
Operations
•
Staffing
• Training
•
Scheduling
• Protocols
•
Hybrid OR
Committee
• Inventory
Management
Institutional Fit Financial Analysis Planning Team Vendor Collaboration Site Visits
Institutional Fit
The following potential benefits should be considered when assessing the value of a Hybrid OR:
•
New interdisciplinary approaches to care
– Enhanced imaging capabilities enable more advanced procedures
•
Potential to improve outcomes & safety
– Fewer handoffs between teams
– Fewer episodes of anesthesia
– Reduced radiation exposure and use of contrast
– Immediate surgical option possible if required as backup
•
Flexibility for future innovation in care delivery and procedures
– Growing number of hybrid procedures and indications
– Hybrid OR may be especially suited to robotic procedures
The Hybrid OR has the potential to transform an institution’s cardiac patient care, but increases operational complexity and requires a culture of collaboration.
Reference: Odle 2011
Financial Analysis Planning Team Institutional Fit Vendor Collaboration Site Visits
Financial Analysis
• The cost to build a Hybrid OR typically ranges from $1-$5M
• Most projects take a total of 12-18 months for design and build.
• Institution needs to have the right type and volume of procedures to justify the cost
• Equipment vendors can provide an ROI calculator
Not every institution will have the right type and volume of procedures to make the project financially viable
References: Belkin 2009, Kpodonu 2010, Deshchenko 2011
Institutional Fit Financial Analysis Planning Team Vendor Collaboration Site Visits
Planning Team
A large group of stakeholders needs to be brought together at the earliest stages of the planning process
Administration
• Hospital administration
• Business managers
• Internal applications technology specialist
• Information technology specialist
Medical Staff
• MDs that will use the facility
• Anesthesiology
• Radiology and echo
• Perfusion technician
• OR and cath lab nurse/nurse managers
• Infection control specialist
Design/Engineer/
Construction
• Architect
• Interior designer
• Internal hospital facilities manager
• Building construction manager
Early collaboration among cross-functional stakeholders will help prevent design flaws and friction
References: Hirsch 2008, Odle 2011
Institutional Fit Financial Analysis Planning Team Vendor Collaboration Site Visits
Design and Equipment Vendors
• Use of an overall designer/architect is important
• A consulting engineer can help craft detailed lists of requirements and detailed RFPs as planning advances
• Review of proposals should include the core planning team
Because each Hybrid room is different, design and equipment vendors play a fundamental role in helping the institution identify the room suited to its unique needs
Reference: Hirsch 2008
Financial Analysis Planning Team Institutional Fit Vendor Collaboration Site Visits
Site Visits
• Visiting an operational Hybrid OR is an important step in the planning process
– Dozens of decisions go into the development of a Hybrid OR
– Once the room is built, it will be difficult to make changes
– Site visits allow the team to understand the “whys” behind decisions made by other institutions, and what they would have done differently
• Visits should include a multidisciplinary subgroup of the core planning team.
Site visits are an essential step to help the planning team leverage the experiences of other institutions
Reference: Belkin 2009
Key Takeaways: Planning Phase
• The Hybrid OR has the potential to transform an institution’s cardiac patient care, but increases operational complexity and requires a culture of collaboration.
