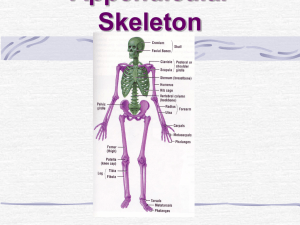
extremities chart
advertisement

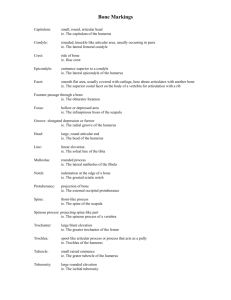
Extremities Radiology Chart Anomaly/Line 1 ER, IR, N LR MR View Bone AC spot AP shoulder Clavicle, acromion Acromioclavicular Joint Space AP shoulder or AP AC jt Acromion (scap), clavicle Acromioclavicular Spot AP shoulder Clavicle Acromiohumeral Interval AP shoulder Humerus, acromiom (scap) All Long Apophysis Arcs of carpal alignment PA wrist Carpals Carpal bones Any Carpals Carpal Coalition AP wrist Lunate and triquetrum Carpals PA wrist Carrying angle AP elbow Clavicle Deltoid tuberosity variations AP shoulder Humerus Straight or 10-15º cephalad None Humerus, ulna Clavicle None Carpals PA clavicle None Tube Tilt None None None None None None Straight or 10-15º caudad None Measurement/Comment Top part of jt is wide. Usu viewed bilaterally. Meassure inf and sup aspects of AC jt and average. Normal 2-4 mm. Common in weight lifting. Signifies osteolysis (look for cortex of clavicle), HPT, rheumatoid arthritis. Measure sup and inf aspects of jt space and average. Normal: 2-4 mm (3 mm ave). Diff b/t both AC jts should not be more than 2-3 mm. ↓ space = DJD; ↑ space = trauma, osteolysis, HPT, rheumatoid arthritis. For distal clavicle and AC jt. Turn pts head away from side being radiographed. See Clavicle (P to A projection). Distance b/t inf margin of acromion and sup aspect of humeral head. Normal: 7-11 mm (ave 9 mm). < 7 mm = rotator cuff tear Outgrowth or projection from 2º center of ossification; bony attaachment site for ligaments and tendons. Ex: greater tuberosity, lesser trochanter. Three arcs are outlined. Arc 1 = proximal articular surfaces of scaphoid, lunate, triqueetrum. Arc 2 = distal articular surfaces of same bones. Arc 3 = prox surfaces of capitate and hamate. Normal is smooth and continuous. Scaphoid, lunate, triquetrum, pisiform, hamate, capitate, trapezoid, trapezium. Normal anomaly. Bones can fuse, esp lunate and triquetrum. Pt may have mechanical problems or osteoarthritis earlier than usual. Smaller view is best for viewing carpals. Scaphoid, lunate, triquetrum, pisiform, trapezium, trapezoid, capitate, hamate. Line AB drawn down humerus, to long axis. Line CD drawn down center of ulna and to long axis. Angle formed ~ 15º. Significance: may be fx or deformities. Turn pts head away from side being radiographed. Tube tilt will get through angle better. Want to define med to lat edges. Preferred in anatomic detail and in kyphotic pts. See AC Spot for A to P projection. Normal variant. 1/3 way down shaft of humerus. Irregular bump on deltoid tuberosity. Extremities Radiology Chart Anomaly/Line 2 ER, IR, N LR MR View Bone All Long AP shoulder Humerus, scap All Long External Shoulder Scap, humerus Fat planes AP shoulder Humerus, scap Flap fracture AP shoulder Scapula, humerus Diaphysis Dislocation Epiphysis External rotation Fracture Fracture AP elbow, lat elbow AP elbow, lat elbow, med elbow Radius Humerus Tube Tilt None None None None Measurement/Comment The shaft of a long bone – longest and narrowest portion. Provides mechanical support. Houses bone marrow. Developed from 1º center of ossification. Anterior dislocation will go inferior (most common); post dislocation (rare), usu due to shocks or seizures, will go superior b/c of scapula. End of a long bone developed from 2º center of ossification; covered w/artic cart; supports joint movement. Have pt stand A to P, and turn arm away from body until palm of hand faces laterally. (thumb moves in arc from anterior to lateral to posterior). All adult shoulder views are done in lat (or ext) rotation. None Normal variant. Folds around the shoulder. None Flap of bone torn from bone. Sometimes accompanied with dislocation. Usu from trauma. None Radial head/neck fx most common in adults. None Supracondylar most common fx in children. Most common fx in adult or child. Artery is different for