From www.bloodjournal.org by guest on March 6, 2016. For personal use only.
Blood First Edition Paper, prepublished online January 30, 2007; DOI 10.1182/blood-2006-10-054528
Ancestry and Pharmacogenetics of Antileukemic Drug
Toxicity
Shinji Kishi1, Cheng Cheng2,4, Deborah French1, Deqing Pei2, Soma Das6, Edwin H. Cook6,
Nobuko Hijiya3,4,5, Carmelo Rizzari7, Gary L. Rosner8, Tony Frudakis9, Ching-Hon Pui3,4,5,
William E Evans1,4,5 and Mary V. Relling1,4,5*
Departments of 1Pharmaceutical Sciences, 2Biostatistics, 3Hematology-Oncology,
4
Hematologic Malignancies Program, St. Jude Children's Research Hospital, and 5University of
Tennessee, Memphis, TN, 6Department of Psychiatry, Pediatrics, and Human Genetics,
University of Chicago, Chicago, IL. 7Clinica Pediatrica, Universita di Milano, Milano, Monza,
Italy, 8Biostatistics, M.D. Anderson Cancer Center, Houston, TX and 9 DNAPrint Genomics,
Sarasota, FL.
One of the authors (Tony Frudakis) is employed by a company (DNAPrint Genomics) whose
product (AncestrybyDNA 2.5) was used in the present work for some genotyping. These
genotyping results were donated by DNAPrint Genomics.
*To whom reprint requests should be addressed: Department of Pharmaceutical Sciences, St.
Jude Children’s Research Hospital, 332 North Lauderdale, Memphis TN 38105-2794.
Phone: 901-495-2348; Fax: 901-525-6869: e-mail: mary.relling@stjude.org
Running title: Pharmacogenetics of ALL Toxicity
Clinical Observations, Interventions, and Therapeutic Trials
1
Copyright © 2007 American Society of Hematology
From www.bloodjournal.org by guest on March 6, 2016. For personal use only.
Abstract
Treatment-related toxicity in acute lymphoblastic leukemia (ALL) cannot only be lifethreatening but may affect relapse risk. In 240 patients, we determined whether toxicities were
related to 16 polymorphisms in genes linked to the pharmacodynamics of ALL chemotherapy,
adjusting for age, race (self-reported or via ancestry-informative markers), sex and disease
risk group (lower vs. higher-risk therapy). Toxicities (gastrointestinal, infectious, hepatic, and
neurological) were assessed in each treatment phase. During the induction phase, when drugs
subject to the steroid/cytochrome P4503A pathway predominated, genotypes in that pathway
were important: vitamin D receptor (odds ratio [OR] 6·85 [95% confidence interval 1·73-27·0])
and cytochrome P4503A5 (OR 4·61 [1·11-19·2]) polymorphisms were related to
gastrointestinal toxicity and infection, respectively. During the consolidation phase, when
antifolates predominated, the reduced folate carrier polymorphism predicted gastrointestinal
toxicity (OR 10·4 [1·35-80·4]) as it also did during continuation (OR 2·01 [1·06-4·11]). In all
three treatment phases, a glucuronosyltransferase polymorphism predicted hyperbilirubinemia
(p = 0·017, < 0·0001, and < 0·0001, respectively) and methotrexate clearance (p = 0·028),
which was also independently associated with hyperbilirubinemia (p = 0·026). The genotypephenotype associations were similar whether analyses were adjusted by self-reported race or
ancestry-informative genetic markers. Germline polymorphisms are significant determinants
of toxicity of antileukemic therapy.
2
From www.bloodjournal.org by guest on March 6, 2016. For personal use only.
Introduction
Acute lymphoblastic leukemia (ALL) is cured in approximately 80% of children with multiagent
chemotherapeutic regimens.1-4 Treatment-related toxicity cannot only be life-threatening 5,6 but
is also one of the main reasons for interruption or discontinuation of chemotherapy, which may
increase relapse risk. Moreover, adverse events affect the quality of life for patients during
and after cancer therapy.7-10 Prediction of toxicity is difficult, because of wide interpatient
variation in pharmacokinetics and pharmacodynamics of antileukemic agents. A trial-and-error
approach to dosing is not optimal due to delay between dosing and toxicity, and because the
same toxicity (e.g. myelosuppression) can be attributable to multiple drugs.
The extent to which genetic predisposition influences risk of common toxicities is not clear.
Toxicity from anticancer drugs can be affected by inherited polymorphisms in genes that
encode drug-metabolizing enzymes, transporters, targets, and receptors.11-14 Although we and
others have assessed whether germline polymorphisms relate to antileukemic agent toxicity,
15-18
most prior studies have focused on few polymorphisms and very specific toxicities, and
did not assess the influence of gene-gene interactions. Moreover, many studies failed to
account for confounding factors such as age, sex, race, and differences in chemotherapeutic
regimens.9,19-21
Herein, we used a candidate-gene approach, adjusting for confounding factors, to determine
whether all common therapy-induced toxicities (gastrointestinal toxicity, infection,
hyperbilirubinemia, and neurotoxicity) were related to 16 common polymorphisms in genes
involved in the pharmacodynamics of ALL therapy. We also assessed whether pathwayoriented groupings of these genetic polymorphisms were useful. These results are interpreted
in the context of our prior analysis of genes influencing relapse risk.22
3
From www.bloodjournal.org by guest on March 6, 2016. For personal use only.
Methods
Patients
Of 247 children with newly diagnosed ALL treated on the Total XIIIB study 23 at St. Jude
Children's Research Hospital, 240 were evaluable herein. We excluded one patient who died
shortly after diagnosis and did not have a remission DNA sample; five patients with Down
syndrome and one patient with cystic fibrosis because their underlying diseases can influence
toxicity.24,25 The study was approved by St. Jude Children’s Research Hospital’s Institutional
Review Board, and informed consent was obtained from parents, guardians, or patients (as
appropriate). Patients were prospectively assigned to one of two treatment groups based upon
relapse risk (lower or higher/intermediate). Of the 240 evaluable patients, 3 patients came off
study due to toxicity; 30 patients were censored prior to the end of treatment because of
relapse (n=8), second cancer (n=3), stem cell transplantation (n=3), induction failure (n=3) and
other reasons (n=13). However, for each treatment phase, all patients were included in the
analysis up to time of censoring.