• Not every institution will have the right type and volume of procedures to make the project financially viable
• Early collaboration among cross-functional stakeholders will help prevent design flaws and friction
•
Because each Hybrid room is different, design and equipment vendors play a fundamental role in helping the institution identify the room suited to its unique needs
•
Site visits are an essential step to help the planning team leverage the experiences of other institutions
Key Steps in Building & Operating a Hybrid OR
Phase I
Planning
•
Institutional Fit
• Financial Analysis
•
Planning Team
• Vendor
Collaboration
•
Site Visits
Phase II
Design &
Construction
•
Location & Space
• Room Design
•
Table
• Imaging
•
Audiovisual &
Communications
• IT System
Phase III
Staffing &
Operations
•
Staffing
• Training
•
Scheduling
• Protocols
•
Hybrid OR
Committee
• Inventory
Management
Location & Space Room Design Table Imaging
Audiovisual &
Communications
IT System
Location & Space
• The Hybrid room is ideally collocated near cath lab and ORs
– If ORs are separated from cath labs, it is more common to collocate near other ORs for quick access to equipment and personnel
• If modifying or combining existing rooms:
– OR advantage is that surgical core already exists
– Cath lab advantage is that lead lining is in place
• Average room is ~1000 sq ft to accommodate people and equipment
– There may be up to 20-25 people in the room during a procedure
– Need enough space for two teams to prep
– Headroom is crucial with at least 10 feet clearance
Existing space and the cost of retrofitting will determine whether an institution should modify or build a completely new room
References: Kpodonu 2009, Bashore 2012
Location & Space Room Design Table Imaging
Audiovisual &
Communications
IT System
Room Design: Floor Plan
• Building a full-scale cardboard mockup in an unused space reveals workflow and equipment space issues
– Vendors can develop 3D layout but this still doesn’t give as comprehensive an understanding as a mockup
– All stakeholders need to be involved with this exercise which typically results in changes to the room’s layout
• Flexibility and versatility of the hybrid room is very important
– Need to accommodate varying procedural requirements: different teams, variable table positions, and various imaging modalities
• Making key decisions up front will allow team to understand, rather than guessing, how all of the variables will work together
Making equipment and design decisions up front, along with building a fullscale cardboard mockup of the room, will optimize the plan prior to construction
Location & Space Room Design Table Imaging
Audiovisual &
Communications
IT System
Room Design: Ceiling Plan
• The ceiling plan represents one of the most challenging steps in the planning of a hybrid suite
• Key considerations for a very tight space
– Surgical lighting
– Monitor booms
– Laminar flow ceiling
– Cameras
– C-arm (if ceiling mounted)
Getty Images
• Headroom is crucial with at least 10 feet clearance required
The ceiling plan is one of the most challenging steps requiring many components to fit into a very tight space
Reference: Kpodonu 2009
Location & Space Room Design Table Imaging
Audiovisual &
Communications
IT System
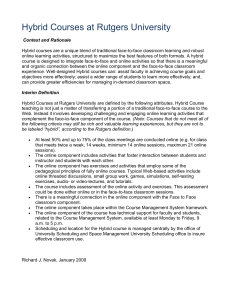
Table
Image courtesy of Maquet
• Table design must accommodate and optimize usefulness and safety of imaging equipment
– Floating tables, similar to those used in the cardiac cath lab allow full coverage of the body in most situations
– Lead shields should be incorporated into the table to reduce radiation exposure to the operators
• Table needs to meet the requirements of both interventional cardiologists and surgeon
– Tradeoffs will likely need to be made
– e.g. surgeon’s preference for a breakable tabletop
• Many hybrid rooms position the table diagonal to the room in order to maximize space
The table must accommodate the needs of various stakeholders and will likely require tradeoffs
References: Belkin 2009, Bashore 2012
Location & Space Room Design Table Imaging
Audiovisual &
Communications
IT System
Imaging
• Hybrid suite imaging system will include most advanced imaging systems for preoperative planning and intraoperative use:
– Superior image quality
– Quick and detailed information
– Minimal X-ray exposure
– Image routing, storage and management
– Delay Obsolescence
• Displays are ideally available in all four quadrants of the room
