View/Open - National Acoustic Laboratories
advertisement

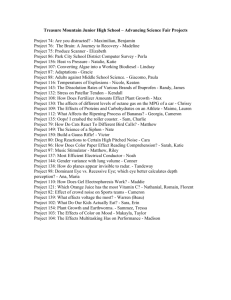
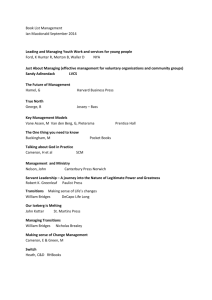
Cameron et al – SPD Indigenous Children 1 Prevalence and Remediation of Spatial Processing Disorder (SPD) in Indigenous Children in Regional Australia Sharon Cameron a Harvey Dillon a Helen Glyde a Sujita Kanthan a Anna Kania a a National Acoustic Laboratories KEY WORDS: spatial processing disorder; chronic otitis media; deficit-specific auditory training. Abbreviations: 4FAHL ACMS AEO CANS CAPD COM GLM HRTF Leq LIFE LiSN-S NAL-RP PGA SNR SPD SRT Four-frequency average hearing level Aboriginal Corporation Medical Service Aboriginal Education Officer Central auditory nervous system Central auditory processing disorder Chronic otitis media General linear model Head-related transfer function Equivalent continuous sound pressure level Listening Inventory for Education Listening in Spatialized Noise – Sentences Test National Acoustic Laboratories – Revised Profound Prescribed gain amplifier Signal-to-noise ratio Spatial processing disorder Speech reception threshold Corresponding Author: Sharon Cameron, PhD Senior Research Scientist National Acoustic Laboratories Australian Hearing Hub 16 University Avenue Macquarie University NSW 2109 Australia Phone: +61 2 9412 6851 Fax: +61 2 9412 6769 e-mail: Sharon.Cameron@nal.gov.au Cameron et al – SPD Indigenous Children 2 Objective: This study aimed to determine the prevalence of spatial processing disorder (SPD) in the Indigenous Australian population and the benefit of and logistical issues arising from remediation of the disorder. Design: Participants were assessed for SPD with the Listening in Spatialized Noise – Sentences test (LiSN-S). Participants diagnosed with SPD were instructed to use the LiSN & Learn auditory training software until 100 games had been completed. Study Sample: Participants were 144 Indigenous Australian children (aged between 6;0 [years;months] and 12;2). Results: Ten participants (6.9 per cent) presented with SPD. Nine took part in the auditory training study. Post-training LiSN-S performance improved on average by 0.9 population standard deviations (1.4 dB). There was a significant correlation (r = 0.71, p = 0.031, η2 = 0.51) between total number of LiSN & Learn games played (mean = 65, SD = 27) and improvement in LiSN-S performance. Teachers rated all participants as improving in their listening abilities post-intervention. Conclusions: There is a high prevalence of SPD in the Indigenous Australian population. LiSN & Learn training is effective in remediating SPD in this population and is considered a beneficial intervention by teachers, however improvement in spatial processing is dependent on training program uptake. Cameron et al – SPD Indigenous Children 3 Spatial processing disorder (SPD) is a specific form of central auditory processing disorder (CAPD) which is characterized by a deficit in the ability to utilize binaural cues to achieve spatial release from masking. The functional manifestation of SPD is an inability to understand speech when background noise is present. SPD can occur in children and adults with normal hearing thresholds (Cameron & Dillon 2008, 2011, in press; Cameron et al, 2012) as well as children and adults with mild to moderately-severe hearing impairment (Glyde et al, 2011, 2013) and other clinical groups (Rance et al, 2012 a & b). For those with normal hearing thresholds, SPD is thought to result from an inability to differentiate the differences in the time and intensity of auditory signals arriving at the two ears from various locations in the environment (Cameron et al., 2012). As a result, children diagnosed with SPD need a significantly greater signal-to-noise ratio (SNR) in the classroom in order to achieve the same speech reception thresholds (SRTs) as normally-hearing children without the disorder. SPD can be diagnosed with the Listening in Spatialized Noise – Sentence test (LiSN-S, Cameron & Dillon, 2009). The LiSN-S is an adaptive, virtual-reality test that measures the ability of people to use the spatial cues that normally help differentiate a target talker from distracting speech sounds (Figure 1). The LiSN-S target sentences and distracter speech materials have been synthesized with head-related transfer functions (HRTFs) to create a virtual auditory reality effect (Cameron et al, 2009, Cameron & Dillon, 2007). A diagnosis of SPD is characterized by a pattern of depressed scores on the spatially separated conditions of the LiSN-S compared to the co-located conditions (Cameron & Dillon, 2011). One-sided critical difference scores (required to determine whether an individual has improved on the LiSN-S following remediation) are available for children and adults aged 6 to 60 years Cameron et al – SPD Indigenous Children 4 (Brown et al. 2010; Cameron et al, 2011). In order for the LiSN-S to be used with the hearing-impaired population the software was modified to incorporate a prescribed gain amplifier (LiSN-S PGA) that amplifies and shapes the target and distracting stimuli according to the National Acoustic Laboratories – Revised Profound (NAL-RP) prescription (Glyde et al, 2013). SPD has been shown to be reversible in normal-hearing children with deficit-specific auditory training software (Cameron & Dillon, 2012). The LiSN & Learn software, which was developed specifically to remediate SPD, produces a virtual reality auditory environment under headphones and is designed to be used in the home. Full details of the LiSN & Learn development can be found in Cameron & Dillon, 2011. In summary, the child’s task is to identify a word or words from a target sentence by selecting a matching image on the computer screen. The target sentences are presented in spatially separated background noise. The test configuration is the same as the LiSN-S Same Voice ±90° condition (see “same voice/different directions” box in Figure 1). This configuration maximizes reliance on use of spatial processing cues to differentiate the target from the distracters. A weighted up-down adaptive procedure is used to adjust the signal level of the target based on the child’s response. The child plays two games per