Upon admission, patients (or their parents) were asked to declare their “race” according to
institutional guidelines including black, white, Asian and other. Therapy was divided into three
phases: 8 weeks of remission induction, 2 weeks of consolidation, and 120 weeks of
continuation therapy (including a reinduction phase at weeks 16-21) as described.23
Remission induction consisted of “window” therapy with mercaptopurine, alone or combined
with low- or high-dose methotrexate, followed 4 days later by prednisone, vincristine,
daunorubicin, asparaginase, cytarabine, and etoposide. Consolidation treatment comprised
high-dose methotrexate and mercaptopurine. Continuation treatment differed by risk groups:
the lower-risk arm received mercaptopurine plus methotrexate with pulses of dexamethasone
plus vincristine; the higher-risk arm received drug pairs rotating weekly: etoposide plus
cyclophosphamide, mercaptopurine plus methotrexate, methotrexate plus cytarabine,
4
From www.bloodjournal.org by guest on March 6, 2016. For personal use only.
dexamethasone plus vincristine, and etoposide plus cytarabine. Patients at higher risk of
central-nervous-system relapse received extra intrathecal therapy and cranial irradiation at
week 56-57 of continuation treatment. Methotrexate plasma clearance was estimated following
each course of high-dose methotrexate (http://pharmgkb.org, PA134711664), leucovorin
dosage was adjusted based on plasma methotrexate concentrations as described, 26 and the
per-patient average clearance during consolidation and continuation treatment was analyzed.
Standard supportive care included the use of three-day-a-week oral
trimethoprim/sulfamethoxazole as the only antimicrobial prophylaxis and ondansetron as the
primary antiemetic; use of filgrastim and antifungal prophylaxis was rare.
Toxicities
Toxicities were graded using NCI Common Toxicity Criteria version 1.0 and included the most
common toxicities: gastrointestinal (stomatitis or diarrhea), infection, hyperbilirubinemia, and
neurotoxicity (Table 1). For analyses, toxicity grades were used to dichotomize toxicities as
“present” versus “absent” with grade 3-4 or grade 2-3 toxicities considered as present,
depending on phase, as defined in Table 1. Neurotoxicity was divided into vincristine-related
peripheral neuropathy (e.g., constipation, neurosensory, and neuromotor) or methotrexaterelated central nervous system toxicity (cerebellar or cortical).
For remission induction, time at risk was from beginning of therapy until start of consolidation
treatment. For consolidation phase, time at risk was from the start of consolidation until 4
weeks after completion of consolidation, or until start of continuation therapy, whichever came
first. During these two phases, if a patient experienced multiple episodes of the same toxicity,
the highest grade for that phase was used in the analysis. For toxicity occurring during
continuation treatment, time at risk was from the beginning of continuation until 2 weeks after
5
From www.bloodjournal.org by guest on March 6, 2016. For personal use only.
the end of therapy. Patients were censored at time of withdrawal from protocol treatment for
any reason.
Genotyping
DNA was extracted from normal blood cells using samples that were collected after the
successful completion of remission induction in nearly all cases. Polymorphisms in candidate
genes encoding proteins involved in pharmacokinetics or pharmacodynamics of antileukemic
agents (Figure 1) have previously been linked to a functional phenotype in vivo or in vitro;
genotyping for 16 polymorphic loci [CYP3A4*1B (A>G at position -392) and CYP3A5*3 (G>A
at position 22893); GSTP1 313A>G, GSTM1 deletion, GSTT1 deletion, MDR1 exon 21
(2677G>T/A), MDR1 exon 26 (3435C>T), MTHFR 677C>T, MTHFR 1298A>C, NR3C1
1088A>G, RFC (SLC19A1) 80A>G, TPMT ( 238G>C, 460G>A, 719A>G), TYMS enhancer
repeat, UGT1A1 promoter repeat, VDR intron 8 G>A, and VDR FokI (start site) T>C] was
performed as described 22 and was 100 percent successful.
Ancestry-informative markers (AIMs) were genotyped by DNAPrint Genomics (Sarasota, FL),
and used 176 autosomal genetic markers with large allele frequency differences between
populations to estimate the biogeographical ancestry for each individual. The results are
reported as estimated percentage of Sub-Saharan African, European, Native American and
East Asian.27 (Figure 2)
Statistical analysis
Genotypes for each polymorphic locus were placed in binary groups for statistical analysis as
described.22 The percentage of patients in the less common genotypic group at each locus
ranged from 3·3 to 48·8 percent (median 31·7 percent, Table 2). Except for the continuation
phase, toxicity was regarded as a dichotomous variable. Exact Chi-square tests were used to
6
From www.bloodjournal.org by guest on March 6, 2016. For personal use only.
examine the association between self-reported or AIMs-determined race, age, or upfront
treatment-arm categories (mercaptopurine, mercaptopurine plus high-dose methotrexate,
mercaptopurine plus low-dose methotrexate, or none) and each type of toxicity. Fisher’s Exact
tests were used to examine the association between sex (142 male, 98 female) or risk
category (126 on lower-risk vs. 114 higher risk) and each toxicity. Self-reported race was
divided into 4 categories: whites (n = 167), blacks (n = 44), Asian (n=1) and others (n = 28);
race determined by AIMs was reported as a percentage of 4 categories for each patient: SubSaharan African, European, Native American and East Asian; age was treated as 3
categories: less than 1 (n=10), 1 to 10 (n=159) and over 10 years old (n=71).
For the induction and consolidation period, logistic regression was used to test whether toxicity
was related to each genotype. For the continuation period, each toxicity event was assumed to
be independent, and weighted logistic regression was applied to test the association between
genotype and each toxicity event. Because the duration of continuation therapy was
extensive, time-at-risk for toxicity was considered. Each episode of toxicity was weighted
according to the patient’s duration of risk for toxicity by the following formula:
Wi =
Zi
max( Z i )
1−tox
,
where Zi is cumulative incidence of toxic episodes (of a given type) at time of the ith episode or
at the time of censoring, tox=1 if Zi corresponds to a toxicity episode, and tox=0 otherwise.