Image courtesy of Maquet
State of the art imaging systems may represent up to half the cost of the project
References: Kpodonu 2009, Nollert 2010
Location & Space Room Design Table Imaging
Audiovisual &
Communications
IT System
Audiovisual and Communications
• Requires integration of all imaging modalities and media
• Two-way audio communication between hybrid room and control room is important
•
Real-time observation and education with remote-site conferencing are especially important for academic institutions
• Including a telephone router allows for hands-free direct conversations with consulting colleagues and referral physicians
References: Hirsch 2008, Belkin 2009
Location & Space Room Design Table Imaging
Audiovisual &
Communications
IT System
IT System
• Image integration
– DICOM-compatible system for image transfer and archiving
– Capability to route images into and out of the room
– A PACS can allow retrieval and viewing of multi-modal images
– Angiography is very data-intensive; need to provide for storage beyond the short-term
• EMR integration
– System should link to archived images
• Inventory-management
– RFID beginning to appear
• Scheduling software
Reference: Hirsch 2008
Key Takeaways: Design & Construction
• Existing space and the cost of retrofitting will determine whether an institution should modify or build a completely new room
• Making equipment and design decisions up front, along with building a full-scale cardboard mockup of the room, will optimize the plan prior to construction
• The ceiling plan is one of the most challenging steps requiring many components to fit into a very tight space
• The table must accommodate the needs of various stakeholders and will likely require tradeoffs
• State of the art imaging systems may represent up to half the cost of the project
Key Steps in Building & Operating a Hybrid OR
Phase I
Planning
•
Institutional Fit
• Financial Analysis
•
Planning Team
• Vendor
Collaboration
•
Site Visits
Phase II
Design &
Construction
•
Location & Space
• Room Design
•
Table
• Imaging
•
Audiovisual &
Communications
• IT System
Phase III
Staffing &
Operations
•
Staffing
• Training
•
Scheduling
• Protocols
•
Hybrid OR
Committee
• Inventory
Management
Staffing Training Scheduling Protocols
Hybrid OR
Committee
Inventory
Management
Staffing: Two Models
• Dedicated multidisciplinary team model
- Members usually recruited from current OR or cath-lab staff
- Reduces redundancy
- Can be difficult to maintain over time
- Leads to the development of unique hybrid skills
• Flex-team (“pooled”) model
- More common today
- Cross-training of current OR and cath-lab staff
- Requires close scheduling coordination
- Blending/integrating staffs
- May be less efficient
The choice of a dedicated or flexible staffing model will be driven by the unique needs of each institution
Staffing Training Scheduling Protocols
Hybrid OR
Committee
Inventory
Management
Training
• Significant didactic and hands-on education is required
– Usually 3-6 weeks for both physicians and staff
• Cross-training gives an opportunity to strengthen relationships within the extended team
• Conducting several full-team mock cases that cover the spectrum of procedures is valuable
• Important to have formal full-team debriefing sessions after procedures
Training is extensive, involving both didactic and hands-on education
Staffing Training Scheduling Protocols
Hybrid OR
Committee
Inventory
Management
Scheduling
• Some centers have gone to integrated OR scheduling, with openblock time in the hybrid
• For others, a structured approach has been more effective
– e.g. certain days per week assigned to different specialties
– Teamwork and flexibility is critical due to unpredictability of scheduling
• Priority should be given to truly hybrid cases and those possibly requiring conversion
While Hybrid procedures should take precedent, from a practical/volume standpoint most institutions will also need to utilize the room as a functional
OR or cath lab
Staffing Training Scheduling Protocols
Hybrid OR
Committee
Inventory
Management
Protocols
• Joint review and development by all the clinical teams is essential
• Some centers have an ongoing best-practices team that meets monthly and is responsible for updates and education
With multiple teams working in the hybrid OR, protocol development requires compromise and adaptation
Staffing Training Scheduling Protocols
Hybrid OR
Committee
Hybrid OR Committee
• Include key stakeholders
