Emma Hanson KCC DDN Logic Model
advertisement

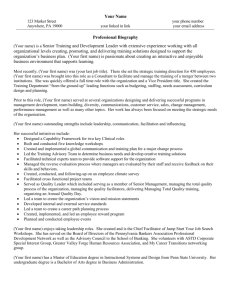
Delivering Differently in Neighbourhoods OVERARCHING LOGIC MODEL Support individuals’, carers’ and communities’ resilience within Adult Social Care – Supporting people to support themselves and others GOAL Transformational change is urgently needed to secure a sustainable model of social care which will continue to meet the needs of the most vulnerable people in our communities. Delivering Differently in Neighbourhoods aims to work with local residents to codesign and develop community owned enterprise to deliver alternative models of care and support which are more community focussed and accountable - thereby reducing health and social care costs. CONTEXT The biggest demand pressure facing local government is from Adult Social Care because of ageing populations, increased longevity and rising expectations combined with the required dramatic budget reductions. The two communities which are the focus of Delivering Differently in Neighbourhoods in KCC are Wye and Hinxhill, and Newington. Wye and Hinxhill has 2282 residents of which 35% are over 65 and 54 people are 90 or over. There are 28 people who receive an ongoing support package. The total annualised average spend is over £358,000 - in addition to this will be many people who fund their own care. Newington has 5210 residents of which 14.5% are over 65 and 20 people are 90 or over. There are 51 people receiving an ongoing support package. The total annualised average spend is over £168,000 - with less people funding their own care. INPUTS Kent County Council will work with the two communities, including engaging parish and town councils and users and their families. Each neighbourhood has different local schemes which will be involved, namely: Our Place in Wye and Hinxhill, Big Local and Ageless Thanet in Newington and Village SOS in both areas. Individuals employing private sector care and local service providers will also be consulted and engaged throughout the process. External advisors include Department for Communities and Local Government and co-operative development bodies e.g. Cooperatives UK, Principle Six or Mutual Advantage. ACTIVITIES Activities are split into 2 areas: The community co-production process being conducted differently and the new community owned enterprise’s impact. Analyse, develop, plan, implement and review a social co-operative in Wye and Hinxhill and Newington. IMPACTS OUTCOMES OUTPUTS Develop a business plan for the roll out of a social co-operative scheme to more neighbourhoods in Kent, based upon the evidence and lessons identified. USER COMMUNITY FINANCIAL SOCIAL CARE SERVICES EMPLOYMENT No. users entering care system Community involvement in the development of care Cost of care Choice in care # users managing their own care # community involvement in the delivery of care # business income # appropriateness of care $ tradition provision # user’s wellbeing and situation # community responsibility of care # community outcomes $ demand $ cost of care # effectiveness of care # volunteers networks # staff retained Investment in staff No. of people trained No. of people recruited Delivering Differently in Neighbourhoods COMMISSIONING PROCESS THEORY OF CHANGE Support individuals’, carers’ and communities’ resilience within Adult Social Care – Supporting people to support themselves and others ‘As Is’ Develop commissioning strategy to identify commissioning priorities for the portfolio Develop project plan ANALYSE Review effectiveness of current service including seeking service user feedback ‘As Is’ Assumptions Pick Location Location chosen is based upon need / gap in provision Familiarisation with location & history Data is available Identify KCC support, resources & timeframe KCC support will not change during the process KCC support is adequate KCC timeframes are realistic Engage community activists, other statutory community and voluntary sector bodies Agreement to be involved Capacity to be involved Remain engaged Make formalised contact with the community Contact is adequate and appropriate Formal co-design group created Remain engaged Communications strategy developed and implemented Communication is adequate and appropriate Viable models identified Data is available Best practice exists and is identified Model options appraisal Robust method implemented Correct stakeholders are involved Preferred model identified Community has capability and capacity to implement Preferred model is the most appropriate & will make the most impact Model accepted by the community Outputs, outcomes and impacts identified Outputs, outcomes and impact are the most appropriate and SMART There is a counterfactual needed PLAN Baseline data collection Engage service users to seek their views their needs, how best to them and how to manage demand Agree success criteria and expected outcomes Confirm resources available Consider EqIA of proposed service Develop commissioning plan including assessing options for how to meet the identified needs Lead the development of effective outcome-based specifications Co-produced business plan developed Legal responsibilities understood and fulfilled There is support to write a comprehensive business plan Training within co-design group identified to implement model DO Baseline cost of current service ‘To Be’ Develop strong relationships with prospective and selected providers Prepare for contract mobilisation including how the contract will be managed Carry out initial contract review Lead on getting necessary approvals for contract award Model implemented Funding is available Funding is secured Consider current and future legislation Complete diagnostic report (including needs analysis) Develop clear summary of outcomes to be achieved through the commissioning exercise PROCESS EVALUATION QUESTIONS What is the current social care provision like now? Why do you want it to be delivered differently? 2) How was the new model delivered? How did it vary from previous social care commissioning? 3) Was the model implemented in the way it had been planned? 4) What did participants and staff feel worked well / less well in delivering the model, why and how? What, therefore, might act as facilitators and barriers to desired impacts? How can barriers be overcome and facilitators harnessed? 6) How might the model be refined or improved? 