Current Management of Alzheimer's Disease
advertisement

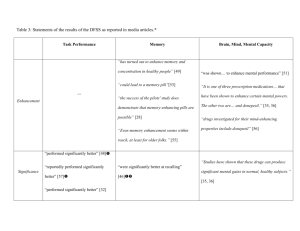
Alzheimer’s Disease The Cholinesterase Inhibitor Medications Diagnosed Dementia Patients Diagnosis visits (millions) 2.5 2.0 1.5 1.0 0.5 0 1995 PCPs 1996 1997 Neurologists 1998 Psychiatrists 1999 All others 11/99 to 10/2000 Source: National Disease and Therapuetic Index (Diagnosis codes: 3310, 2900, 2901, 2902, 2903, 2904). Cholinergic Hypothesis Role — Acetylcholine (ACh) is an important neurotransmitter in brain regions involved in memory Impact — Loss of ACh in AD correlates with impairment of memory Treatment approach — Enhancement of cholinergic function may stabilize or improve cognitive function and may affect behavior and daily functioning Mayeux R et al. N Engl J Med. 1999;341:1670-1679. Cholinergic Hypothesis • Cholinergic deficiency contributes to cognitive decline in AD • It may contribute to behavioral symptoms of AD – Psychosis-agitation – Apathy-indifference – Disinhibition – Aberrant motor behavior Cholinergic Hypothesis (cont’d) Atrophy of the nucleus basalis of Meynert, the source of choline acetyltransferase, causes deficit Other neurochemical and neurohistologic abnormalities contribute to the psychopathology of AD Cholinergic therapy may partially improve behavioral symptoms of AD Cholinergic therapy does not interrupt the disease process Current Medications Used to Treat AD *Paxil 3% *Zyprexa 3% Other 25% *Zoloft 3% Vitamin E 3% *Ativan 4% *Haldol 6% Aricept 44% *Risperdal 9% *These uses are investigational. Source: National Disease and Therapeutic Index, 1998. Cholinesterase Inhibitors • FDA-approved agents: tacrine, donepezil, rivastigmine • Doses – Tacrine: 80 to 160 mg/d – Donepezil: 5 and 10 mg/d – Rivastigmine: 6 to 12 mg/d – Galantamine: 20 to 50 mg/d • Efficacy in mild/moderate AD • Limited information on long-term treatment and in late-stage disease • May be helpful in Lewy body disease Krall WJ, Sramek JJ, Cutler NR. Ann Pharmacother. 1999. Cholinesterase Inhibitors (cont’d) Side-effect profiles are similar — Tacrine: liver toxicity, nausea, vomiting, diarrhea — Donepezil: nausea, vomiting, diarrhea, muscle cramps — Rivastigmine: nausea, vomiting, diarrhea, headache, dizziness — Galantamine: nausea, vomiting, agitation, sleep disturbances Hypothesized Treatment Effect in Alzheimer’s Disease Untreated Cholinesterase Inhibitor (CI) 6– Cognitive Function (ADAS –Cog) 4– 2– 0– -2 – -4 – -6 – -8 – -10 – -12 – -14 – -16 – 1 year 2 years Acetylcholinesterase Inhibitor Development 1993 tacrine (Cognex®) 1994 1995 1996 1997 donepezil (Aricept®) 1998 1999 2000 2001 rivastigmine (Exelon®) galantamine (Reminyl®) Characteristics of Cholinesterase Inhibitors Drug Binding Dose escalation Dosing tacrine (Cognex®) Noncompetitive, reversible 6-week steps qid donepezil (Aricept®) Noncompetitive, reversible 4-6-week step qd rivastigmine (Exelon®) Noncompetitive reversible 2-week steps bid Davis KL, Powchik P. Lancet. 1995;345:625-630. Aricept® package insert. Exelon® package insert. Tacrine (Cognex®) Half-life of 3–5 hours (variable, affected by food intake) 4-times-daily dosing of 10 to 40 mg (40 to 160 mg/day) Metabolized by the cytochrome P450 isoenzyme CYP1A2 Associated with hepatotoxicity (monthly liver testing suggested) Davis KL, Powchik P. Lancet. 1995;345:625-630. Crimson ML. Pharmacotherapy 1998;18(2 pt 2):47S-54S. Donepezil (Aricept®) The first second-generation cholinesterase inhibitor Half-life of 70 hours Once-a-day dosing of 5 to 10 mg Metabolized by cytochrome P450 isoenzymes CYP3A and CYP2D6 Higher doses associated with cholinergic side effects, but generally well tolerated Bryson HM, Benfield P. Drugs Aging. 