Form - Alberta Health Services

High Cost Drug Funding Request Form – Anti-Dementia Drugs
SUBMIT ANNUALLY FROM DATE OF INITIAL DRUG PROVISION
Note - Please select appropriate drug name: donepezil galantamine ER memantine rivastigmine
Care Centre Date (of form submission) Patient Information
Patient Code 1 Date of Birth (YYMMDD)
/ /
(YYMMDD)
/ /
Physician Information
Surname First
New Renewal NOTE: Funding may or may not be approved by Alberta Health Services, Calgary
Approved for use under the following conditions :
Protocol 1 – Alzheimer’s
Donepezil hydrochloride (5-10 mg po qd), galantamine hydrobromide ER (8 - 24 mg po qd), or rivastigmine tartrate oral(1.5 mg – 6 mg po bid), and rivastigmine transdermal patch (if intolerant to oral form) Refer to algorithm for patch dose/conversion conversion are approved for use under the following conditions:
1. The resident must have a diagnosis of Alzheimer Disease or a diagnosis of mixed dementia where Alzheimer
Disease is a significant component; AND
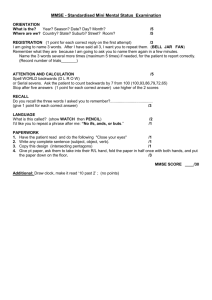
2. The resident will have a Folstein MMSE score within 12 weeks prior to or following admission of between 10 –
26 or a Cognitive Performance Scale (CPS) score between 1
– 4
AND
3. Initial reporting of BOTH an ABS (Aggressive Behavior Scale) and ADL Short (Activities of Daily Living) score is required to establish a baseline functional assessment
4. Rivastigmine patch may ONLY be supplied if there has been a documented intolerance to oral rivastigmine
Check
Condition
For Continuation of Funding
1. An annual MMSE score or a CPS is required; AND
2. Annual reporting of both an ABS (Aggressive Behavior Scale) and ADL Short (Activities of Daily Living) score
Protocol 2
– Lewy Body Disease
Rivastigmine tartrate (1.5 mg – 6 mg po bid or transdermal patch) Refer to algorithm for patch dose/conversion or donepezil hydrochloride (5-10 mg po qd) are approved for use under the following conditions (galantamine hydrobromide has not demonstrated usefulness for this disorder):
Trial of therapy for residents with a diagnosis of Lewy Body dementia where other options, such as low-dose atypical neuroleptics, have either not been tolerated or have failed to control symptoms of hallucinations and agitation associated with the disorder. Where symptoms are controlled, therapy will be long-term for ongoing management and will not require either an MMSE or a CPS score for continued funding.
Note: These individuals will not require MMSE or CPS scores to be completed.
Protocol 3
– Behavioural Disturbance in Alzheimer’s Disease
Donepezil hydrochloride (5-10 mg po qd), galantamine hydrobromide ER (8
– 24 mg po qd), rivastigmine tartrate oral(1.5 mg
– 6 mg po bid), and rivastigmine transdermal patch (if intolerant to oral form) Refer to algorithm for patch
, or memantine (10 mg po bid) are approved for use under the following conditions:
1. Behaviour mapping must be undertaken daily for 2 weeks prior to initiation of the agent and again daily for 2 weeks after initiation of the agent. Following this initial two week period, recording for 1 day every two weeks looking for beneficial effect on target behaviours and for side effects is required for 3 months; AND
2. There must be documented intolerance to or failure of at least 2 trials of 2 weeks duration with other agents specifically being used for behavioural management. These may include mood stabilizers or the following atypical anti-psychotics: risperidone, quetiapine, and olanzapine; AND
3. There must be a recommendation for use by a specialist in psychiatry, geriatrics or neurology (these will be very challenging individuals and the assumption is that a consultant will already be involved) .
4. Initial and annual reporting of both an ABS (Aggressive Behavior Scale) and ADL Short (Activities of Daily
Living) score will be required for funding
5. Rivastigmine patch may ONLY be supplied if there has been a documented intolerance to oral rivastigmine
Note: These individuals will not require MMSE or CPS scores to be completed.
Drug Dose : MMSE: /30
Date:
CPS: -/6
Date:
ABS: -/12
Date:
ADL Short: -/16
Date:
Admission Date:
/ /
Additional Information Relating to Request (i.e. frequency of follow-up with specialist, consult report information, etc.):
Physician’s or Pharmacist’s Name: Initial Drug Provision Date
(YY/MM/DD)
/ /
Processing Instructions: Pharmacy Provider email to
Supportive Living and Long Term Care at: cc.drugmanagement@albertahealthservices.ca
OR
Physician fax to: (403)943-0232
T O TYPE WITHIN EACH CELL , USE THE TAB KEY D O N OT T HIN F ROM C HART
1 Patient Code: First four letters of surname, followed by first two letters of given name
HCD Funding Request Form: HCD-09 Revision: 26/1/2012