Preliminary analyses revealed that some toxicities differed by treatment group or demographic
factors (Supplemental Table 1). Because some of these factors could be confounded by
genotypes 28, we performed analyses that did (multivariate) and did not (univariate – see
Supplemental Tables 2-4) adjust for demographic factors and risk groups; only the multivariate
7
From www.bloodjournal.org by guest on March 6, 2016. For personal use only.
results are presented in the main manuscript. In the multivariate analysis, we used multiple
logistic regression with treatment groups and demographic factors as covariates.
To investigate whether multigenic genotypes predicted toxicities, we categorized the
polymorphisms into 3 functional pathways (Figure 1); glucocorticoid-related genes (CYP3A,
MDR1, NR3C1, VDR), phase II conjugating enzyme genes (GSTs, UGT1A1), and
antimetabolite-related genes (MTHFR, RFC, TPMT, TYMS), and we defined high, medium and
low “activity” for each of these three pathway groupings (Supplemental Table 5). We
performed multivariate weighted logistic regression, adjusting for age, sex, treatment groups,
and race, to test whether multi-gene genotypes affected toxicity.
The stepdown Bonferroni method of Holm was used to assess the statistical significance of the
correlations among genotypes.29 The log rank test was used to compare the cumulative
incidence of toxicity by genotypic groups. A linear or logistic regression model was used to
assess the association between genotypes and methotrexate clearance or between toxicity
and methotrexate clearance, respectively.
8
From www.bloodjournal.org by guest on March 6, 2016. For personal use only.
Results
Self-reported vs AIMs determined race.
Because both genotypes 22 and some toxicities (Supplemental Table 1) differed by race, we
further refined assessment of race using percent of biogeographical ancestry based on AIMs
(Figure 2). The relationships between candidate genotypes and toxicity were essentially
identical whether adjusting for self-reported race or % ancestry by AIMs (Table 3); hence the
odds ratios and p-values reported below are adjusted for self-reported race.
Remission induction.
Multiple (eight) drugs were given and many toxicities were observed over the 8-week period
(Table 1). Accordingly, different genotypes were associated with each toxicity: GSTT1 null and
VDR intron 8 GG genotypes were significantly associated with gastrointestinal toxicity;
CYP3A5, RFC and VDR intron 8 polymorphisms with infection; and GSTM1, UGT1A1, VDR
FokI and VDR intron 8 polymorphisms with hyperbilirubinemia (Table 3, Figure 3).
Consolidation.
Only antimetabolites (methotrexate and mercaptopurine) were given, and the most common
toxicities were gastrointestinal and hyperbilirubinemia (Table 1). The RFC 80A allele, a
polymorphism in the methotrexate uptake transporter, was the only genotype significantly
associated with gastrointestinal toxicity, and the UGT1A1 7/7 genotype was highly predictive
for hyperbilirubinemia (Table 3, Figures 3 and 4), as in remission induction. When genotypes
were combined into three pathway-directed functional groups (defined in Figure 1,
Supplemental Table 5), the antimetabolite pathway group was related to gastrointestinal
toxicity (overall p =0·0058), whereas the phase II conjugating enzyme group was highly
9
From www.bloodjournal.org by guest on March 6, 2016. For personal use only.
(overall p = 0·0015) and the glucocorticoid group was weakly related to hyperbilirubinemia
(overall p = 0·047) (Supplemental Table 6).
Continuation.
Multiple agents were given over 120 weeks, but glucocorticoid use was less intensive than
during remission induction. The UGT1A1 polymorphism remained the strongest predictor
(odds ratio 17·0, p < 0·0001) of hyperbilirubinemia (Table 3, Figure 3), as during induction and
consolidation; incidence of first episode of hyperbilirubinemia was strongly related (p < 0·001)
to UGT1A1 genotype (Figure 4). The CYP3A5 and VDR intron 8 polymorphisms were
associated with peripheral neurotoxicity and the GSTP1 GG genotype with central nervous
system toxicity (Table 2). The RFC 80 A allele continued to significantly associate with
gastrointestinal toxicity as during consolidation (Table 3, Figures 3 and 4). With genotypes
combined into pathway-directed functional groups, the phase II conjugating enzyme group
genotype was related to hyperbilirubinemia (overall p = 0·0007) and to central nervous system
toxicity (overall p = 0·0269), and the glucocorticoid group genotype was associated with
peripheral neurotoxicity (overall p = 0·0235) (Supplemental Table 6).
Methotrexate pharmacokinetics.
The only antileukemic agent for which pharmacokinetic data were available for all patients was
high-dose methotrexate, given twice during consolidation and up to 8 times during
continuation. In univariate logistic regression analyses, the only toxicities significantly related
to methotrexate clearance were gastrointestinal toxicity (p = 0·044) and hyperbilirubinemia
during the continuation phase (p = 0·0001), although only the latter was significant in a
multivariate analysis (p = 0·0262), with average methotrexate clearance lower (92·0 ± 22·2
ml/min/m2) among patients who experienced hyperbilirubinemia than among those who did not
(113·4 ± 24·4 ml/min/m2) (Supplemental Figure 1). Methotrexate clearance significantly
10
From www.bloodjournal.org by guest on March 6, 2016. For personal use only.
predicted hyperbilirubinemia even after adjusting for UGT1A1 genotype (p = 0·0240). Average
methotrexate clearance was lower (102·5 ± 24·0 ml/min/m2) among patients with the loweractivity UGT1A1 7/7 genotype than those with other UGT1A1 genotypes (113·6 ± 24·9
ml/min/m2; p = 0·0284) (Supplemental Figure 1). The UGT1A1 7/7 genotype significantly
predicted hyperbilirubinemia (p = 0·0003) even after adjusting for methotrexate clearance.
Methotrexate clearance did not differ between patients with RFC AA/AG and GG genotypes
(112·7 vs 113·3 ml/min/m2, p = 0·93).
Genotype Correlations.
