ECG workout_Chap07.indd
advertisement

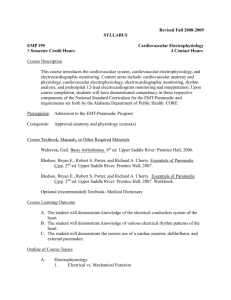
7 Atrial arrhythmias Mechanisms of arrhythmias Under certain circumstances cardiac cells in any part of the heart may take on the role of pacemaker of the heart. Such a pacemaker is called an ectopic pacemaker (a pacemaker other than the sinus node). The result can be ectopic beats or rhythms. These rhythms are identified according to the location of the ectopic pacemaker (for example, atrial, junctional, or ventricular). The three basic mechanisms that are responsible for ectopic beats and rhythms are altered automaticity, triggered activity, and reentry: Altered automaticity — Normally the automaticity of the sinus node exceeds that of all other parts of the conduction system, allowing it to control the heart rate and rhythm. Pacemaker cells in other areas of the heart also have the property of automaticity, including cells in the atria, atrioventricular (AV) junction, and the ventricles. The rates of these other pacemaker sites are slower. Therefore, they’re suppressed by the sinus node under normal circumstances. Because the inherent firing rate of the pacemaker cells of the sinus node is faster than the other pacemaker sites, it is the dominant and primary pacemaker of the heart. An ectopic pacemaker site can take over the role of pacemaker either because it usurps control from the sinus node by accelerating its own automaticity (enhanced automaticity) or because the sinus node relinquishes its role by decreasing its automaticity. Conditions that may predispose cardiac cells to altered automaticity include myocardial ischemia or injury, hypoxia, an increase in sympathetic tone, digitalis toxicity, hypokalemia, and hypocalcemia. Triggered activity — Triggered activity results from abnormal electrical impulses that occur during repolarization when cells are normally quiet. The ectopic pacemaker cells may depolarize more than once after stimulation by a single electrical impulse. Triggered activity may result in atrial, junctional, or ventricular beats occurring singly, in pairs, in runs (3 or more beats), or as a sustained ectopic rhythm. Causes of triggered activity may include myocardial ischemia or injury, hypoxia, an increase in sympathetic tone, and digitalis toxicity. Reentry — Normally an impulse spreads through the heart only once. With reentry, an impulse can travel through an area of myocardium, depolarize it, and then reenter that same area to depolarize it again. Reentry involves a circular movement of the impulse, which continues as long as it encounters receptive cells. Reentry (like triggered activity) may result in atrial, junctional, or ventricular beats occurring singly, in pairs, in runs, or as a sustained ectopic rhythm. Common causes of reentry include myocardial ischemia or injury, hyperkalemia, and the presence of an accessory conduction pathway between the atria and the ventricles. Atrial arrhythmias (Figure 7-1) originate from ectopic sites in the atria. Ectopic P waves from the atrium differ in morphology (shape) from the normal sinus P waves (Figure 7-2). For example, in slower atrial rhythms (premature atrial contractions, wandering atrial pacemaker) the P wave may appear as a small, pointed, and upright waveform; a small squiggle that is barely visible; or it may be inverted if the impulse originates from a site in the lower atrium near the AV junction. In faster atrial rhythms, the ectopic P wave is either superimposed on the preceding T wave, appears in a sawtooth pattern (atrial flutter), or is seen as a wavy baseline (atrial fibrillation). Some atrial arrhythmias may be associated with rapid ventricular rates. Increases in heart rate decrease the length of time spent in diastole. If diastole is shortened, there is less time for coronary artery perfusion and less time for adequate ventricular filling. Thus, an excessively rapid heart rate may lead to myocardial ischemia and may compromise cardiac output. Wandering atrial pacemaker A wandering atrial pacemaker (WAP) (Figure 7-3 and Box 7-1) occurs when the pacemaker site shifts back and Box 7-1. Wandering atrial pacemaker: Identifying ECG features Rhythm: Rate: Regular or irregular Usually normal (60 to 100 beats/minute) but may be slow (< than 60 beats/minute) P waves: Vary in size, shape, and direction across rhythm strip; one P wave precedes each QRS complex PR interval: Usually normal duration, but may be abnormal depending on changing pacemaker location QRS complex: Normal (0.10 second or less) 85 ECG workout_Chap07.indd 85 4/29/2011 2:48:50 PM 86 Atrial arrhythmias Figure 7-1. Atrial arrhythmias. Pointed T-P wave Squiggle Sawtooth Inverted Wavy Figure 7-2. Atrial P waves. forth between the sinus node and ectopic atrial sites. The P wave morphology will vary across the rhythm strip as the pacemaker “wanders” between the multiple sites. The ectopic P wave may appear as a small, pointed, and upright waveform; a small squiggle that is barely visible; or it may be inverted if the impulse originates from a site in the lower atrium near the AV junction. Generally, at least ECG workout_Chap07.indd 86 three different P-wave morphologies should be identified before making the diagnosis of WAP. The heart rate is usually normal, but may be slow. The rhythm may be regular or irregular (each impulse travels through the atria via a slightly different route). The PR interval is usually normal, but may be abnormal because of the different sites of impulse formation. The 4/29/2011 2:48:50 PM Premature atrial contraction Figure 7-3. Rhythm: Rate: P waves: PR interval: QRS complex: Wandering atrial pacemaker. Irregular 60 beats/minute Vary in size, shape, across rhythm strip 0.10 to 0.14 second 0.04 to 0.08 second. QRS complex is normal in duration. The distinguishing feature of this rhythm is the changing P-wave morphology across the rhythm strip. WAP may be a normal phenomenon seen as a result of increased vagal effect on the sinoatrial (SA) node, slowing the sinus rate and allowing other pacemaker sites an opportunity to compete for control of the heart rate. It can also occur due to enhanced automaticity of atrial pacemaker cells that usurp pacemaker control from the SA node. WAP is commonly seen in patients with chronic obstructive pulmonary disease. WAP usually isn’t clinically significant, and treatment is not indicated. If the heart rate is slow, medications should Figure 7-4. Rhythm: Rate: P waves: PR interval: QRS complex: ECG workout_Chap07.indd 87 87 be reviewed and discontinued if possible. If the heart rate is slow and the patient is symptomatic, treatment of the rhythm is the same as for symptomatic sinus bradycardia. When WAP is associated with a heart rate greater than 100 beats per minute, the rhythm is called multifocal atrial tachycardia (MAT) (Figure 7-4). MAT is a relatively infrequent arrhythmia and is most commonly observed in patients with severe chronic obstructive pulmonary disease. Premature atrial contraction A premature atrial contraction (PAC) (Figures 7-5 through 7-12 and Box 7-2) is an early beat originating from an Multifocal atrial tachycardia (MAT). Irregular 140 beats/minute Vary in size, shape, and direction across rhythm strip 0.10 to 0.14 second 0.04 to 0.08 second. 4/29/2011 2:48:51 PM