day, five days a week (taking approximately 15 minutes per day) until at least 100 games have been completed. In a preliminary study (Cameron & Dillon, 2011), nine children who were diagnosed with the LiSN-S as having SPD trained with the LiSN & Learn software. All the children were within normal limits on the LiSN-S post training, improving significantly on the conditions of the LiSN-S which measure spatial processing (p ranging from < 0.003 to 0.0001). Further, in a randomized, blinded, controlled study, Cameron et al (2012) found that the improvement in spatial processing following training was specific to the LiSN & Learn software. In both studies, the Cameron et al – SPD Indigenous Children 5 participants’ SRTs on the LiSN & Learn improved by approximately 10 dB over the course of the training. Improvements on behavioural tests were in line with self-report, parent and teacher ratings of listening ability post training. For a comprehensive review see Cameron and Dillon (in press). The prevalence of CAPD is said to be 2 – 3% (Chermak & Musiek, 1997). However, the exact proportion of individuals with SPD in the general population is unknown. In an evaluation report on a trial to assess and remediate CAPD conducted by Australian Hearing between April 2012 and February 2013, it was reported that 19 per cent of children (69 of 359) referred for assessment due to reported listening difficulties, presented with SPD as diagnosed with the LiSN-S (unpublished report by Australian Hearing). Further, Dillon et al (2012) reported that 17.5 per cent of children (32 of 183) referred for assessment for CAPD in various studies at the National Acoustic Laboratories have been diagnosed with SPD. Approximately 50 per cent of the children in these studies presented with a history of chronic otitis media (COM). Kapadia et al. (2012) found significantly poorer spatial processing ability (p = 0.012), as measured by the LiSN-S, in a group of 17 six year old children with a history otitis media with effusion requiring ventilation tubes. It may be hypothesized that fluctuating access to normal binaural cues during bouts of COM may negatively influence the development of spatial processing mechanisms within the central auditory nervous system (CANS). To this end, the conductive hearing loss caused by otitis media decreases the inter-aural cues present in the two cochlea, so the CANS is unable to develop the processing mechanisms that enable these cues to be used in understanding speech in noisy places (Cameron & Dillon, in press). That is, the deprivation may lead to a reduction in the number of synapses available to assist in binaural interaction. It is possible Cameron et al – SPD Indigenous Children 6 that for a proportion of these children, the processing mechanisms do not develop normally even after hearing sensitivity returns to normal. Indigenous Australian children have higher rates of middle ear disease than have been described in any other population in the world. Estimates suggest that Aboriginal children in Australia experience, on average, 2.6 years of conductive hearing loss. The equivalent figure for non-Aboriginal children is three months (OATSIH, 2001). Studies conducted over the years in regional areas of Australia have reported prevalence rates of middle ear abnormalities in Indigenous children to be between 45-62% (Adams et al, 2004; Thorne, 2003). Given the high prevalence of middle ear disease in Indigenous communities, and the aforementioned link between an early history of COM and SPD, it is expected that the prevalence of SPD will be higher in the Indigenous population compared to the nonIndigenous population. The presence of SPD would contribute to listening difficulties in the classroom and may limit the educational progress of Aboriginal children with the disorder. Many of these children would have additional disadvantages arising from listening in their second language (Nicholls, 2005), poor acoustics in the classroom (Massie et al., 2004), and comorbid conductive hearing loss arising from current or past middle ear disorders (Thorne, 2003). Despite the negative impact that SPD could have on educational outcomes for Indigenous Australian children there is currently no funding to cover services for children with CAPD. The focus of this research was to examine the prevalence of SPD in a sample Indigenous Australian population. The pilot study additionally aimed to determine the benefit of auditory training in the school setting in Indigenous Australian children diagnosed with SPD Cameron et al – SPD Indigenous Children 7 and to identify any logistical issues that would need to be resolved if a national program to diagnose and remediate this disorder were to be mounted. Methods Approval for the study discussed in this paper was granted from the Australian Hearing Human Research Ethics Committee, as well as the Student Engagement and Program Evaluation Bureau of the NSW Department of Education and Communities. Additional approvals were obtained from the NSW Aboriginal Education Consultative Group (Lower North Coast Region) and the Durri Aboriginal Corporate Medical Service. Participants Data was collected from a total of 144 children aged between 6;0 [years;months] and 12;2 (mean age 8;10). There were 69 males and 75 females. Participants were recruited from four government primary schools in Kempsey, NSW, being Kempsey East public school, Kempsey West public school, Kempsey South public school and Green Hill public school. In addition to the 144 children who took part in the study, a total of 13 children met the study exclusion criteria, as follows: 1. Children with a diagnosed intellectual disability or with documented unmedicated attention deficit or hyperactivity disorder (ADHD) were excluded from the study due to the impact of such conditions on the validity of diagnostic test results as well as on a child’s ability to undertake daily auditory training. Six children were excluded based on these criteria. 2. On the day of testing the children underwent a formal hearing assessment, including direct diagnostic otoscopy, tympanometry and pure tone audiometry. If otoscopic Cameron et al – SPD Indigenous Children 8 examination revealed ear discharge the child was excluded from the study and referred for appropriate medical advice. Two children failed the otoscopic examination. 