To test whether association of genotypes with toxicities was confounded by associations
among genotypes, we assessed correlations among genotypes at the 16 loci. Other than the
expected linkage disequilibrium within some loci (e.g., CYP3A4 with CYP3A5; MDR1 exon 21
with MDR1 exon 26 polymorphisms), the only genotypes correlated were the MDR exon 21
and CYP3A4 polymorphisms (p < 0·001) (Supplemental Table 7). However, these two loci
were not associated with toxicities in this analysis, and when gene-gene interactions were
assessed separately within racial groups, there was no association between the two
polymorphic loci (p = 1·00 in whites).
11
From www.bloodjournal.org by guest on March 6, 2016. For personal use only.
Discussion
In this comprehensive pharmacogenetic study of patients with leukemia, several inherited
polymorphisms were significantly related to toxicity of antileukemic therapy. Of particular
interest are polymorphisms related to toxicity during more than one phase of therapy, those
that predicted more than one type of toxicity (Figure 3), and those that could be related to
pharmacokinetics of specific medications.30,31
We found that RFC genotype was associated with infection and gastrointestinal toxicity (Table
3); patients harboring the A allele exhibiting a substantial increase in incidence of
gastrointestinal toxicity (Figures 3 and 4). RFC codes for a membrane transporter responsible
for cellular uptake of reduced folate and methotrexate.32 Prior experimental work has failed to
yield an unequivocal functional consequence resulting from the G to A nonsynonymous
substitution at position 80,33,34 although several clinical studies corroborate findings of
enhanced toxicity associated with the A allele. Although it has been reported that patients with
the RFC AA genotype have higher plasma methotrexate concentrations than those with the
AG or GG genotype,35 our data did not corroborate that finding. While these results indicate a
potential role for this RFC SNP in toxicity for patients on this protocol, we acknowledge that
such genotype/phenotype associations could be complicated by other folate-related
polymorphisms, the regimen of leucovorin rescue relative to the methotrexate exposure, and
the indirect effects of the RFC on folate and purine/pyrimidine homeostasis.
The strongest predictor of hyperbilirubinemia was the UGT1A1 promoter-repeat polymorphism
(Table 3, Figures 3 and 4). Bilirubin is a substrate for UGT1A1, and the promoter-repeat
polymorphism predicts hyperbilirubinemia even in the absence of drug challenge.36,37
However, in the presence of drug challenge, bilirubin concentrations could conceivably be
12
From www.bloodjournal.org by guest on March 6, 2016. For personal use only.
even higher, especially in patients with the low activity UGT1A1 7/7 genotype. In fact, we
found that patients with low methotrexate clearance were at higher risk of hyperbilirubinemia
(Supplemental Figure 1), and because both methotrexate clearance and UGT1A1
polymorphism predicted hyperbilirubinemia, it is possible that higher concentrations of both
bilirubin and methotrexate could be due to lower clearance of both, by virtue of each
interacting with UGT1A1. This is consistent with a report that methotrexate can inhibit
glucuronidation.38 Thus, lower UGT1A1 activity could directly result in hyperbilirubinemia due
to reduced bilirubin conjugation, and also indirectly by resulting in higher plasma methotrexate,
which could competitively inhibit bilirubin conjugation and excretion.
The VDR intron 8 polymorphism has been associated with several clinical phenotypes,19;39-41
directly or through regulation of CYP3A42 or p-glycoprotein, but has not previously been
associated with the toxicities reported here. We found that VDR intron 8 GG genotype was
related to gastrointestinal toxicity and infection during induction (Table 3). In contrast, there
was no association between VDR polymorphisms and toxicities during consolidation, when
only antimetabolites were used. VDR effects on other “glucocorticoid” pathway genes
(CYP3A, MDR1, and NR3C1) are complicated when glucocorticoids are given along with
other CYP3A/MDR1 substrates during the remission induction phase, because glucocorticoids
are potent enhancers of plasma clearance of antileukemic agents (Figure 1),41 which may
function as both substrates and inhibitors of CYP3A. Thus, if a polymorphism causes
decreased CYP3A activity, this may decrease clearance for most CYP3A substrates (e.g.,
vincristine, etoposide and daunorubicin) but that may be countered by greater exposure to
glucocorticoid, which increases clearance of CYP3A substrates. Hence, that the VDR intron 8
GG genotype was associated with greater toxicity during remission induction but lower toxicity
during the continuation phase (Table 3) could be because steroids are given continuously
during remission induction but not in continuation. Similar considerations may explain why the
13
From www.bloodjournal.org by guest on March 6, 2016. For personal use only.
“low activity” CYP3A5 G allele was associated with higher risk of toxicity during induction but
with lower risk during continuation (Table 3).
The toxicities we analyzed were the most common we observed that included grades 3 and 4,
but not all toxicities were dose-limiting. For example, hyperbilirubinemia or peripheral
neuropathy rarely influenced delivery of therapy, whereas severe infection or mucositis
generally resulted in therapy delays. Other ALL studies that emphasize other medications are
likely to result in identification of alternative predictive polymorphisms, and both alternative
candidate gene and genome-wide strategies to assess germline genotype effects on toxicity
are likely to identify additional predictive genotypes.
It has been suggested that a series of polymorphisms within pathways may be more predictive
of pharmacologic phenotypes than single gene loci. To address this, we clustered
polymorphisms into 3 functional groups (Figure 1, Supplemental Table 5). However these
multigenic “pathway” genotypes were no more informative than the strongest individual loci
(compare Supplemental Table 6 to Table 3). It is possible that genotypes for polymorphisms
in some genes have evolved to “compensate” for dysfunction in other genes. That MDR1 and
CYP3A polymorphisms are significantly associated with each other when all racial groups are
combined, and that multigenic pathways are not more predictive of toxicity than single loci,
support our hypothesis that human polymorphisms tend to act to “cancel each other out” rather
than necessarily accentuating inter-individual phenotypic differences.
