reconstruction of the anterior talofibular ligament for
advertisement

RECONSTRUCTION
FOR
OF
THE
ANTERIOR
TREATMENT
0.
From
THE
K.
SEFTON.
St James’s
J.
OF
GEORGE,
University
THE
J.
Hospital,
TALOFIBULAR
M.
UNSTABLE
FITFON,
Leeds,
LIGAMENT
H.
and
ANKLE
McMULLEN
Victoria
Hospital,
Worksop
Chronic
instability
of the ankle is frequently
due to disruption
of the fibres of the anterior
talofibular
ligament
and the anterolateral
capsule.
This allows
momentary
subluxations
at the ankle joint; the talus
tilts
into an abnormal
through
ligament
the
The
lateral
The
main
varus
detailed
anatomy
side of the ankle
components
gives
and
rotates
forwards
The use of a free
of the ankle
without
the
anterior
talofibular,
the posterior
talofibular
by the capsular
fibres.
conflicting
opinions
the
ligaments,
The recent
as to
the
site
The
anterior
talofibular
( 1 977)
ligament
extending
neck
of
have
shown
by
most
commonly
and Anderson
and
ligament
(1949)
is a distinct
from the
the talus.
and
anterior
border
of
Ala-Ketola
et a!.
arthrography
that
it is the
injured.
Work
by Leonard
LeCocq
(1954)
suggests
that
rupture
of this element
of the complex
allows
anterior
displacement
of the talus from the mortise
of the joint in
the
coronal
plane,
rotation
about
degrees
because
capsule.
The
of the
fibres
its vertical
of the
talar
tilting
by medial
of 7 to 10
to the
talus.
Clinical
(Bostr#{246}m 1966).
that
Although
injury
to
primary
and
lateral
in the
1 966).
common
The
from
the
tip
of the calcaneus.
The
when
the ankle
is
therefore
this
ligament
recurrent
posterior
lacks
inversion
talofibular
band arising
from the posterior
running
to the posterior
aspect
disruption
of this
of persistent
experimental
talofibular
instability
calcaneus
metatarsal.
subtalar
provides
of
have been
between
which
passes
evolved
to create
tight
the lateral
malleolus
or between
the lateral
malleolus
and
These
procedures
restrict
inversion
joint
unnecessarily.
excellent
long-term
It is more
stability
CLINICAL
logical
to
The
on
without
restriction
diagnosis
clinical
span
of chronic
and
many
instability
radiological
years
with
and swelling.
The
abnormal
movement
demonstrate
inversion
EXAMINATION
of the
signs.
recurrent
important
ofthe
ankle
Symptoms
inversion
to the
rotational
tibia
and
displacement
depends
invariably
injuries,
pain
feature
on examination
talus in the ankle mortise.
this,
stress
must
be applied
of the foot and to displace
the talus
lateral
malleolus.
is
To
to cause
forward
in
The
anterior
then easily felt by palpation
of
the talus
in front
of the lateral
malleolus.
Bostr#{246}m
( 1 966) referred
to this as the
anterior
drawer”
sign. In
comparison
Gillespie
and Boucher
( 1 97 1 ) found evaluation of pure talar
tilt was difficult
and not as helpful.
is
“
Stress
However,
radiography
an abnormality
correlate
(Freeman
with
1 965)
is used to confirm
the diagnosis.
of talar
tilt does
not always
functional
and varus
ligament
is very
work
ligament
shows
is the
Witten
Mathieu
1 960). As asymmetry
1 975), the critical
ankle,
greater
on
of the
axis
inversion.
G. K. Sefton,
F.R.C.S.Ed..
Senior
Orthopaedic
Registrar,
St James’s
University
J. George,
M.D..
Os Rzezzypospolitey
3/93,
61/397
Poznan,
Poland.
J. M. Fitton,
F.R.C.S.,
Consultant
Orthopaedic
Surgeon,
St James’s
University
H. McMullen,
F.R.C.S.,
Consultant
Orthopaedic
Surgeon,
Victoria
Hospital,
Requests
for reprints
should
be sent to Mr G. K. Sefton.
352
a vertical
reconstruct
only the anterior
tabofibular
ligament
using a
free
tendon
graft.