3. Where hearing thresholds exceeded normal limits (>20 dB at 500 Hz, 1, 2 or 4 kHz), unmasked and masked bone conduction was undertaken to determine the nature of the hearing loss. Four children with a sensorineural hearing loss were excluded from the study. 4. Children with a conductive loss were excluded if they had a four-frequency average hearing level (4FAHL) ≥ 40 dB and/or the 4FAHL between the two ears by more than 20 dB to ensure adequate amplification during testing and LiSN & Learn training. One child with a 4FAHL which differed between the ears by more than 20 dB was excluded. Procedures: Pre- and Post-Training The audiological measurements and the LiSN-S test were administered by three members of the research team. Testing took approximately 30 minutes per child. Testing was carried out in a quiet room, such as the school library, in the participating schools between 9 am and 3 pm. The LiSN-S is designed to be delivered in a sound-attenuated environment, such as an audiological test booth. As such, maximum permissible noise levels for this test were determined at each frequency (500 Hz, 1, 2, 4, 8 kHz). To ensure that these levels were not exceeded the equivalent continuous sound pressure level (Leq) in dB at each school was measured using a Brüel & Kjær type 2231 sound level meter. Measurements were taken prior to each LiSN-S test session and if intermittent fluctuations in noise levels occurred, such as if heavy vehicles passed outside. In such cases testing was suspended until acceptable noise levels were recorded. The procedure used, prior to testing, to calculate the LiSN-S permissible noise levels is detailed in Appendix A. Cameron et al – SPD Indigenous Children 9 Children who were diagnosed as having SPD were re-tested on the audiological measures and LiSN-S post-training. Test-retest reliability on the LiSN-S measures ranged from r = 0.2 for the spatial advantage measure to r = 0.7 for high cue SRT measure, with mean test-retest differences ranging from a maximum of 0.7 dB on the high cue SRT to only 0.1 dB on the total advantage measure (Cameron et al, 2011). Following training, teachers of the children with SPD were requested to complete the Listening Inventory for Education (LIFE) – ‘Teacher Appraisal of Listening Difficulty’ questionnaire (Anderson & Smaldino, 1998) and to forward these to the research audiologist. AUDIOLOGICAL TESTING Following otoscopic examination, audiometric and tympanometry evaluation was undertaken using an Interacoustics® AA222 Audiotraveller diagnostic audiometer/impedance meter. The transducers used for pure tone audiometry were E-A-RTone® 3A insert earphones (unless contraindicated) in combination with MSA Left/Right™ 766243 headband earmuffs, size “high” (yellow cup) in order to provide greater attenuation of ambient noise. Peltor H7A supra-aural earphones were used for participants with contraindications, such as large tympanic membrane perforations or ventilation tubes. Audiometry was conducted using 20 dB HL screening levels at 500 to 4000 Hz. For participants who did not pass the screening cut-off, both air and bone conduction thresholds were obtained. LiSN-S The LiSN-S was administered using a personal computer and Sennheiser HD215 circumaural headphones. The headphones were connected to the headphone socket of the PC via a Buddy 6G USB soundcard. The sensitivity of the soundcard was automatically set to a predetermined level by the LiSN-S software in order to achieve pre-designated signal levels, Cameron et al – SPD Indigenous Children 10 alleviating the need for daily calibration (Cameron et al, 2009). At this pre-set level, the combined distracters at 0° had a long-term root mean square (RMS) level of 55 dB SPL as measured in a Brüel and Kjær type 4153 artificial ear attached to a Brüel and Kjær sound level meter, model 2231. The LiSN-S software creates a virtual reality auditory environment under headphones by pre-synthesizing the speech stimuli with HRTFs. Target sentences are perceived as coming from directly in front of the listener (0° azimuth). The distracter speech, in the form of looped children’s stories, varies according to either their perceived spatial location (0° vs + and -90° azimuth), the vocal identity of the speaker/s of the stories (same as, or different from, the speaker of the target sentences), or both these parameters. The target sentences are initially presented at a level of 62 dB SPL. The distracter stories are presented at a constant level of 55 dB SPL (for the combined level of the two competing talkers). The target and competing signals are presented to both ears simultaneously. The listener’s task was to repeat back to the examiner the words heard in each target sentence. If the participant made a grammatical mistake that was considered to be a cultural norm (such as sawed for seen) the word was scored as correct. Up to 30 sentences were presented in each of the four conditions of distracter location and voice: same voice at 0º, same voice at ±90º, different voices at 0º and different voices at ±90º. The SNR was adjusted adaptively in each condition by varying the target level. The adaptive procedure is performed automatically by the software when the examiner enters the number of words in each sentence that is correctly identified by the participant. The SNR was decreased by 2 dB if a listener scored more than 50 per cent of words in a sentence correct, and increased by 2 dB if he or she scored less than 50 per cent of words correct. The SNR was not adjusted if a response of exactly 50 per cent correct was recorded (for example, 3 out of 6 words correctly identified). A minimum of five sentences were provided as practice, however, practice Cameron et al – SPD Indigenous Children 11 continued until one upward reversal in performance (i.e., the sentence score dropped below 50 per cent of words correct) was recorded. Testing ceased in a particular condition when the listener had either (i) completed the entire 30 sentences in any one condition; or (ii) completed the practice sentences plus a minimum of