1997;10:234-239. Aricept® package insert. Rivastigmine (Exelon®) Newer second-generation cholinesterase inhibitor Half-life of 1.5 hours Dosing (bid) of 3 to 12 mg/day Metabolism is almost totally independent of the hepatic cytochrome P450 system Gastrointestinal adverse events are common, including weight loss Exelon® package insert. Outcome Scales Used in Phase III Trials of AD Drugs Cognition Alzheimer’s Disease Assessment ScaleCognitive Subscale (ADAS-cog) Global change Clinician Interview-Based Impression of Change plus Caregiver Input (CIBIC-plus) Activities of daily living Interview for Deterioration in Daily Living Activities in Dementia (IDDD) Progressive Deterioration Scale (PDS) Clinical Dementia Rating-Sum of Boxes (CDR-SB) (ADL) Behavioral disturbances Neuropsychiatric Inventory (NPI) Alzheimer’s Disease Assessment Scale-Cognitive Subscale (ADAS-cog) Primary outcome measure — A validated, sensitive, and psychometric measure — Contains 11 items that measure cognitive change — Scoring range is 0–70; higher scores = greater cognitive impairment — Efficacy is measured as mean change from baseline Rosen WG et al. Am J Psychiatry. 1984;141:1356-1364. Clinician Interview-Based Impression of Change plus Caregiver Input (CIBIC-plus) Evaluates 4 areas: cognition, behavior, daily functioning, general psychiatric symptoms Scores range from 1 (markedly improved) to 7 (markedly worse) Schneider LS et al. Alzheimer Dis Assoc Disord. 1997;11(suppl 2):S22-32. Tacrine Safety Adverse gastrointestinal effects (somewhat alleviated by concomitant food intake) Elevated liver transaminase levels (ALT) — 25%–30% of patients with ALT > 3 times the upper limit of normal Monitoring of liver function required Farlow M et al. JAMA. 1992;268:2523-2529. Knapp MJ et al. JAMA. 1994;271:985-991. Donepezil: Percentage of Patients With Improvement in ADAS-cog (Rogers) Change in ADAS-cog (LOCF*) 4 Treatment group 7 Placebo 7.8% 26.8% 57.7% Donepezil 5 mg/day 15.4% 37.8% 78.7% Donepezil 10 mg/day 25.2% 53.5% 81.1% * Last observation carried forward. † Includes patients who did not improve or decline. 0† Rogers SL et al. Neurology. 1998;50:136-145. Donepezil Safety Individual adverse events that occurred significantly more frequently with donepezil 10 mg than with placebo: — — — — — Nausea (17%) Diarrhea (17%) Vomiting (10%) Fatigue (8%) Muscle cramps (8%) Rogers SL et al. Neurology. 1998;50:136-145. Donepezil Safety (cont) In the largest trial (N = 818), digestive system and nervous system adverse events occurred more frequently with donepezil 5 mg and 10 mg than with placebo — Digestive system = 36% vs 24% — Nervous system = 38% vs 29% Burns A et al. Dement Geriatr Cogn Disord. 1999;10:237-244. Donepezil Summary Donepezil (5* and 10 mg) improves cognition and global function in patients with mild-to-moderate AD Long-term efficacy is maintained for up to 50 weeks ADL may be partially maintained by donepezil Donepezil is generally safe and well tolerated * In the largest trial, donepezil 5 mg was significantly better than placebo using the ADAS-cog scale, but scores worsened from baseline. Rivastigmine Safety During the maintenance phase, adverse events with rivastigmine 6–12 mg (1–4 mg)* compared with placebo were: — Dizziness, 14% (8%) vs 4% — Nausea, 20% (8%) vs 3% — Vomiting, 16% (5%) vs 2% — Dyspepsia, 5% (6%) vs 1% — Sinusitis, 4% (1%) vs 1% * p < 0.05 vs placebo for all events except rivastigmine 1–4 mg for dizziness and sinusitis (not different from placebo). Corey-Bloom J et al. Int J Geriatr Psychopharmacol. 