– Start by drawing from members of planning team
• Monthly hybrid OR conference can be useful:
– Discuss cases
– Review operations, including performance metrics
– Identify and address problems
– Learn about new technologies
Inventory
Management
An ongoing Hybrid OR committee can optimize operations, address unforeseen issues, and help with the introduction of new technologies
Staffing Training Scheduling Protocols
Hybrid OR
Committee
Inventory
Management
Inventory Management
• A designated inventory-manager can partner with cath lab and surgical OR counterparts to ensure proper stocking
• RFID is beginning to appear in more institutions
•
Some centers have additional inventory in the equipment room adjacent to the hybrid OR
Inventory management is essential to smooth operations but is often overlooked during the planning phase
Reference: Belkin 2009
Key Takeaways: Staffing & Operations
•
The choice of a dedicated or flexible staffing model will be driven by the unique needs of each institution
•
Training is extensive, involving both didactic and hands-on education
•
While Hybrid procedures should take precedent, from a practical/ volume standpoint most institutions will also need to utilize the room as a functional OR or cath lab
• With multiple teams working in the hybrid OR, protocol development requires compromise and adaptation
• An ongoing Hybrid OR committee can optimize operations, address unforeseen issues, and help with the introduction of new technologies
• Inventory management is essential to smooth operations but is often overlooked during the planning phase
Summary
• Hybrid ORs are becoming a standard part of cardiovascular programs and have the potential to improve patient care
• There is no standard model that can be broadly applied today
• The decision whether to build, how to build, and how to manage a hybrid OR will need to be customized to the unique circumstances of a particular institution
• Hybrid ORs require close cooperation by a cross-specialty team
• The cost is typically $1-$5M and requires an 18-month total planning process
Acknowledgements
This overview was developed with input from personnel at the following institutions:
Banner Good Samaritan Medical Center
Phoenix, AZ
Portneuf Medical Center
Pocatello, ID
St. Francis Hospital
Roslyn, NY
University of Kansas Hospital
Kansas City, KS
The Cardiac Hybrid OR
References & Resources
Published References
Bashore TM, Balter S, Barac A, et al. 2012 American College of Cardiology Foundation/
Society for Cardiovascular Angiography and Interventions Expert Consensus
Document on Cardiac Catheterization Laboratory Standards Update. J Am Coll
Cardiol 2012;59: 2221-305
Byrne JG et al. Hybrid cardiovascular procedures. JACC Cardiol Interv 2008;1:459-68.
Hirsch R. The Hybrid Cardiac Catheterization Laboratory for Congenital Heart Disease:
From Conception to Completion. Cath Cardiovasc Interven 2008;71:418-28.
Klein LW et al. The catheterization laboratory and interventional vascular suite of the future: anticipating innovations in design and function. Catheter Cardiovasc Interv
2011;77:447-55.
Maisano F et al. Hybrid rooms for transcatheter valve interventions: rationale, vision and technical requirements. Intervent Cardiol 2010;2(10):503-10.
Kpodonu J. Hybrid Cardiovascular Suite: The Operating Room of the Future. J Card
Surg 2010;25:704-9.
Kpodonu J and Raney A. The cardiovascular hybrid room a key component for hybrid interventions and image-guided surgery in the emerging specialty of cardiovascular hybrid surgery. Interact Cardiovasc Thrac Surg 2009;9:688-92.
Odle TG. Managing transition to a Hybrid Operating Room. Radiol Technol 2011;83(2):
165CI-181CI.
Online References
Belkin M. The design and implementation of hybrid operating rooms. Veith Symposium
2009 (www.veithsymposium.org/pdf/vei/2761.pdf).
Deshchenko O. Special report: the case for the hybrid OR. DOTmed.com (August 2011)
Nollert G et al. The cardiovascular hybrid OR: clinical and technical considerations.
CTSNet.org (March, 2010).
From theHeart.org:
Vassiliades TA and Zimrin DA. Hybrid revascularization: the best of both worlds.
(www.theheart.org/documents/sitestructure/en/content/programs/1065241/transcript
.pdf)
Miller R. Hybrid revascularization strategy driven by new technology, and soon, new data. January 31, 2011. (www.theheart.org/article/1179057.do)
From Cath Lab Digest (CathLabDigest.com):
Kerr JF. Keys to success in designing a hybrid cath lab. 2009;17(3).