a further 17 scored sentences, and their standard error, calculated automatically in real time over the scored sentences, was less than 1 dB. A participant’s speech reception threshold was calculated in each condition as the average SNR recorded for the scored sentences. The procedure takes approximately 15-20 min to complete. As shown in Figure 1, performance on the LiSN-S is evaluated on the same voice 0° condition (low cue SRT); the different voices ±90° condition (high cue SRT), as well as on three difference scores - talker, spatial and total advantage. These advantage measures represent the benefit in decibels (dB) gained when talker (pitch), spatial, or both talker and spatial cues are incorporated in the maskers, compared to the baseline (low cue SRT) condition where no talker or spatial cues are present in the maskers. As previously mentioned, SPD is characterized by a pattern of depressed scores on the spatially separated conditions of the LiSN-S compared to the co-located conditions. In this study a participant was diagnosed as having SPD if his or her LiSN-S pattern score was more than 1.96 population standard deviations below the mean. An individual’s pattern score, which is calculated automatically by the LiSN-S software, is a measure of the benefit, in decibels, of adding spatial information, averaged across the conditions where no talker cues are available and the condition where there are talker cues available. The formula used to derive the pattern measure is described in Cameron and Dillon (2011). Cameron et al – SPD Indigenous Children 12 LiSN-S PGA Children with mild conductive losses as described in the Participants section were assessed with the LiSN-S in prescribed gain amplifier mode. The participant’s right and left ear air and bone conduction thresholds were entered and, as discussed in the introduction, the software amplified and shaped the LiSN-S stimuli according to the child’s NAL-RP prescription (Glyde et al, 2013). LIFE QUESTIONNAIRE The Listening Inventory for Education - Teacher Appraisal of Listening Difficulty (LIFE) is a measure of improvement in listening ability following intervention. The LIFE has been a widely used efficacy tool for more than ten years (Anderson, Smaldino, & Spangler, 2011). The questionnaire is comprised of 16 items, each describing an educational situation. For example, item 4 asks: Attention has improved when listening to directions presented to whole class. Item 16 originally read: Based on my knowledge and observations I believe that the amplification system is beneficial to the student’s overall attention. The words amplification system were changed to auditory training software for the present study. A five-point response scale is used from +2 (Agree) to -2 (Disagree). All items are added together to produce a composite score on an incremental scale from -35 to +35. A score of 35 represents strong positive change indicating that the intervention was highly beneficial. A score of 0 represents no change, and -35 suggests the intervention was highly unfavourable. Procedures: Training LiSN & LEARN Children who were diagnosed as having SPD undertook auditory training with the LiSN & Learn. Training took place in a quiet room in the school, such as the library, using a school Cameron et al – SPD Indigenous Children 13 computer and was carried out under the supervision of the participant’s school teacher or Aboriginal Education Officer (AEO). The software was installed by the research audiologist, who demonstrated the training program to the participant and his or her supervisor. All the semantic items used in the development of the LiSN & Learn target sentences are acquired by children aged 30 months of age (Cameron & Dillon, 2011). However, as English may not be the first language of the Indigenous Australian children a word and picture flash cards were used to familiarize the children with the LiSN & Learn target words to ensure that language factors did not inhibit program usability (National Acoustic Laboratories, 2013). The LiSN & Learn stimuli (target words and distracter stories) are presented through Sennheiser HD215 headphones. Calibration is undertaken at start up using a reference signal (whooshing sound; speech-shaped random noise) that is adjusted by the child using a slider bar. The child is instructed to move the slider bar until he or she can barely hear the whooshing sound. The reference signal is level normalized so that its rms level is 40 dB less than the rms level of the combined distracters stories. Thus, when presented, the sensation level of the combined distracters is at least 40 dB SL. A starting level of 7 dB SNR is utilized. The children were instructed to play two games per day, five days per week for 50 training sessions (i.e. until 100 games have been played). Training took approximately 15 minutes per day. Five training games were used - Listening House, Listening Ladder, Answer Alley, Goal Game and Space Maze. The first four games differ only in respect to the animations (e.g., the game is set in a bowling alley in Answer Alley and a soccer field for Goal Game) and the auditory stimuli used to provide feedback and positive reinforcement. The target and distracter stimuli and the response protocol are identical for all games. In all games the child’s task was to identify a word from a target sentence presented in background noise consisting of two looped distracter stories. The target sentences emanated from 0° azimuth Cameron et al – SPD Indigenous Children 14 and the distracter stories emanated from + and - 90º azimuth. All speech stimuli are produced by the same female speaker so the listener must predominantly rely on processing of spatial cues to separate the target sentence from the distracter speech. A tone burst is presented before each sentence to alert the child that a sentence will be presented. Immediately following the presentation of the sentence four images and a question mark appear at the top of the screen (Figure 2). In a five-alternative, forced-choice, adaptive method, the child uses the computer mouse to select one of the images that matches a word from the sentence he or she had just heard (or make an unsure response by