1998;1:55-65. Rivastigmine Safety (cont) Rivastigmine was generally safe and well tolerated There was no evidence of hepatotoxicity Fewer adverse events were observed with concomitant food administration versus administration without food In addition to nausea and vomiting, rivastigmine was associated with significant weight loss Exelon [package insert]. East Hanover, NJ: Novartis Pharmaceuticals Corp; 2000. Rivastigmine Summary Rivastigmine (6–12 mg) improves cognition and global function in patients with mild-to-moderate AD Positive effects on ADL have been observed in some studies Rivastigmine is generally safe and well tolerated, although cholinergic side effects occur at high doses Galantamine (Reminyl®) Galantamine has a dual mechanism of action Competitive inhibition of acetylcholinesterase1 — Allosteric modulation of presynaptic and postsynaptic nicotinic receptors2 — Galantamine improves major aspects of AD (eg, cognition, behavior, function)1 Galantamine is generally safe and well tolerated1 1. Tariot PN et al. Neurology. 2000;54:2269-2276. 2. Maelicke A, Albuquerque EX. Eur J Pharmacol. 2000;393:165-170. Dual Mechanism of Action N = nicotinic Presynaptic nerve terminal M = muscarinic ACh = acetylcholine M receptor N receptor Galantamine ACh Postsynaptic nerve terminal Galantamine ACh and other neurotransmitters • Choline • Acetic acid M receptor N receptor Maelicke A, Albuquerque EX. Eur J Pharmacol. 2000;393:165-170. Tariot PN et al. Neurology. 2000;54:2269-2276. Galantamine: Potential Advantages of Nicotinic Receptor Modulation May increase release of ACh — Release of other neurotransmitters also increases May have a neuroprotective effect Maelicke A, Albuquerque EX. Eur J Pharmacol. 2000;393:165-170. Galantamine Safety (cont) Adverse events* Placebo (n = 286) (%) Galantamine Galantamine 16 mg/day 24 mg/day (n = 279) (n = 273) (%) (%) Nausea 4.5 13.3 16.5 Vomiting 1.4 6.1 9.9 Anorexia 3.1 6.5 8.8 Agitation 9.4 10.0 8.1 Diarrhea 5.9 12.2 5.5 * 5% of patients receiving galantamine and more often than in patients receiving placebo. Tariot PN et al. Neurology. 2000;54:2269-2276. GI Adverse Events Nausea: incidence related to treatment initiation and dose escalation — Typically transient, resolving within 1 week — Rarely severe Weight loss: reported as an adverse event in 5% of patients, with none discontinuing treatment Reminyl® package insert. Comedication Minimal potential for clinically relevant drug interactions — No effect on kinetics of digoxin or warfarin As with other cholinergics, galantamine should be used with caution in patients with heart block or sick sinus syndrome Agents in Development Memantine–NMDA receptor antagonist — Improvement in patients with severe AD and VaD1 — Recent phase III trials indicate significant improvement compared with placebo in CIBIC-plus scores2 — Patients with moderately severe and severe AD benefited the most 1. Winblad B, Portis N. Int J Geriat Psychiatry. 1999;14:135-146. 2. Reisberg B. World Alzheimer Congress, 2000. Agents in Development (cont) Immunization against b-amyloid1 Huprine X—acetylcholinesterase inhibitor2 Xanomeline patch—m1/m4 muscarinic receptor agonist3 AIT-082 (purine hypoxanthine derivative)— increases neurotransmission4 COX 2 inhibitors—neuroinflammation therapy5 Protease inhibitors—target g-secretases to prevent amyloid formation6 1. Schenk DB et al. Nature. 1999;400:173-177. 2. Camps P et al. Mol Pharmacol. 2000;57:409-417. 3. Shannon HE et al. Schizophr Res. 2000;42:249-259. 4. Lahiri DK et al. Ann NY Acad Sci. 2000;903:387-393. 5. O’Banion K. World Alzheimer Congress, 2000. 6. Dovey HF et al. J Neurochem. 2001;76:173-181. Current Treatment Summary Cholinergic agents initially improve and transiently maintain cognitive abilities in patients with mild-to-moderate AD Cognitive abilities worsen over time, indicating treatment does not stop (but may delay) the progression of AD New treatments that maintain cognitive ability and stop the progression of AD are needed Referrals SHANDS at UF Geriatric Psychiatry Inpatient Unit Intake and Referral Line 352-265-5411 UF Psychiatry Clinical Trials Program 1-877-STUDY94