Inactivating polymorphisms in TPMT12 were not associated with toxicity in this study, as they
were in our prior clinical trial.43 This is because the current study included algorithms for
prospectively measuring TPMT status and adjusting mercaptopurine dosages downward in all
children with at least one TPMT non-functional allele and evidence of myelosuppression. This
14
From www.bloodjournal.org by guest on March 6, 2016. For personal use only.
illustrates the potential clinical benefit of prospectively adjusting chemotherapy based on
genotypes that have been definitively linked to risk of specific adverse drug effects. In this
regard, new genotype/phenotype associations identified in the current study could also lead to
less toxicity once translated into routine clinical use in future protocols.
It has been shown that population genetic structure may confound candidate genotypephenotype association studies.44,45 The improvement in defining genotype vs phenotype
relationships likely depends upon the mechanistic basis for confounding by race, the
“accuracy” of self-reported race, as well as racial composition of the group. In this study, the
more refined assessment of race made possible by genotyping at 176 markers (n=240) did not
alter our genotype vs toxicity findings compared to adjusting for self-reported race, perhaps
because of high concordance (Figure 2) between genetically-assessed and self-reported race
in this cohort.
How should these polymorphisms that affect toxicity be interpreted in the context of their
effects on relapse risk? In this protocol, the strongest predictors of hematologic relapse were
the higher-activity GSTM1 non-null and the TYMS 3/3 genotypes.22 Fortunately, we found that
neither of these polymorphisms was associated with toxicity. Our results raise the possibility
that one may be able to identify pharmacogenetic profiles for patients in whom increased
dosages may be warranted to decrease risk of relapse, and others in whom decreased
dosages may be necessary to decrease risk of toxicity. Further studies including patients on
alternative chemotherapeutic regimens would be beneficial to enhance the observations
herein, as it is likely that additional predictive genotypes may be elucidated by future candidate
gene or genome-wide studies.
15
From www.bloodjournal.org by guest on March 6, 2016. For personal use only.
We conclude that germline polymorphisms in candidate genes plausibly linked to the
pharmacodynamics of antileukemic therapy influence risk of toxicity during this therapy.
Eventually, individualizing dosages based partly on inherited genetic predisposition holds
promise as a strategy to minimize risk of serious toxicity without compromising efficacy.
Acknowledgements
We thank our protocol co-investigators, clinical and research staff, and the patients and their
families for their participation. This work was supported by NCI CA 51001, CA 78224,
CA21765 and the NIH/NIGMS Pharmacogenetics Research Network and Database (U01
GM61393, U01GM61374 http://pharmgkb.org/ PS206362) from the National Institutes of
Health; by a Center of Excellence grant from the State of Tennessee; and by American
Lebanese Syrian Associated Charities (ALSAC). C-H Pui is the American Cancer Society F.M.
Kirby Clinical Research Professor.
Conflict of interest statement: None declared.
M.V.R. and W.E.E. conceived the project.
C.H-P. is a principal investigator of the leukemia trials and supervised clinical data collection.
N.H. reviewed cases of neurotoxicity.
C.C., D.P, and G.L.R. carried out and interpreted the statistical analyses.
T.F. carried out the AIMs genotyping.
S.D., E.H.C. and C.R. performed genotyping.
S.K. and D.F. interpreted the data and were primary authors.
All the investigators contributed to the writing of the paper.
16
From www.bloodjournal.org by guest on March 6, 2016. For personal use only.
Reference List
1.
Nachman JB, Sather HN, Sensel MG et al. Augmented post-induction therapy
for children with high-risk acute lymphoblastic leukemia and a slow response to initial therapy.
N.Engl.J.Med. 1998;338:1663-1671.
2.
Pui CH, Relling MV, Downing JR. Acute lymphoblastic leukemia. N.Engl.J.Med.
2004;350:1535-1548.
3.
Schrappe M, Camitta B, Pui CH et al. Long-term results of large prospective
trials in childhood acute lymphoblastic leukemia. Leukemia 2000;14:2193-2194.
4.
Silverman LB, Gelber RD, Dalton VK et al. Improved outcome for children with
acute lymphoblastic leukemia: results of Dana-Farber Consortium Protocol 91-01. Blood
2001;97:1211-1218.
5.
Rivera GK, Evans WE, Kalwinsky DK et al. Unexpectedly severe toxicity from
intensive early treatment of childhood lymphoblastic leukemia. J.Clin.Oncol. 1985;3:201-206.
6.
Winick NJ, Bowman WP, Kamen BA et al. Unexpected acute neurologic toxicity
in the treatment of children with acute lymphoblastic leukemia. J.Natl.Cancer Inst.
1992;84:252-256.
7.
Gunnars B, Nygren P, Glimelius B. Assessment of quality of life during
chemotherapy. Acta Oncol. 2001;40:175-184.
8.
Pui CH, Cheng C, Leung W et al. Extended follow-up of long-term survivors of
childhood acute lymphoblastic leukemia. N.Engl.J Med. 2003;349:640-649.
9.
Lipshultz SE, Lipsitz SR, Mone SM et al. Female sex and drug dose as risk
factors for late cardiotoxic effects of doxorubicin therapy for childhood cancer. N.Engl.J.Med.
1995;332:1738-1743.
17
From www.bloodjournal.org by guest on March 6, 2016. For personal use only.
10.
Meadows AT, Robison LL, Neglia JP, Sather H, Hammond D. Potential long-
term toxic effects in children treated for acute lymphoblastic leukemia. N.Engl.J.Med.
1989;321:1830-1831.
11.
Evans WE, McLeod HL. Pharmacogenomics--drug disposition, drug targets,
and side effects. N.Engl.J.Med. 2003;348:538-549.
12.
Weinshilboum R. Inheritance and drug response. N.Engl.J.Med. 2003;348:529-
13.
Diasio RB, Beavers TL, Carpenter JT. Familial deficiency of dihydropyrimidine
537.
dehydrogenase. Biochemical basis for familial pyrimidinemia and severe 5- fluorouracilinduced toxicity. J.Clin.Invest. 1988;81:47-51.
14.
Iyer L, King CD, Whitington PF et al. Genetic predisposition to the metabolism
of irinotecan (CPT-11). Role of uridine diphosphate glucuronosyltransferase isoform 1A1 in the
glucuronidation of its active metabolite (SN-38) in human liver microsomes. J.Clin.Invest.