selecting an image of a question mark). A weighted up-down adaptive procedure is used to adjust the signal level of the target based on the participant’s response. The target is decreased by 1.5 dB when the child correctly identifies a target image. It is increased by 2.5 dB if the wrong target is identified, and it is increased by 1.5 dB if an unsure (question mark) response is made. If the child selects the unsure response for a particular sentence, that sentence is repeated at the higher SNR. However if the child selects the unsure response again for that same sentence, a different sentence is presented at a higher SNR. If the child selects a correct image, a short congratulatory sound is presented (such as a bell). If the child selects an incorrect or unsure image a short negative sound is presented (such as a buzzer). Different sounds and animations are used as feedback for each of the four games. In the Space Maze game the child hears an instruction (e.g., move up three spaces) and must use the computer mouse to select a direction (up, down, left, right) and a number (from one to ten) in order to move around the maze. The direction and number buttons remain on the screen throughout the game. A minimum of five sentences is provided as practice; however practice continues until one upward reversal in performance (that is, the first incorrect or unsure response that occurs after Cameron et al – SPD Indigenous Children 15 a correct response) has been recorded. The SNR decreases in 3 dB steps during the practice period. There are 40 sentences in any game. The child’s SRT for each game is measured as the average SNR over all sentences, excluding the practice. Feedback regarding the child’s performance during the game, positive reinforcement for correct responses and progress indicators are incorporated into the software. Further, a personalized avatar or “buddy” that the child designs on install provides positive feedback throughout the training sessions. Players earn “currency” for completing games which can be used to purchase items for their buddy in the LiSN & Learn reward shop or to play nontraining games that are incorporated in the software. In addition to the intrinsic rewards built into the LiSN & Learn software, over the course of the training participants were offered small, culturally-appropriate rewards (including stationery such as pencils and stickers for reaching training milestones, and laminated certificates) as an incentive to continue with and to complete training. Results were recorded automatically by the software. Progress reports in the form of an Excel spread sheet were generated by selecting the report generation button in the progress report area. The participants’ teacher or the AEO were required to email these reports to the research audiologist on a weekly basis. The research audiologist checked the reports each week to ensure that the child was using the software as required by the study protocols. The four participating schools were allocated a five-month period in which to complete the ten-week training program, ranging from the start of the second NSW public school term on 23 April 2012 to the end of the third school term on 21 September 2012. Results Cameron et al – SPD Indigenous Children 16 Analyses were performed with Statistica 10.1. Prevalence of SPD Fifteen of the 144 participants, or 10.4 per cent of the study sample, presented with a mild conductive hearing loss (>20 dB at 500 Hz, 1, 2 or 4 kHz and 4FAHL < 40 dB). Performance on the LiSN-S - as determined by each participant’s pattern measure expressed as a Z-score was normally distributed as determined by the Shapiro-Wilk test of normality (p = 0.232). However, as shown in Figure 3, performance was negatively skewed, presumably due to the high incidence of COM in the Indigenous Australian population. Ten participants, or 6.9 per cent of the study sample, presented with a spatial processing disorder (SPD) as determined by his or her LiSN-S pattern score. Of the ten children with SPD, four had a mild conductive hearing loss. Nine of the ten children with SPD (four males and five females) went on to train with the LiSN & Learn. The other child withdrew from the study as he was not willing to undertake the training. Details of the hearing thresholds and middle ear function pre- and post-training of the nine children who undertook the LiSN & Learn remediation are presented in Table 1. Results of LiSN & Learn Training Figure 4 shows the individual participant improvement in SRT in dB on the LiSN & Learn over time (expressed as a five-day running average) for the nine children who took part in the training study. None of the children completed the entire training program of 100 games. On average the participants played 65 games (SD 27) with a range of 25 to 98 games. It can be seen in Figure 4 that some participants showed a dip in performance during training. The student learning support officer supervising the training of participants 518, 523 and 524 Cameron et al – SPD Indigenous Children 17 advised that ear infections were suspected during this period. Upon further inspection it was noted that the children were not undertaking the calibration procedure (i.e. they were moving the slider bar to the same spot without listening to the calibration tone). The supervisor instructed these participants to “blow their noses” before each test to attempt to equalize the pressure in their middle ear cavities and also assisted in the calibration process. This resulted in the return to more linear improvement in SRT on the LiSN & Learn as shown in the graph. The pre- and post-training LiSN-S pattern Z-scores for each participant - together with number of games played and LIFE teacher ratings - are documented in Table 2. The mean pre-training LiSN-S pattern Z-score was -2.6 population SD units from the mean (SD = 0.4). There was a trend of improvement on the LiSN-S post training, with the mean LiSN-S Zscore improving to -1.7 (SD = 2.4), as shown in Figure 5. Repeated measures Analysis of Variance (ANOVA) with number of games played as a continuous predictor showed that there was no significant difference between pre- and post-training performance (F (1, 7) = 