This
corrects
the instability
of the
ankle
without
restricting
inversion
at the subtalar
joint.
An operation
has been
devised
which
fulfils
this
requirement.
It has been
used
for many
years
and
may
clinical
and
the anterior
cause
extends
lateral
surface
and
relaxed
is a wide strong
of the fibula
and
rare
main
talus
damage
ligament
1 973)
significance
(Bostr#{246}m
ligament
surface
and
of the
about
operations
structures
relation
(Grond
major
injury
axis,
associated
calcaneofibular
fibula
to the
are horizontal
inverted
of the
displacement
inwards
and the
the fifth
at the
and
extent
of the
lesion
in chronic
inversion
injuries.
Aufranc
(1958)
states that ofall the ligamentous
injuries
those
of the ankle,
especially
the fibular
collateral
ligaments,
are the commonest
and the least understood.
sizeable
structure
the fibula
to the
and
tendon
graft to reconstruct
the anteriot
talofibular
restricting
movement
at the subtalar
level.
numerous
ligamentous
of the ligaments
stabilising
has been well documented.
are
calcaneofibular
and
which
are reinforced
literature
position
the medial
malleolus.
restores
the stability
occur
in
the
Hospital,
Hospital,
Worksop,
otherwise
instability
of the
ankle
tilting
of up to 20 degrees
normal
symptomatic
Leeds
LS9
Leeds
LS9
Nottinghamshire,
THE
ankles
(Rubin
and
is rarely
found
(Laurin
and
sign is a talar tilt substantially
side.
7TF,
7TF,
JOURNAL
England.
England.
England.
OF BONE
AND
JOINT
SURGERY
RECONSTRUCTION
OPERATIVE
The
operation
is done
ing
tourniquet.
from
the
plantaris
tendon
of the
suitable
alternatives.
passing
away
to expose
lateral
fibres
of the
made
as shown
below
which
of the
from
and
exposure
1 . The
diameter
first
hole
surface
horizontal
and
talus
extensor
lateral
The
sheet
some
plane
the
side
and
The
of the
is deep
to the
aspect.
It is, of course,
that
backwards
on its lateral
and
avoid
damaging
the
passes
upwards
through
the
lateral
to the
surface,
a little
below
the
a good
calcaneal
through
lowest
bony
part
cover.
surface
is easily
difficult
Care
of the
malleolus
entry
of the
fourth
its lowest
for
the
first
time
thirty-four
ankles
in
been
stabilised
using
this
been
possible
to examine
reported
that
they
were
for examination
Ten were
lost
of operation
had
and so were
to follow-up.
varied
from
ten
to
Table
I. Grading
of symptoms
of the ankle
in instability
of the
lateral
ligament
Grade
I
Full activity,
including
strenuous
No pain.
swelling
or giving
way.
Grade
2
Occasional
No giving
Grade
3
No
aching
way or
only
feeling
sport.
after
strenuous
of apprehension.
exercise.
Grade
4
giving
way
but
some
rough
remaining
especially
on
Recurrent
activities,
instability
and giving
with episodes
of pain
apprehension.
ground.
way
and
in normal
swelling
these
be taken
The
from
point
talus,
to construct
talus.
at the
articular
also
years
second
body
fibular
must
age
perforated.
the
of the
twelve
did not attend
in the review.
a little
neck
ridge
last
patients
have
but it has only
Six other
patients
are
through
margin
joint.
horizontally
tunnels
horizontally
anterior
ankle
that
surface
holes
of the
runs
leave
its
drill
side
hole
353
of the
of the
outer
convenient
four
passes
to
in a plane
still
1.IGAMENT
stripped
of the
divide
the
thirty-four
procedure
eighteen.
satisfied
but
not included
posterior
thin
is easily
to the
are
oblique
the
The
body
to
the
brevis
by an
malleolus.
neck
absent,
peroneus
is exposed
necessary
plantaris
are
capsule
of appropriate
through
a firm
TAI.OFIBULAR
During
derived
a Brand
or the
the
of the
superficial
downwards
third
talus
burrs
its
presents
The
be
tendon
damaged
be
preferably
downwards
above
sufficient
in Figure
level
goes
ankle
aspect
to gain
from
the
hole
of the
slightly
It may
Paton’s
fibula
toes
an exsanguinat-
using
and
of the
the
lateral
leg
using
talus.