1998;101:847-854.
15.
Kishi S, Griener JC, Cheng C et al. Homocysteine, pharmacogenetics, and
neurotoxicity in children with leukemia. J Clin Oncol 2003;21:3084-3091.
16.
Aplenc R, Glatfelter W, Han P et al. CYP3A genotypes and treatment response
in paediatric acute lymphoblastic leukaemia. Br.J.Haematol. 2003;122:240-244.
17.
Naoe T, Tagawa Y, Kiyoi H et al. Prognostic significance of the null genotype of
glutathione S- transferase-T1 in patients with acute myeloid leukemia: increased early death
after chemotherapy. Leukemia 2002;16:203-208.
18.
Stanulla M, Schaeffeler E, Flohr T et al. Thiopurine methyltransferase (TPMT)
genotype and early treatment response to mercaptopurine in childhood acute lymphoblastic
leukemia. JAMA 2005;293:1485-1489.
19.
Relling MV, Yang W, Das S et al. Pharmacogenetic risk factors for
osteonecrosis of the hip among children with leukemia. J Clin Oncol 2004;22:3930-3936.
18
From www.bloodjournal.org by guest on March 6, 2016. For personal use only.
20.
Arndt C, Hawkins D, Anderson JR et al. Age is a risk factor for chemotherapy-
induced hepatopathy with vincristine, dactinomycin, and cyclophosphamide. J Clin.Oncol.
2004;22:1894-1901.
21.
Stoneham S, Lennard L, Coen P, Lilleyman J, Saha V. Veno-occlusive disease
in patients receiving thiopurines during maintenance therapy for childhood acute lymphoblastic
leukaemia. Br.J.Haematol. 2003;123:100-102.
22.
Rocha JC, Cheng C, Liu W et al. Pharmacogenetics of outcome in children with
acute lymphoblastic leukemia. Blood 2005;105:4752-4758.
23.
Pui CH, Sandlund JT, Pei D et al. Improved outcome for children with acute
lymphoblastic leukemia: results of Total Therapy Study XIIIB at St Jude Children's Research
Hospital. Blood 2004;104:2690-2696.
24.
Gururangan S, Horner M, Rodman JH, Marina NM. Successful treatment of
acute lymphoblastic leukemia in a child with cystic fibrosis. Med.Pediatr.Oncol. 1994;22:414416.
25.
Ravindranath Y. Down syndrome and leukemia: new insights into the
epidemiology, pathogenesis, and treatment. Pediatr.Blood Cancer 2005;44:1-7.
26.
Rubnitz JE, Relling MV, Harrison PL et al. Transient encephalopathy following
high-dose methotrexate treatment in childhood acute lymphoblastic leukemia. Leukemia
1998;12:1176-1181.
27.
Frudakis T, Thomas M, Gaskin Z et al. Sequences associated with human iris
pigmentation. Genetics 2003;165:2071-2083.
28.
Burchard EG, Ziv E, Coyle N et al. The importance of race and ethnic
background in biomedical research and clinical practice. N.Engl.J Med. 2003;348:1170-1175.
29.
1979;6:65-70.
19
Holm S. A simple sequentially rejective multiple test procedure. Scan J Stat
From www.bloodjournal.org by guest on March 6, 2016. For personal use only.
30.
Evans WE, Relling MV. Pharmacogenomics: translating functional genomics
into rational therapeutics. Science 1999;286:487-491.
31.
Relling MV, Dervieux T.
Pharmacogenetics and cancer therapy. Nature
Reviews Cancer 2001;1:99-108.
32.
Goldman ID, Matherly LH. The cellular pharmacology of methotrexate.
Pharmacol Ther. 1985;28:77-102.
33.
Whetstine JR, Gifford AJ, Witt T et al. Single nucleotide polymorphisms in the
human reduced folate carrier: characterization of a high-frequency G/A variant at position 80
and transport properties of the His(27) and Arg(27) carriers. Clin.Cancer Res 2001;7:34163422.
34.
Chango A, Emery-Fillon N, de Courcy GP et al. A polymorphism (80G->A) in
the reduced folate carrier gene and its associations with folate status and homocysteinemia.
Mol Genet.Metab 2000;70:310-315.
35.
Laverdiere C, Chiasson S, Costea I, Moghrabi A, Krajinovic M. Polymorphism
G80A in the reduced folate carrier gene and its relationship to methotrexate plasma levels and
outcome of childhood acute lymphoblastic leukemia. Blood 2002;100:3832-3834.
36.
Bosma PJ, Chowdhury JR, Bakker C et al. The genetic basis of the reduced
expression of bilirubin UDP-glucuronosyltransferase 1 in Gilbert's syndrome. N.Engl.J Med.
1995;333:1171-1175.
37.
Monaghan G, Ryan M, Seddon R, Hume R, Burchell B. Genetic variation in
bilirubin UPD-glucuronosyltransferase gene promoter and Gilbert's syndrome. Lancet
1996;347:578-581.
38.
Rajaonarison JF, Lacarelle B, Catalin J, Durand A, Cano JP. Effect of
anticancer drugs on the glucuronidation of 3'-azido-3'-deoxythymidine in human liver
microsomes. Drug Metab Dispos. 1993;21:823-829.
20
From www.bloodjournal.org by guest on March 6, 2016. For personal use only.
39.
Sainz J, Van Tornout JM, Loro ML et al. Vitamin D-receptor gene
polymorphisms and bone density in prepubertal American girls of Mexican descent .
N.Engl.J.Med. 1997;337:77-82.
40.
Morrison NA, Qi JC, Tokita A et al. Prediction of bone density from vitamin D
receptor alleles. Nature 1994;367:284-287.
41.
Kishi S, Yang W, Boureau B et al. Effects of prednisone and genetic
polymorphisms on etoposide disposition in children with acute lymphoblastic leukemia. Blood
2004;103:67-72.
42.
Thummel KE, Brimer C, Yasuda K et al. Transcriptional control of intestinal
cytochrome P-4503A by 1alpha,25- dihydroxy vitamin D3. Mol.Pharmacol. 2001;60:13991406.