3.80, p = 0.092, η2 = 0.35). There was, however, a significant interaction between degree of improvement and number of LiSN & Learn games completed (F (1, 7) = 7.19, p = 0.031, η2 = 0.51). The correlation between performance improvement and games played was r = 0.71. Thus children who played more games on the LiSN & Learn improved more on the LiSN-S, as shown in Figure 6. Group performance on the various LiSN-S SRT and advantage measures pre- and posttraining is illustrated in Figure 7. Mean scores were calculated from the individual standard scores (or Z-scores) for each of the nine participants in the LiSN & Learn study. Performance improved post-training in every LiSN-S condition except for talker advantage, however, as evidenced by the error bars representing the 95 per cent confidence intervals, there was more Cameron et al – SPD Indigenous Children 18 variation post-training. This degree of variation is consistent with the interaction of amount of training on LiSN-S performance described above. Thus whereas repeated measures ANOVA showed that the effect of training was significant when averaged across all measures (F (1, 8) = 10.34, p = 0.012, η2 = 0.56), Tukey HSD post-hoc multiple comparison test revealed that post-training improvement of 1.2 population SDs (4.0 dB) was significant only for the high cue SRT condition (p = 0.027). High cue SRT is the LiSN-S condition that is most similar to real-life listening in that the distracters are spatially separated and distracter voices are different to that of the target speaker. The degree of improvement in the high cue SRT condition is partly due to an improvement in some ability in the participants (such as auditory vigilance) that applies even when there is no spatial separation, as evidenced by the improvement in the low cue condition of 1.9 population SDs (2.8 dB), as well as improvement in spatial processing ability. Post-Training Teacher Ratings of Listening Ability The individual participant LIFE –Teacher Appraisal of Listening Difficulty questionnaire results are provided in Table 2. As described in the methods section, the LIFE is a measure of real-world improvement in listening ability following some form of intervention, in this case LiSN & Learn auditory training for SPD, on a scale of -35 to +35. The mean rating was +24 (SD 10). However there was no significant correlation (r = -0.10) between the teacher ratings and the participants’ post-training improvement in LiSN-S pattern Z-score (F (1, 7) = 0.07, p = 0.797, η2 = 0.06) or improvement in high cue SRT Z-scores (F (1, 7) = 0.03, p = 0.867, η2 = 0.00). In order to investigate the study aims of determining the benefit of auditory training in the Indigenous Australian population and identify any logistic issues that may impact a national Cameron et al – SPD Indigenous Children 19 program to identify and remediate SPD, school principals, class teachers and the teachers/support staff who supervised the LiSN & Learn training were asked to provide qualitative feedback on the progress of the LiSN & Learn training. These details are provided in Appendix B. The qualitative feedback was obtained during and after training, and before reassessment on the LiSN-S. To protect participant confidentiality, ID numbers have been removed from these comments and number of games played is noted as a range (< 50 or > 50). Post-training performance on the LiSN-S is noted as “pass” or “fail” based on the LiSN-S pattern score. Discussion The initial aim of this study was to investigate the prevalence of SPD in the Indigenous Australian population. As reported in Dillon et al (2012) children with SPD commonly present with a history of chronic otitis media, and the incidence of COM is particularly high in the Indigenous Australian population. The prevalence of SPD in the study sample of 144 children drawn randomly from the Indigenous population in a regional town was indeed high at 6.9 per cent. The second objective of the study was to determine whether the benefits of auditory training with the LiSN & Learn software for non-indigenous children with SPD reported by Cameron & Dillon (2011) and Cameron et al (2012) would be found in the Indigenous Australian population in this study. In the present study, improvement in spatial processing post training was measured by LiSN-S performance as well as teacher ratings of improvement in listening ability following intervention using the LIFE questionnaire. On average, post-training LiSNS performance improved by nearly one population standard deviation. However, LiSN-S performance was variable and significantly related to the number of LiSN & Learn training Cameron et al – SPD Indigenous Children 20 games played by the participant (r = 0.71, p = 0.031, η2 = 0.51). Whereas all participants were requested to complete 100 games over 50 training sessions, actual uptake ranged from 25- 98 games (mean 65 games). This was despite providing children in this study with rewards - additional to those intrinsic in the software – such as culturally-appropriate stationery and laminated certificates. All teachers rated the LiSN & Learn intervention as beneficial for their respective students. On a scale of -35 to +35, the mean LIFE rating was +24 (range +11 to +35). Interestingly, however there was no significant correlation between the teacher ratings and the participants’ post-training improvement in LiSN-S pattern Z-score (r = -0.10, p = 0.797, η2 = 0.06). An inspection of the qualitative feedback from teachers provided in Appendix B showed that even for children who completed less than half the required number of training games and whose LiSN-S performance was not within normal limits post-training, teachers felt that the training was beneficial to the child’s listening performance in the classroom. Feedback indicated that the confidence of these children had improved, as had their classroom participation. It could be hypothesized that in the early stages of training the child may learn aspects of auditory vigilance that may assist in classroom situations. This hypothesis is supported by the attentional improvements measured post LiSN & Learn training in Cameron and Dillon (2011). However, the study has confirmed