GB Anatomy - Tharwat kandil
advertisement

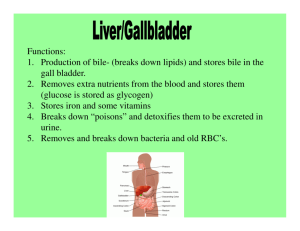
Dr. Tharwat S. Kandiel ANATOMY The gallbladder (or cholecyst, sometimes gall bladder) is a pear-shaped organ that stores about 50 mL of bile (or "gall") until the body needs it for digestion. The gallbladder is about 7-10 cm long in humans and appears dark green because of its contents (bile), rather than its tissue. It is connected to the liver and the duodenum by the biliary tract. The cystic duct leads from the gallbladder and joins with the common hepatic duct to form the common bile duct. The common bile duct then joins with the pancreatic duct, and enters the duodenum through the hepatopancreatic ampulla at the major duodenal papilla. Artery Cystic artery Vein Cystic vein Nerve Celiac Ganglia, vagus Precursor Foregut 1 Dr. Tharwat S. Kandiel HISTOLOGY The layers of the gallbladder are as follows: The gallbladder has a simple columnar epithelial lining characterized by recesses called Aschoff's recesses (lacunae of Luschka) , which are pouches inside the lining. Under the epithelium there is a layer of connective tissue. Beneath the connective tissue is a wall of smooth muscle that contracts in response to cholecystokinin, a peptide hormone secreted by the duodenum. There is essentially no submucosa separating the connective tissue from serosa and adventitia. Function of GB The gallbladder stores about 50 mL of bile , which is released when food containing fat enters the digestive tract, stimulating the secretion of cholecystokinin (CCK). The bile, produced in the liver, emulsifies fats and neutralizes acids in partly digested food. After being stored in the gallbladder, the bile becomes more concentrated than when it left the liver, increasing its potency and intensifying its effect on fats. Most digestion occurs in the duodenum. ANOMALIES The gallbladder may be absent = 0.075% The gallbladder and cystic duct may be absence. 2 Dr. Tharwat S. Kandiel The gallbladder is irregular in form or constricted across its middle; more rarely, it is partially divided in a longitudinal direction. Two distinct gallbladders, each having a cystic duct that joined the hepatic duct. (0.026%), The cystic duct may itself be doubled The gallbladder has been found on the left side (to the left of the ligamentum teres) in subjects in whom there was no general tranposition of the thoracic and abdominal viscera. The gallbladder may be intrahepatic or beneath the left lobe. Ectopic sites include retrohepatic positions, or in the anterior abdominal wall or falciform ligament, they may be suprahepatic or transversely position, floating, or retroperitoneal. They may be in the midline anterior epigastric above the left lobe or suprahepatic above the right hepatic lobe. 3 Dr. Tharwat S. Kandiel CHOLEDOCHAL CYST Choledochal cysts are congenital anomalies of the bile ducts. They consist of cystic dilatations of the extrahepatic biliary tree, intrahepatic biliary radicles, or both. Douglas is credited with the first clinical report in a 17-year-old girl who presented with intermittent abdominal pain, jaundice, fever, and a palpable abdominal mass. Pathophysiology: The pathogenesis of choledochal cysts is most likely multifactorial. Some aspects of the disease are consistent with a congenital 4 Dr. Tharwat S. Kandiel etiology, others with a congenital predisposition to acquiring the disease under the right conditions. The vast majority of patients with choledochal cysts have an anomalous junction of the common bile duct with the pancreatic duct (anomalous pancreatobiliary junction [APBJ]). An APBJ is characterized when the pancreatic duct enters the common bile duct 1 cm or more proximal to where the common bile duct reaches the ampulla of Vater. Miyano and Yamataka have demonstrated such APBJs in more than 90% of their patients with choledochal cysts. The APBJ allows pancreatic secretions and enzymes to reflux into the common bile duct. In the relatively alkaline conditions found in the common bile duct, pancreatic proenzymes can become activated. This results in inflammation and weakening of the bile duct wall. Severe damage may result in complete denuding of the common bile duct mucosa. From a congenital standpoint, defects in epithelialization and recanalization of the developing bile ducts during organogenesis and congenital weakness of the duct wall have also been implicated. The result is formation of a choledochal cyst. Anatomy: The following discussion of the pertinent anatomy of choledochal cysts is based on the Todani classification published in 1977. Type I choledochal cysts are most common and represent 80-90% of the lesions. Type I cysts are dilatations of the entire common hepatic and common bile ducts or segments of each. They can be saccular or fusiform in configuration. Type I cysts can be divided into 3 subclassifications, including type IA cysts, which are typically saccular and involve the entire extrahepatic 5 Dr. Tharwat S. Kandiel bile duct (common hepatic duct plus common bile duct) or the major portion of the duct. Type II choledochal cysts are relatively isolated protrusions or diverticula that project from the common bile duct wall. They may be sessile or may be connected to the common bile duct by a narrow stalk. Type III choledochal cysts are found in the intraduodenal portion of the common bile duct. Another term used for these cysts is choledochocele. Type IVA cysts are characterized by multiple dilatations of the intrahepatic and extrahepatic biliary tree. Most frequently, a large solitary cyst of the extrahepatic duct is accompanied by multiple cysts of the intrahepatic ducts. Type IVB choledochal cysts consist of multiple dilatations that involve only the extrahepatic bile duct. Type V choledochal cysts are defined by dilatation of the intrahepatic biliary radicles. Often, numerous cysts are present with interposed strictures that predispose the patient to intrahepatic stone formation, obstruction, and cholangitis. The cysts are typically found in both hepatic lobes. Occasionally, unilobar disease is found and most frequently involves the left lobe. 6 Dr. Tharwat S. Kandiel The patient may present at any age with Obstructive jaundice Cholangitis and Abd signs, with RUQ swelling in some cases It is a premalignant condition Diagnosis by US and MRI Radical excision of the cyst is the treatment of choice with Roux – en –Y reconstruction. 7