43.
Relling MV, Hancock ML, Rivera GK et al. Mercaptopurine therapy intolerance
and heterozygosity at the thiopurine S-methyltransferase gene locus. J.Natl.Cancer Inst.
1999;91:2001-2008.
44.
Choudhry S, Coyle NE, Tang H et al. Population stratification confounds
genetic association studies among Latinos. Hum.Genet. 2006;118:652-664.
45.
Hoggart CJ, Parra EJ, Shriver MD et al. Control of confounding of genetic
associations in stratified populations. Am.J.Hum.Genet. 2003;72:1492-1504.
21
From www.bloodjournal.org by guest on March 6, 2016. For personal use only.
Figure legends
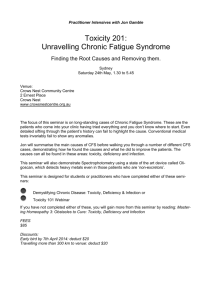
Figure 1: The interactions of antileukemic agents with gene products. Antileukemic
agents (dashed boxes) interact with gene products typed in this study (genes italicized, with
their functions indicated in the colored boxes). Bidirectional arrows indicate that the drugs are
both substrates for and competitive inhibitors of the indicated gene products; dashed arrow
indicates inductive effect of steroids on CYP3A enzymes; flat-headed arrows indicate inhibitory
effects. Genotypes were determined at loci in the indicated genes and analyzed individually;
they were also pooled into one of three major groups: glucocorticoid (green), phase II
conjugating blue), and antimetabolite-related (red).
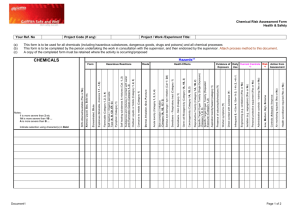
Figure 2: Concordance of self-reported and AIMs determined race. Percentage of SubSaharan African, European, Native American and East Asian ancestry as determined by AIMs
(y-axes) plotted by self-reported race categories (x-axes); black, n= 44; white, n=167; Asian,
n=1 and other, n=28. Boxes indicate quartiles, horizontal bars indicate medians and whiskers
indicate the range after excluding outliers (circles).
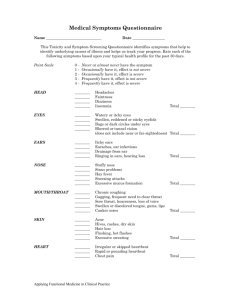
Figure 3: Odds ratios of experiencing toxicity during therapy. Median (95 percent
confidence intervals) odds ratios of experiencing the indicated toxicity for the three phases of
therapy for the most predictive genotypes. Odds ratios resulting from multivariate analyses
using self-declared race. The genotypes depicted were significantly associated with more
than one toxicity or with toxicity in more than one phase of therapy.
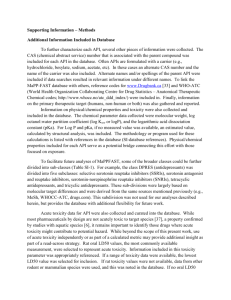
Figure 4: Incidence of toxicity based on specific genotypes. Cumulative incidence of the
first episode of grade 3-4 gastrointestinal (GI) toxicity differing (p=0.014) by RFC genotypes
during therapy (top). Cumulative incidence of the first episode of grade 3-4 hyperbilirubinemia
differing (p < 0·001) by UGT1A1 genotypes, during therapy (bottom).
22
From www.bloodjournal.org by guest on March 6, 2016. For personal use only.
Figure 1
From www.bloodjournal.org by guest on March 6, 2016. For personal use only.
Figure 2
From www.bloodjournal.org by guest on March 6, 2016. For personal use only.
Figure 3
From www.bloodjournal.org by guest on March 6, 2016. For personal use only.
Figure 4
Table 1. Frequencies of toxicity included in analyses by treatment phase.
Toxicity
Central nervous system
Hyper-
GastroTreatment
toxicity
Bilirubinemia
intestinal
Phase
Toxicity
3
4
3
4
2
14
2
28
7
16
3
7
0
61
9
97
21
3
4
2
3
4
2
3
4
49 17
6
_
8
0
0*
2*
0*
21 5
0
3*
1*
0*
0*
2*
0*
43
1
7
23
(6)
(13)
Grade
Induction,
total number
of patients#
with toxicity
Consolidation,
total number
of patients#
with toxicity
Continuation,
total number
59
12
of episodes
(patients#)
(41)
(7)
(62)
(18)
(34)
(9)
(29)
(1)
From www.bloodjournal.org by guest on March 6, 2016. For personal use only.
Peripheral neuropathy
Infection
Continuation,
total number
of episodes of
week at risk
0.002866 0.000423 0.004558 0.000987 -
0.00277 0.0005 0.004981 0.0020 0.00004 0.00004 0.0003 0.00108
0.001926 0.000329 0.002913 0.000846 -
0.00159 0.0004 0.002772 0.0013 0.00004 0.00004 0.0002 0.00108
Continuation, total
number of patients
with toxicity per
week at risk
From www.bloodjournal.org by guest on March 6, 2016. For personal use only.
toxicity per
From www.bloodjournal.org by guest on March 6, 2016. For personal use only.
# The number of patients or episodes of toxicity analyzed, broken down by NCI grade and
phase: e.g. for hyperbilirubinemia during induction or consolidation, grade 2, 3, and 4 episodes
were considered as toxic, whereas for continuation, only grade 3 and 4 episodes were
considered as toxic for purposes of the analyses. The total numbers of the patients at risk
were 240, 239, and 237 during the induction, consolidation and continuation phases,
respectively. *not analyzed statistically because of too few events.
From www.bloodjournal.org by guest on March 6, 2016. For personal use only.