that spatial processing ability improves proportionately to the number of LiSN & Learn training games completed. To this end it may be speculated that regardless of whether a child’s confidence improves as a result of undertaking training, sustained listening performance would still be impacted due to aspects of auditory fatigue that would occur if the underlying binaural processing deficit remained unremediated. Cameron et al – SPD Indigenous Children 21 In respect to specific factors that would need to be addressed should a national program be launched, an issue identified through teacher feedback was lack of compliance with training due to disinterest in the LiSN & Learn program with repeated use. Some modifications to the software to make the games more engaging would help to alleviate this problem. It was also noted that some target words required additional familiarisation following period of absence such as school holidays, for example the verbs played, skipped and hopped. These words could be highlighted on the flash cards and this issue could be noted in training packs for teachers. Limitations of the Study and Potential Solutions As noted in the results section, three children who were suspected of having ear infections were not undertaking the daily calibration procedure required to adjust LiSN & Learn output levels. The children simply set the calibration slider bar to the same level each day, rather than actually listening to, and adjusting the level of the reference tone. Thus it is probable that the output levels in the headphones were inadequate during the period of infection. In the case of these children, once the supervisor instructed these participants to “blow their noses” before each test and also assisted in the calibration process the issue resolved, and performance on the LiSN & Learn improved linearly. However, this issue highlights the fact that audiometric and immittance data at the beginning and end of the study offer only limited information on how a conductive disorder was potentially impacting the children overall and particularly during training. The calibration process could be improved by replacing the slider bar measurement with a procedure whereby the listener selects on an object on the computer screen when he or she Cameron et al – SPD Indigenous Children 22 perceives a tone. In this adaptive method, the reference signal becomes louder or softer depending on the child’s response. There is far less possibility of the child faking or ignoring the daily calibration procedure using this method. Regardless of upgrading the software to improve the calibration procedure, it is still imperative that the child’s performance is monitored daily to ensure that unexpectedly poorer results on the LiSN & Learn is not the result of a pervasive middle ear infection over the course of training, and that divergence from linear improvements is reported to the researcher or professional overseeing the training. Following confirmation of a serious ear infection the training can be suspended until the child is well enough to continue with the program. Of course, unexpectedly poor performance on the LiSN & Learn on any particular day could be due to any number of contributing factors in any population, including fatigue or distraction, although as the incidence of chronic otitis media is so prevalent in the Indigenous Australian community that researchers and professional and supervising teachers should be particularly mindful of this factor during training. Effective communication of the results and limitations of the current study to those involved in future studies or community programs with Indigenous Australian will be necessary to minimize issues such as those associated with middle ear infection on performance. Conclusion There is a high prevalence of SPD in the Indigenous Australian population. LiSN & Learn training has the potential to remediate SPD in this population and is considered a beneficial intervention by teachers, however improvement in spatial processing is dependent on compliance with the training protocols. In any future program to assess and remediate Indigenous Australian children for SPD school principals, teachers and supervisors should be Cameron et al – SPD Indigenous Children 23 provided with the results of this study in respect to the relationship between training and improvements in spatial processing ability so that realistic expectations of training outcomes are ensured and game completion encouraged. Additionally, daily monitoring of LiSN & Learn performance and calibration procedures may ensure that mild temporary hearing threshold shifts do not impact severely on day-to-day performance and overall outcomes. Acknowledgements The authors would like to acknowledge the financial support of the Commonwealth Department of Health and Ageing. The authors would also like to thank the principals, teachers and students of the schools in Kempsey NSW who participated in this study. We would also like to thank Mr Mark Seeto for assistance with statistics. Declaration of Interest: This research was funded by Australian Hearing. The authors would like to disclose that the LiSN-S test described in this paper is distributed under license by Phonak Communications AG. The LiSN & Learn auditory training software described in this article is distributed by the National Acoustic Laboratories. Financial returns from the sale of the LiSN-S and the LiSN & Learn benefit the National Acoustic Laboratories and Dr Cameron. This has in no way influenced the research reported in this article. Cameron et al – SPD Indigenous Children 24 References Adams K., Dixon T. & Guthrie J. 2004. Evaluation of the Gippsland Regional Indigenous Hearing Health Programme - January to October 2002. Health Promotion Journal of Australia, 15, 205-210. Anderson K.L., & Smaldino J.J. 1998 . Listening Inventory For Education: An Efficacy Tool- Teacher Appraisal of Listening Difficulty. Tampa, FL: Educational Audiology Association. Anderson, K.L., Smaldino, J.J. & Spangler, C. 2011. LIFE-R The Listening Inventory For Education-Revised. http://successforkidswithhearingloss.com/wpcontent/uploads/2011/09/LIFE-R-Instruction-Manual.pdf. Brown D., Cameron S., Martin J., Watson C. & Dillon H. 2010. The North American Listening in Spatialized Noise – Sentences Test (NA LiSN-S): Normative data and test-retest reliability studies for adolescents and young adults. J Am Acad Audiol, 21, 629-641. Cameron S., Brown D., Keith R., Martin J., Watson C. & Dillon H. 2009. Development of the North American Listening in Spatialized Noise - Sentences Test (NA LiSN-S): Sentence equivalence, normative data and test-retest reliability studies. J Am Acad Audiol, 20, 128-146. Cameron et al – SPD Indigenous Children Cameron S. & Dillon H. 2007. 