Kpodonu J. The cardiovascular hybrid surgical room: evolving into the future of cardiovascular surgery. 2012;20(3).
Rihal CS. Hybrid lab planning and perspectives. 2010;18(11).
Online References
From Endovascular Today (EVToday.com):
Peeters P et al. The catheterization lab of the future (March 2008).
Benjamin ME. Building a modern endovascular suite (March 2008).
Eagleton MJ and Schaffer JL. The vascular surgery operating room (August 2007).
From Imaging Technology News (ITNonline.com):
Fornell D. Planning for a Hybrid Suite (July 8, 2010).
Fornell D. How to Plan for a Hybrid OR (September 21, 2011).
Mateo D. Hybrid Suites Open Doors (March 3, 2010).
From Cardiovascular Business (CardioVascularBusiness.com):
Making the Case for a Hybrid Interventional OR (May 2011; article 27223).
ACCA: Making the Case for a Hybrid OR, How One Hospital Did It (April 2011; article
27258).
Cath Lab Update: Hybrid Adoption and PCI Imaging Tools (August 2010; article
23370).
Related Guidelines
Coronary Revascularization Guidelines
Hillis LD et al. ACCF/AHA guideline for coronary artery bypass graft surgery. JACC
2011;58(24):e123-e210.
Levine GN et al. 2011 ACCF/AHA/SCAI guideline for percutaneous coronary intervention. JACC 2011;58(24):e44-e122.
Wijns W et al. Guidelines on myocardial revascularization: the Task Force on Myocardial
Revascularization of the European Society of Cardiology (ESC) and the European
Association for Cardiothoracic Surgery (EACTS). Eur Heart J 2010;31:25-1-55.
Endovascular Guidelines
Fanelli F and Dake MD. Standard of practice for the endovascular treatment of thoracic aortic aneurysms and Type B dissections. Cardiovasc Intervent Radiol 2009;32:849-
60
Hodgson KJ et al. Clinical competence statement on thoracic aortic repair (TEVAR): multispecialty consensus recommendations, a report of the SVS/SIR/SCAI/SVMB
Writing Committee to develop a clinical competence standard for TEVAR. J Vasc
Surg 2006;43(4):858-62.
Related Guidelines
Transcatheter Aortic Valve Replacement Guidelines
Holmes DR and Mack MJ. Transcatheter valve therapy: a professional society overview from the American College of Cardiology Foundation and the Society of Thoracic
Surgeons. Ann Thorac Surg 2011;92:380-89.
Tommaso CL, Bolman RM, Feldman T, et al. SCAI/AATS/ACCF/STS multisociety expert consensus statement: operator and institutional requirements for transcatheter valve repair and replacement: Part 1 TAVR. J Am Coll Cardiol 2012.
Cardiac Catheterization Laboratory Standards
Bashore TM, Balter S, Barac A, et al. 2012 American College of Cardiology Foundation/
Society for Cardiovascular Angiography and Interventions Expert Consensus
Document on Cardiac Catheterization Laboratory Standards Update. J Am Coll
Cardiol 2012;59: 2221-305
Additional Resources
•
For Hybrid OR case studies, visit www.hybridOR.medtronic.com
• For detailed information about Hybrid OR equipment, to take a virtual tour of a Hybrid OR, or to find information about alliances that offer integrated solutions, visit the websites of hybrid equipment manufacturers (partial list)*
– GE
– Siemens
– Maquet
– Philips
– Skytron
– STERIS
– Toshiba
•
The Advisory Board Company ( www.advisory.com
) has developed extensive Hybrid OR reports and analysis for member institutions
* Medtronic does not recommend or endorse any manufacturer or their equipment and appearing on this list should not be construed as a recommendation or endorsement .
UC201206539 EN © 2012 Medtronic, Inc.