Table 2. Percentage of the 240 patients falling into the two primary genotypic groups at each
of 16 loci.
locus
% in 1st
% in 2nd genotype
genotype group
group
genotype groups
CYP3A4*1B
AA vs. AG and GG
79.6
20.4
CYP3A5*3
AA and AG vs. GG
32.1
67.9
GSTM1 deletion
null vs. non-null
42.5
57.5
GSTP1 313A>G
AA and AG vs. GG
82.9
17.1
GSTT1 deletion
null vs. non-null
15.8
84.2
MDR1 exon 21 G>T/A
GG vs. others
36.7
63.3
MDR1 exon 26 C>T
CC and CT vs. TT
76.3
23.7
MTHFR 677C>T
CC vs. CT and TT
48.8
51.2
MTHFR 1298A>C
AA vs. AC and CC
53.8
46.2
NR3C1 1088A>G
AA vs. AG
96.7
3.3
RFC 80A>G
AA and AG vs. GG
68.3
31.7
TPMT combined
others vs. 238GG,
5.8
94.2
genotypes
460GG and 719AA
3AND3 vs. others
31.7
68.3
7AND7 vs. others
10.4
87.9
VDR FokI T>C
CC vs. CT and TT
46.3
53.7
VDR intron8 G>A
AA and AG vs. GG
54.2
45.8
TYMS enhancer
repeat
UGT1A1 promoter
repeat
From www.bloodjournal.org by guest on March 6, 2016. For personal use only.
Table 3. Toxicities significantly associated with genotypes in a multivariate analysis.
Odds ratio
Toxicity
Odds ratio
(95%
p
(95%
p
confidence
value#
confidence
value+
Genotype*
limits)#
limits)+
Induction Phase
Gastrointestinal
GSTT1 null vs
4·77
non-null
(1·4-16·3)
VDR intron8 GG
6·85
vs AA or AG
(1·73-27·0)
CYP3A5 GG vs
4·61
AA or AG
(1·11-19·2)
RFC AA or AG vs
3·25
GG
(1·17-9·07)
VDR intron8 GG
3·14
vs AA or AG
(1·4-7·09)
Hyper-
GSTM1 null vs
1·95
bilirubinemia
non-null
(1·06-3·58)
UGT1A1 7/7 vs
3·05
others
(1·22-7·64)
VDR FokI CT or
1·94
TT vs CC
(1·04-3·61)
VDR intron8 GG
1·94
vs AA or AG
(1·04-3·62)
RFC AA or AG vs
10·4
GG
(1·35-80·4)
UGT1A1 7/7 vs
13·0
Infection
0·013
5·22
0·0093
(1·50-18·1)
0·006
6·67
0·0076
(1·64-25·0)
0·035
5·56
0·0192
(1·32-25·0)
0·024
3·25
0·0255
(1·16-9·13)
0·005
3·13
0·0060
(1·39-7·14)
0·032
2·00
0·0272
(1·08-3·69)
0·017
2·98
0·0199
(1·19-7·46)
0·036
2·00
0·0338
(1·05-3·70)
0·037
2·00
0·0321
(1·06-3·85)
Consolidation Phase
Gastrointestinal
Hyper-
0·025
10·7
0·0236
(1·37-82·7)
<
13·4
<
From www.bloodjournal.org by guest on March 6, 2016. For personal use only.
bilirubinemia
others
(4·1-41·3)
0·0001
(4·27-41·9)
0·0001
RFC AA or AG vs
2·01
0·033
2·03
0·0424
GG
(1·06-4·11)
Hyper-
CYP3A5 GG vs
2·67
bilirubinemia
AA or AG
(1·03-6·94)
GSTT1 non-null
4·18
vs null
(1·2-14·7)
RFC GG vs AA or
2·99
AG
(1·61-5·59)
TYMS others vs
2·08
3/3
(1·01-4·32)
UGT1A1 7/7 vs
17·0
others
(7·23-39·9)
Peripheral
CYP3A5 AA or
2·81
neurotoxicity
AG vs GG
(1·24-6·39)
VDR intron8 AA
2·22
or AG vs GG
(1·06-4·67)
Central nervous
GSTP1 GG vs AG
3·32
system
and AA
(1·41-7·81)
Continuation Phase
Gastrointestinal
(1·02-4·01)
0·044
3·13
(1·16-8·33)
0·025
4·55
0·0240
(1·22-16·7)
0·001
2·70
0·0012
(1·47-5·0)
0·048
2·22
0·0382
(1·04-4·80)
<0·0001
0·014
18·27
<
(7·82-42·7)
0·001
2·76
0·0061
(1·34-5·71)
0·035
2·16
0·0415
(1·03-4·51)
0·006
2·70
(1·18-6·25)
* first genotype listed had a higher risk of toxicity compared to the second genotype
listed
# Odds ratio and p-value for genotype predictors of toxicity adjusted for non-genetic
predictors of toxicity using self-reported race.
+ Odds ratio and p-value for genotype predictors of toxicity adjusted for non-genetic
predictors of toxicity using AIMs determined race.
0·0231
0·0201
From www.bloodjournal.org by guest on March 6, 2016. For personal use only.
Prepublished online January 30, 2007;
doi:10.1182/blood-2006-10-054528
Ancestry and pharmacogenetics of antileukemic drug toxicity
Shinji Kishi, Cheng Cheng, Deborah French, Deqing Pei, Soma Das, Edwin H. Cook, Nobuko Hijiya,
Carmelo Rizzari, Gary L. Rosner, Tony Frudakis, Ching-Hon Pui, William E. Evans and Mary V. Relling
Information about reproducing this article in parts or in its entirety may be found online at:
http://www.bloodjournal.org/site/misc/rights.xhtml#repub_requests
Information about ordering reprints may be found online at:
http://www.bloodjournal.org/site/misc/rights.xhtml#reprints
Information about subscriptions and ASH membership may be found online at:
http://www.bloodjournal.org/site/subscriptions/index.xhtml
Advance online articles have been peer reviewed and accepted for publication but have not yet
appeared in the paper journal (edited, typeset versions may be posted when available prior to
final publication). Advance online articles are citable and establish publication priority; they are
indexed by PubMed from initial publication. Citations to Advance online articles must include
digital object identifier (DOIs) and date of initial publication.
Blood (print ISSN 0006-4971, online ISSN 1528-0020), is published weekly by the American Society of
Hematology, 2021 L St, NW, Suite 900, Washington DC 20036.
Copyright 2011 by The American Society of Hematology; all rights reserved.