scaphoid bone; artery enters distal end. If fx is not treated, proximal part dies b/c of malnourishment. Cause: falling on extended hand Fracture AP, lat, lat oblique wrist Scaphoid None Fracture Lat wrist Triquetrum None 2nd most common fx. Can see piece of floating bone. Cause: landing on dorsal hand Fracture of clavicle Bilateral AP clavicle Clavicle 15º cephalad Important to compare sides. Protect thyroid from X-rays, if possible. Separate views can protect thyroid more. Fracture, Barroom Med oblique hand MCP None Fracture, Boxer’s Med oblique hand MCP None AP shoulder Humerus, scap Glenohumeral Joint Space Internal rotation Internal Shoulder Scap, humerus None None 5th metacarpal fx of head. Compare with “boxer’s fx”. (MCPs = knuckles). 2nd or 3rd MCP head fx. Compare with ‘barroom fx”. (MCPs = knuckles) Sup, inf and middle aspects of joint space measurements are averaged. Normal: 4-5 mm. < 4mm = arthritis (usu DJD). > 5 mm = acromegaly or posterior dislocation. Have pt stand A to P, and turn arm towards body until palm faces laterally. (thumb moves in arc from anterior to medial to posterior). Internal rotation pts tend to raise shoulder. Looks like humerus on top of acromiom. Extremities Radiology Chart Anomaly/Line Longitudinal axial alignment of wrist Metacarpal sign 3 View Bone Lat wrist Radius and hand bones ER, IR, N LR MR Tube Tilt Measurement/Comment none Draw line through center of radius in extended wrist and hand. Radius, lunate, and 3rd metacarpal shouls be aligned along long axis. Deviation = fracture or dislocation. PA hand Metacarpals All Long Lat hand, PA hand, med oblique hand Phalanges Optional view Axial shoulder Glenoid fossa (scap), humerus Optional view Abduction “Baby Arm” shoulder Clavicle, scapula None Optional view Y- (outlet) oblique shoulder Humerus, scap None Optional view Spot hand Indiv hand bones None Optional view stress Indiv hand bone None Ossicles Any hand Carpals None Ossification centers PA hand MCPs None All Metacarpals, usually Metaphysis Normal variants Osteophyte None None Draw line along heads of 4th and 5th metacarpal heads. Normal: 3rd MCP head shoud be at or prox to line. Deviation: 4th MCP is too short. Signifies Turner’s Syndrome or fx Zone b/t physis and diaphysis; expanded area that tapers into the shaft. Greatest metabolic region of bone. Responsible for forming of long bone shape. None Bifid phalanx, extra phalanx, esp in thumb Pointing straight up through axilla Sees glenohumeral jt and space. Pts arm is held flexed abducted 90º to floor in front of them, Tube is aimed up through axillary space. None Periosteum All Long None Physis All Long None Position pt A to P, with arm abducted to 90º, elbow flexed to 90º, plam of hand faces tube. For AC jt, proximal humerus, clavicle, lung apex, coracoid and acromium. Have pt breathe in, breathe out and hold. Positon pt w/ shoulder against bucky. Beam goes through scap. Look for big, open space at supraspinatus. Either lat or PA view. Close up of one specific area—easier to locate problem Pushes problem region in same direction of injury. Especially helpful for hairline fx and ligament tears. Bones in carpals; look identicle to sesamoids. Located at proximal end of digit 1 (thumb), and distal end of digits 2-5. Bone spurs. Signifies osteoarthritis. Joint is degenerating, and bone develops osteophytes to protect against bone-on-bone rubbing. Soft tissue enveloping around long bone; attached by sharpey’s fibers. Maintains caliber, integrity of bone. Appositional bone growth. Not radiographically visible when normal. In growing bones; contributes to enchondral growth. Located b/t epipysis and metaphysis; seen as a radiolucent band on radiographs. Extremities Radiology Chart Anomaly/Line 4 ER, IR, N LR MR Tube Tilt View Bone Physis mimicking fracture AP shoulder Humerus None Pseudotumor of the humerus AP shoulder Humerus None Radiocapitellar line Lateral elbow Humerus, radius