Using
the
the
same
an inch
replaces
malleolus.
retinacular
neck
and
about
should
muscle
aspect
which
graft
the
extensors
fibula
tissue
the
of
forwards
of the
of scar
the
long
ANTERIOR
RESULTS
anaesthesia
plantaris
anterolateral
incision
aspect
for
If the
tendons
The
general
tendon
stripper.
THE
TECHNIQUE
under
Material
OF
to
fifty-eight
hole
point
on
hole.
years
complained
ated
(average
twenty-nine
of recurrent
pain
and
before
operation
years
with
lateral
swelling.
had
a
The
ranged
mean
of
five
those
who
wished
were
sports.
grading
of
years.
two
able
to
follow-up
participate
by
in Grade
their
Jones
and
the symptoms
sixteen
being
2. Clinical
two it was
uneventfully.
in
Good,
revealed
that there
was no restriction
ment.
Particular
attention
was directed
ment
of subtalar
movement.
In sixteen
was normal,
in the other
All the wounds
healed
to fifteen
The
a period
varying
from six
five years).
All patients
normal
occupations
and
suggested
1 and
had
associ-
symptoms
six months
Livingstone
(1975)
was used to evaluate
(Table
I). The results
were all satisfactory,
in Grade
All
with
duration
from
examinations
were made
after
months
to twelve
years (average
had been
able to resume
their
favourite
The
years).
instability
examination
of ankle
moveto the assesscases
inversion
limited
by 5 degrees.
DISCUSSION
Operative
been
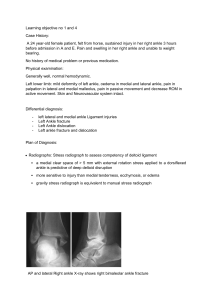
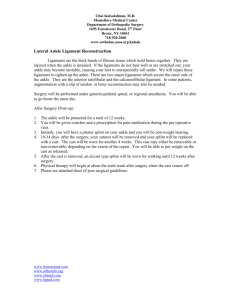
Fig.
Diagram
to show
the
four
drill
through
which
the
tendon
graft
is
inserted.
The
plantaris
tendon
through
these
thickness
of the
and
graft
fixed
are
knotted
by
one
demonstrated
restored.
The
foot
below-knee
resumed
when
at six
weeks
VOL.
61-B,
the
on the
two
anchoring
stability
ankle
are
then
Weight-bearing
wound
to allow
has
No. 3. AUGUST
surface
silk
of
and
sutures:
the
the
and
of the
plaster
plaster
may
activities.
four
ends
easily
has
been
angle
may
be removed
end
of the
foot
in relation
limit
normal
patients
inversion,
malleolus
is then
joint
at a right
the
in double
the
lateral
it
ankle
immobilised
weight-bearing
1979
to be passed
tight,
through
healed,
graduated
enough
It is pulled
normal
and
plaster.
long
holes.
together
or
that
is usually
four
of the
by many
Jones
1955;
Lee
procedures
involve
which
the peroneus
1
holes
repair
described
in a
be
A
suggested
fibula.
ligament
authors
operated
as did
ankle
1953;
has
Watson-
1957; Good
et a!. 1975)
but their
some
form
of lateral
tenodesis
by
brevis
tendon
is fixed to the lower
They
act by restricting
on
those
by
Evans
treated
by
different
approach
to
by Burrows
(1955),
of the
of the
(Evans
to the leg and can only
movement
at the subtaloid
anterior
talofibular
This
restores
the
movement
lateral
ligament
normal
ankle
joint
inversion
(1953)
had
Elmslie
(1934).
limited
the problem,
as
is to reconstruct
using
a free tendon
anatomy
and
allows
and
of the
be effective
if they
level.
All of the
the
subtalar
joint.
first
the
graft.
full
This
354
G.
may
prove
wishing
to
Indeed,
absolutely
resume
one
of
K.
SEFTON,
essential
a career
in
our
patients
J.
GEORGE,
for a young
a professional
subsequently
J.
M.
person
sport.
FITTON,
H.