25 Development of the Listening in Spatialized Noise - Sentences Test (LISN-S). Ear Hear, 28, 196-211. Cameron S. & Dillon H. 2008. The Listening in Spatialized Noise – Sentences Test: Comparison to prototype LISN test and results from children with either a suspected (central) auditory processing disorder or a confirmed language disorder. J Am Acad Audiol, 19, 377-391. Cameron S. & Dillon H. 2009. Listening in Spatialized Noise – Sentences test (LISN-S) (Version 2.003) [Computer software]. Murten, Switzerland: Phonak Communications AG. Cameron S. & Dillon H. 2011. Development and evaluation of the LiSN & Learn auditory training software for deficit-specific remediation of binaural processing deficits in children: Preliminary findings. J Am Acad Audiol, 22, 678-696. Cameron S. & Dillon H. 2012. LISN & Learn Auditory Training Software (Version 3.0.0) [Computer software]. Sydney, NSW: National Acoustic Laboratories. Cameron S. & Dillon H. In press. Remediation of spatial processing issues in Central Auditory Processing Disorder. In G.D. Chermak & F. E. Musiek (eds.) Handbook of Central Auditory Processing Disorder, 2nd ed. Comprehensive Intervention. Volume 2. San Diego: Plural Publishing. Cameron et al – SPD Indigenous Children 26 Cameron S., Glyde H. & Dillon H. 2011. Listening in Spatialized Noise- Sentences Test (LiSN-S): Normative and retest reliability data for adolescents and adults up to 60 years of age. J Am Acad Audiol, 22, 697-709. Cameron S., Glyde H. & Dillon H. 2012. Efficacy of the LiSN & Learn auditory training software: Randomized blinded controlled study. Audiology Research, 2:e15. Chermak, G.D., & Musiek, F.E. 1997. Central Auditory Processing Disorders: New Perspectives. San Diego: Singular Publishing Group. Dillon H., Cameron S., Glyde H., Wilson W. & Tomlin D. 2012. Opinion: Re-designing the process of assessing people suspected of having central auditory processing disorders. J Am Acad Audiol, 23, 97-105. Glyde H., Cameron S., Dillon H., Hickson L. & Seeto, M. (2013). The effects of hearing impairment and aging on spatial processing. Ear Hear, 34, 15-28. Glyde H., Hickson L., Cameron S., & Dillon H. (2011). Problems hearing in noise in older adults. Spatial processing disorder? Trends in Amplif, 15, 116-126. Kapadia, S., Godden, D., Harvey, J., Satyanarayana, N. & Morley, A. Spatial listening in children with a history of otitis media with effusion. Poster session presented at: Global Perspectives on CAPD. American Academy of Audiology Conference; 2012 March 30 – 31; Boston, MA. Cameron et al – SPD Indigenous Children 27 Massie, R., Theodoros, D., McPherson, B. & Smaldino, J. (2004). Sound-field amplification: Enhancing the classroom listening environment for Aboriginal and Torres Strait Islander children. Australian Journal of Indigenous Education, 33, 47-53. National Acoustic Laboratories. 2013. LiSN & Learn – Chart of Target Words. Retrieved from http://capd.nal.gov.au/lisn-learn-additional-resources.shtml. Nicholls, C. 2005. Death by a thousand cuts: Indigenous language bilingual education programmes in the Northern Territory of Australia, 1972-1998. International Journal of Bilingual Education and Bilingualism, 8(2-3), 160-177. OATSIH – Office for Aboriginal and Torres Strait Islander Health (2001). Burden of disease. In Systematic review of existing evidence and primary health care guidelines on the management of Otitis Media (middle ear disease) in Aboriginal and Torres Strait islander populations. Canberra, Australia: Commonwealth Department of Health and Aged Care. Rance G., Ryan M.M., Carew P., Corben L.A., Yiu E., Tan J. & Delatycki MB. 2012a. Binaural speech processing in individuals with auditory neuropathy. Neuroscience, 226, 227-235. Rance G., Corben L. & Delatycki M. 2012b. Auditory processing deficits in children with Friedreich ataxia. J Child Neurol, 27, 1197-1203. Cameron et al – SPD Indigenous Children 28 Thorne J.A. 2003. Middle ear problems in Aboriginal school children cause developmental and educational concerns. Contemp Nurse, 16, 145-150. Cameron et al – SPD Indigenous Children 29 Figure Legends Figure 1. The four subtests of the LiSN-S test, and the three difference scores (advantage measures) that can be derived from them. The target speech, T, always comes from the front, whereas the two distracter stories, D1 and D2, come from the front or the sides, in different conditions. D1 and D2 can be the same voice as T or different voices. Figure 2. Image of a LiSN & Learn training game. Figure 3. Histogram showing performance on the LiSN-S as measured by the pattern measure, expressed as a Z-score, for the 144 participants in the study. Figure 4. Individual improvement in SRT in dB on LiSN & Learn over time, expressed as a five-day running average, for each of the nine participants who took part in the auditory training study. Figure 5. Pre- and post-training performance on the LiSN-S pattern score, expressed as a Zscore, for the nine participants in the LiSN & Learn auditory training study. Error bars represent 95 per cent confidence intervals. Figure 6. Scatterplot of positive relationship between total number of LiSN & Learn games played and post-training improvement on LiSN-S as measured by the pattern Z-score. Regression bands, bounded by dotted lines, represent 95 per cent confidence intervals. Cameron et al – SPD Indigenous Children 30 Figure 7. Performance on the individual LiSN-S SRT and advantage measures pre- and postfor the nine children in the LiSN & Learn study. Performance is expressed in population standard deviation units from the mean. Error bars represent 95 per cent confidence intervals.