Medical Symptoms Questionnaire: Toxicity & Health Screening
advertisement

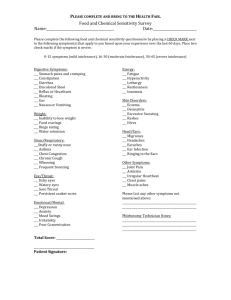
Medical Symptoms Questionnaire Name _____________________________ Date _________________ This Toxicity and Symptom Screening Questionnaire identifies symptoms that help to identify underlying causes of illness and helps us track your progress. Rate each of the following symptoms based upon your typical health profile for the past 30 days. Point Scale 0 1 2 3 4 HEAD ________ ________ ________ ________ Headaches Faintness Dizziness Insomnia EYES ________ ________ ________ ________ Watery or itchy eyes Swollen, reddened or sticky eyelids Bags or dark circles under eyes Blurred or tunnel vision (does not include near or far-sightedness) Total ________ EARS ________ ________ ________ ________ Itchy ears Earaches, ear infections Drainage from ear Ringing in ears, hearing loss Total ________ ________ ________ ________ ________ ________ Stuffy nose Sinus problems Hay fever Sneezing attacks Excessive mucus formation Total ________ ________ ________ ________ ________ ________ Chronic coughing Gagging, frequent need to clear throat Sore throat, hoarseness, loss of voice Swollen or discolored tongue, gums, lips Canker sores Total ________ ________ ________ ________ ________ ________ Acne Hives, rashes, dry skin Hair loss Flushing, hot flashes Excessive sweating Total ________ ________ ________ ________ Irregular or skipped heartbeat Rapid or pounding heartbeat Chest pain Total ________ NOSE MOUTH/THROAT SKIN HEART - Never or almost never have the symptom Occasionally have it, effect is not severe Occasionally have it, effect is severe Frequently have it, effect is not severe Frequently have it, effect is severe Applying Functional Medicine in Clinical Practice Total ________ Medical Symptoms Questionnaire LUNGS Chest congestion Asthma, bronchitis Shortness of breath Difficulty breathing Total ________ DIGESTIVE TRACT ________ ________ ________ ________ ________ ________ ________ Nausea, vomiting Diarrhea Constipation Bloated feeling Belching, passing gas Heartburn Intestinal/stomach pain Total ________ JOINTS/MUSCLE ________ ________ ________ ________ ________ Pain or aches in joints Arthritis Stiffness or limitation of movement Pain or aches in muscles Feeling of weakness or tiredness Total ________ ________ ________ ________ ________ ________ ________ Binge eating/drinking Craving certain foods Excessive weight Compulsive eating Water retention Underweight Total ________ ENERGY/ACTIVITY ________ ________ ________ ________ Fatigue, sluggishness Apathy, lethargy Hyperactivity Restlessness Total ________ MIND ________ ________ ________ ________ ________ ________ ________ ________ Poor memory Confusion, poor comprehension Poor concentration Poor physical coordination Difficulty in making decisions Stuttering or stammering Slurred speech Learning disabilities Total ________ ________ ________ ________ ________ Mood swings Anxiety, fear, nervousness Anger, irritability, aggressiveness Depression Total ________ ________ ________ ________ Frequent illness Frequent or urgent urination Genital itch or discharge WEIGHT EMOTIONS OTHER ________ ________ ________ ________ Total ________ GRAND TOTAL TOTAL _________ Add individual scores and total each group. Add each group scores for a grand total. Optimal: < 10 Mild toxicity: 10-50 Moderate toxicity: 50-100 Severe toxicity: > 100 Applying Functional Medicine in Clinical Practice