Sail sign Secondary ossification centers Lat elbow Humerus None None Any Humerus, radius, ulna Any hand MCPs, phalanges AP shoulder Scap, humerus, clavicle Standard view AP elbow Humerus, radius, ulna Standard view Oblique, elbow Humerus, radius,ulna Standard view Lateral elbow Humerus, ulna, radius None Standard view Medial oblique elbow Humerus, ulna None Standard view PA wrist None Sesamoids Standard view Carpals None None None None None Measurement/Comment Normal variant. Jagged radiolucent line, which is posterior physis . Looks like fracture, esp in children. Edge depends on of film and pt, how shoulder is positioned. Normal variant. Large lucent region. Looks like a tumor, but it is not. Due to greater tuberosity in rotation. Line drawn down center of radius and parallel ot long axis. Should pass through center of capitellum. Significance: radial head subluxation or dislocation. Ant fat pad more radiolucent than rest of tissue. Usu in shape of triangle. Significance: fx in jt somewhere, which swelling or bleeding ‘lifted’ fat pad up. Age of appearance: capitellum → 1 yr; radial head → 4 yrs; med epicondyle → 7 yrs; trochlea → 10 yrs; olecranon → 10 yrs; lateral epicondyle → 11 yrs. Bones in tendons or ligaments, especially around joints. Looks identicle to ossicles. Pisiform is a sesamoid. Demonstrates proximal humerus, scapula, clavicle, rib cage. Want to see some lung (for disease – can refer px to shoulder), and some muscle tissue. Look for physis to determine if child. Viewed, elbow in extension. Elbow extended on bucky, hand in supinated position. Radius and ulna overlap proximally. Olecranon process should be in the middle; condyles level with each other. Viewed, elbow in extension. Olecranon process is in lat or medial position, depending on angle. Ulna and radius tend to separate out w/lat oblique; rad and ulna cross in med oblique. Elbow is flexed at 90º. Arm resting on bucky, thumb up. Humerus as flat as possible to bucky to prevent distortion of humerus. Views radioulnar jt, distal humerus, prox rad and ulna. Arm in extended position. Hand is pronated on bucky.Views medial aspect of elbow. Allows carpal bones and joints to be viewed, also distal radius and ulna. Greater detail than PA hand view. Extremities Radiology Chart 5 View Bone ER, IR, N LR MR Tube Tilt Standard view Lateral wrist Carpals, distal radius and ulna None Standard view Medial oblique wrist None Hand is semipronated (finger and index from an “O”). Standard view PA hand None Thumb is in oblique view. Other digits in PA Standard view Medial oblique hand Hand bones, distal radius and ulna None Thumb is in lat view. Hand in 35º-40º All digits spread out as far as possible. Don’t mistake flexed finger for problem. Standard view Lateral hand Hand bones, distal radius and ulna None. Supernumary AP wrist Carpals None Supracondylar process Lat elbow Humerus Anomaly/Line Ulnar variance PA wrist Vacuum sign lat elbow Carpals, distal radius and ulna Hand bones, distal radius and ulna Ulna, radius None None None Measurement/Comment Thumb is ant, out of the way. Views relationships of carpals (esp lunate) and distal radius. Thumb in PA. Difficult to see individual carpals. Should have full “ray” (spread of fingers) on view. Normal anomaly. Too many carpal bones. Need to count carpals. Pt may have mechanical problems or osteoarthritis earlier than usual. Normal variant. Struther’s ligament attaches process to humerus, forms foramen. Median N, brachial art, sometimes ulnar N, radial art can become ‘entrapped’ Draw line A at distal ulna at Radioulnar jt, and line B at the level of distal radial styloid process ( to line A). Normal = line B 9-12 mm distal to line A. > 12 mm = negative ulnar variance (ulna to short); < 9 mm = positive ulnar variance (ulna is too long) Viewed in flexion. Normal anomaly. Thin line b/t humerus and glenohumeral jt. If in any other joint, signifies DJD (osteoarthritis).