1) 5) Delivering Differently in Neighbourhoods Support individuals’, carers’ and communities’ resilience within Adult Social Care – Supporting people to support themselves and others If possible all measures to be collected quarterly (starting 3 years prior to project) USER OUTPUTS No. users entering care system No. users provided with care and support No. users entering care system Due to unavailable population figures at this level % of users has not been included as a measure Data from Swift – does it include private social care? OUTCOMES # users managing their own care No. users managing their own care – Self Funders No. users managing their own care – Direct Payments Data from Swift % of users managing their own care – Self Funders % of users managing their own care – Direct Payments IMPACTS # user’s wellbeing and situation Warwick-Edinburgh Mental Wellbeing Scale (7 Item Scale): Users wellbeing http://www2.warwick.ac.uk/fac/med/research/platfo rm/wemwbs/swemwbs_7_item.pdf http://www2.warwick.ac.uk/fac/med/research/platfo rm/wemwbs/ Delivering Differently in Neighbourhoods Support individuals’, carers’ and communities’ resilience within Adult Social Care – Supporting people to support themselves and others If possible all measures to be collected quarterly (starting 3 years prior to project) COMMUNITY OUTPUTS Community involvement in the development of care 1. I can make a positive difference to the social care provision within the community around me 2. I consider myself involved in the community Start and finish of co-design and development: (1 Strongly agree, 2 Agree, 3 Neutral, 4 Disagree, 5 Strongly Disagree) 3. I have been able to shape the provision of social care within the community around me OUTCOMES # community involvement in the delivery of care 1. I can make a positive difference (to the social care provision) within the community around me Start (question 3 only) and finish of delivery: 2. I consider myself involved in the community (1 Strongly agree, 2 Agree, 3 Neutral, 4 Disagree, 5 Strongly Disagree) 3. I am involved in the delivery* of social care within the community around me * Insert specific initiative activity # community responsibility of care & # community outcomes IMPACTS 1. I can make a positive difference (to the social care provision) within the community around me 2. I consider myself involved in the community Start (question 3 only) and finish of delivery: (1 Strongly agree, 2 Agree, 3 Neutral, 4 Disagree, 5 Strongly Disagree) *Insert specific initiative activity 3. I feel that the social care provision* is accountable to community around me No. of community outcomes* met Community outcomes need to be defined once what is being delivered is finalised Delivering Differently in Neighbourhoods Support individuals’, carers’ and communities’ resilience within Adult Social Care – Supporting people to support themselves and others If possible all measures to be collected quarterly (starting 3 years prior to project) FINANCIAL OUTPUTS Cost of care Cost of social care – Self funders Cost of social care – Direct Payments Cost of social care – Other Data from Swift Cost of social care – No. of users OUTCOMES # business income Income generated* *Dependent on specific initiative $ Demand & $ cost of care IMPACTS No. users provided with care and support No. users entering care system No. of hospital admissions No. of Emergency Admissions - primary reasons for admission to hospital Using the counterfactual area as a comparison the number of prevented / delayed / avoidable can be calculated Using the New Economy Manchester Unit Cost database costs prevented can be calculated No. of hospital admissions from Public Health (in a given age range?) Delivering Differently in Neighbourhoods Support individuals’, carers’ and communities’ resilience within Adult Social Care – Supporting people to support themselves and others If possible all measures to be collected quarterly (starting 3 years prior to project) SOCIAL CARE SERVICES OUTPUTS Choice in care No. of users of the initiative Collected by the initiative OUTCOMES # appropriateness of care 1. Overall how satisfied or dissatisfied are you with the care and support services you receive?* (Extremely satisfied, very satisfied, quite satisfied, nether satisfied or dissatisfied, quite dissatisfied, very dissatisfied, extremely dissatisfied) *Ask the users at an appropriate time frame dependent to specific initiative User satisfaction in this instance is being used as a proxy to appropriateness Question taken from ‘Personal Social Services Adult Social Care Survey’ (Question 1) http://www.hscic.gov.uk/catalogue/PUB16162/pss-ascseng-1314-fin-rpt.pdf Inappropriate A&E referrals (attendances at A&E for injuries/illnesses that could have been handled elsewhere) Compare this score with Kent ASCOF scoring http://www.hscic.gov.uk/catalogue/PUB16162/pss-ascseng-1314-fin-annx.xlsx # effectiveness of care IMPACTS No. users provided with care and support Using the counterfactual area as a comparison the number of prevented / delayed / avoidable can be calculated No. users entering care system No. of hospital admissions Emergency Admissions - primary reasons for admission to hospital Re-attendances at A&E Using the New Economy Manchester Unit Cost database costs prevented can be calculated No. of hospital admissions from Public Health (in a given age range?) Emergency admissions - elective data would be useful here as a comparative Delivering Differently in Neighbourhoods Support individuals’, carers’ and communities’ resilience within Adult Social Care – Supporting people to support themselves and others If possible all measures to be collected quarterly (starting 3 years prior to project) EMPLOYMENT OUTPUTS Investment in staff & No. of people trained & No. of people recruited No. local people / volunteers active within the initiative No. local people / volunteers trained as a result of the initiative* This output does not need to be measured for the counterfactual * The type of training depends on the specific initiative OUTCOMES $ traditional provision No. users provided with care and support No. of users of the initiative This outcome does not need to be measured for the counterfactual Calculate proportion of users of the initiative over users provided with care and support IMPACTS # volunteers networks & # staff retained No. of local people retained No. of volunteers retained This impact does not need to be measured for the counterfactual