The
dysfunction
suffered
a
MCMULLEN
review
after
ankles
were
demonstrated
operation
stable.
This
compound
fracture-dislocation
of his talus while playing
rugby
football.
At
exploration
the
reconstructed
that
derangement
of
mechanism
is a factor
anterior
takes
ligament
was
intact.
This operation
was devised
by Mr J. M. Fitton
and Mr H. McMullen
presented
in this paper
is derived
from
a study
of their
patients.
and
has
some
been
time
used
a prolonged
the patients
before
reflects
Freeman’s
hypothesis
the
proprioceptive
in ankle
instability,
protective
and that
for proprioceptive
at both
period
of
felt their
hospitals
adaptation
for a number
it
to occur.
of years.
The
information
REFERENCES
Ala.Ketola,
injuries.
L., Puranen,
Radiology,
J., Koivisto,
125, 63-68.
J.
Anderson,
K. J., and LeCocq,
Surgery,
36-A,
825-832.
Aufranc,
Year
Burrows,
37-B,
Evans,
( I 966)
H. J.
169.
Sprained
(1 955)
R. C. (1934)
Freeman,
47-B,
Gillespie,
H. S., and
53-A,
920-924.
Good,
C.
j.,
Jones,
subluxation
M.
A.,
G.
Leonard,
Rubin,
(1957)
and
M.
G.,
Watson-Jones,
and
H.
J.
(1949)
Witten,
Sir
of
P.
Llvlngstone,
Sagittal
Injuries
of the
The
R. (1 955)
Fractures
ankle-a
foot
after
(1975)
mobility
Joint
of
normal
of the
of the
and
Injuries.
the
ankle.
fibular
Fourth
ankle.
Journal
collateral
edition.
of
lateral
of
Bone
Journal
.
of
of ankle
ofBone
Scandinavica,
Journal
of
ankle.
the
and
Chicago:
132,
Bone
of the
and
and
Joint
Journal
and
London:
THE
of
of
ankle.
Joint
The
551-565.
and
Joint
Surgery,
Society
of
Medicine,
and
Joint
Surgery,
and
Joint
Surgery,
JOURNAL
99-104.
828-834.
373-377.
Joint
Surgery,
S. Livingstone
OF
Neerlandicum,
108,
39-A,
31-A,
and
E. and
7, 63-65.
Research,
Surgery,
Surgery,
ofBone
Bone
(‘hirurgicum
Related
Joint
Bone
injury.
Archivum
and
Bone
Royal
Journal
of the ankle.
of
the
Journal
ankle.
ligament
ligaments.
Edinburgh
classification
by E. F. Cave.
Chirurgica
Orthopaedics
Journal
Edited
Proceedings
ligaments
Clinical
joint.
of the ankle
ankle.
of the
instability
of the
and
364-367.
ligament
collateral
ankle
Acta
of the
100,
injuries
582-585.
ruptures.
treatment.
lateral
lateral
pp.
ligament
surgical
the
ofligament
ligament
Injuries,
lateral
Reconstruction
of the
ligaments
angle
to
Other
of Surgery,
of
of the fibular
dislocation
lateral
and
injuries
repair
of injuries
talar-tilt
Annals
diagnosis
collateral
ligament
of the
method
Watson-Jones
in recurrent
M. (1960)
ankle-joint.
the
and
of “chronic”
rupture
in the
to the fibular
In Fractures
treatment
B. N
treatment
(I 975)
repair
the
Arthrography
of injury
overlooked
of the
(1 97 1)
surgical
Surgical
Surgical
of
Instability
Boucher,
treatment
injuries.
for
instability
J. T. H. (1 973) The
25, 131-136.
Laurin,
C., and Mattdeu,
H.
VI.
operation
Recurrent
Grond,
Lee,
Operative
Recurrent
( 1 965)
M. A. R.
669-677.
Puuper#{225}, M. (1977)
ligamentous
ankles.
Elmslie’s
D. L. (1 953)
46, 343-344.
and
F. ( 1 954)
0. E. (1958)
Ankle
injuries,
Book
Publishers
Inc.
Bostr#{246}m, L.
Elmslie,
E.,
BONE
42-A,
3 1 1 -326.
Ltd.
AND
JOINT
SURGERY