Quo Vadis Medicine… The Road Ahead for Physicians
advertisement

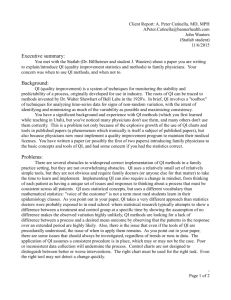
Chapter 159 Quo Vadis Medicine… The Road Ahead for Physicians E Prabhu A SHORT HISTORY OF MEDICINE • • • • • • • 2000 BC: Here, eat this root. 1000 BC: That root is heathen, say this prayer. 1850 AD: That prayer is superstition, drink this potion. 1940 AD: That potion is snake oil, swallow this pill. 1985 AD: That pill is ineffective, take this injection. 2000 AD: That injection is painful, inspire this gas. 2020 AD: That gas is toxic, here, eat this root. ~ Author Unknown “Sareere Jarjareebhute Vyaadhigraste Kalevare; Aushadam Jahnavi Toyam Vaidyo Narayano Harih.” “When the body is in the grip of disease and old age, Ganga Water is the medicine and Lord Narayana is the physician.” ~ Puranas EXECUTIVE SUMMARY The practice of medicine in India is built on time-tested principles and ethics. There is a decreased inclination toward basic medical research all along among all physicians although they are clinically strong. Newer developments are happening at a very rapid pace in the field of medicine and biology. Therefore, the society looks upon the leadership support of the physicians for their well-being. Corporatization of medicare is yet to have a significant impact on the practice of clinical medicine. The road ahead is smooth and yet challenging for all physicians. order in several parts of our country. However, the clinical skills of the physicians are challenged vigorously by the rapidly developing technology in all segments of life sciences. The social structures, economic goals and ethical values of the world are also shifting these days. Computers and Internet have fully thrown open the world of medical knowledge to everyone. Physicians, as a consequence, have developed a vision of the overall game plan in the field of biological sciences and are assuming leadership roles. Perhaps, this attitude is also due to their prolonged and rigorous training in the art of healing as well as their ardent commitment to their patients and the society. Basic scientists, technocrats, administrators, sociologists, investment bankers, economists, legal experts and philosophers—for every one in the society are keen to become a principal stakeholder in the field of health care. Therefore, medicine would still continue to attract the best of talents in our society.2 WHAT MAKES PHYSICIANS SPECIAL? Physicians are trained to remain calm, keep their priorities straight and not get distracted by the surrounding environment. They also develop an inherent ability to learn, understand, integrate a large volume of information and connect facts together to derive logical conclusions. Many of them are mentally and emotionally tough and are capable of enduring prolonged working hours under difficult circumstances, often with no support. They are also team players with a natural compassion and empathy for fellow human beings and they continue to stand by their values even during testing times.3 INTRODUCTION WHAT ARE THE CHANGING PARADIGMS? Major-General Sir Gerald G Giffard, Knight Commander (KCIE) [Indian Medical Service (IMS), retired] read before the East India Association, at Caxton Hall, on November 17th 1924 about the future of medicine in India.1 He informed that the practice of medicine in India is attractive but observed that Indians “…have hardly any aptitude for medical research.” He said that native physicians had spent all their money they could command on their education and therefore could not start independent practice. Therefore, they got stagnated in great towns and became fully dependent on government employment. He along with the Raja of Panagal, the first minister of the Madras government developed several schemes to support physicians with a house for a specified number of years, free medicines and apparatus, and gradually diminish the subsidy over a period of time allowing them to be successful in their practice. Visionaries like them initiated the golden era for the physicians in our country. Today, the practice of clinical medicine is of high Today, we can identify disorders where clinical signs and symptoms are very subtle that they may not be suspected in the first place. Technological advances also help in establishing the etiology of a clinically proven disease objectively at the earliest instant. Timetested conventional management protocols are continuously being tested by the shifting social values, economic situations and political circumstances. The knowledge of physicians is expected to transcend beyond their geopolitical boundaries in the field of medicine and biology. Pharmaceutical industries, diagnostic aids, medical equipment technology and insurance often dose the physicians with strategic snake oils, discredited nostrums and unproven treatment benefits, citing tailored evidence-based medicine. Unlike the previous generations, physicians are often tempted—“why do we not try them?” Therefore, it is often difficult for them to make conscientious decisions considering the cause, consequences and costs in clinical General medicine. The financial experts also make them work on numbers, calculate earnings before the deduction of interest expenses, taxes, depreciation and amortization (EBDITDA), and make them answerable to the creditors in the corporate health care institutions. HOW WAS THE ROAD TRAVERSED? In 1897 the father of Internal medicine, Sir William Osler, spoke of the field of medicine and its uncertainties that, since time memorial, “To have striven, to have made an effort, to have been true to certain ideals - this alone is worth the struggle…. Gentlemen, if you want a profession in which everything is certain you had better give up medicine.” Much earlier our ancient physicians taught that “Dividho jayate vyadih, Sariro manasasthatha, Parasparanz tavorjanma, Nirdvadvam nopalahhyate” (Diseases occur both physically and mentally and even though each part might be dominant, they cannot be compartmentalized). Their understanding in medicine is “Sukarthah sarvabutanam, Matah sarvah pravarthayah, Sukham ca na vina dharmat, thasmad dharmaparo bhavet” (All activities of man are directed to the end of attaining happiness, whereas happiness is never achieved without righteousness. It is the bounden duty of man to be righteous in his action). In Charaka Samhita, it is given that the physician who regards compassion for living beings as the highest religion fulfills his mission (Sidhartah) and obtains the highest happiness. He confers the highest form of religious blessings to the physician who snaps the snares of death for his patients. WHO ARE OUR COLLABORATORS? The Field of Medical Imaging and Technology Conventional medical imaging modalities like X-ray, ultrasound, computed tomography, interventional radiology and magnetic resonance imaging (MRI) always help us to visualize the anatomy of the body precisely. The molecular dynamics, biochemistry and physiology of the body are better explained with singlephoton emission computed tomography (SPECT) and positron emission tomography (PET) studies.4 Fluorescent dyes are being also developed to tag biomolecules and study them without the use of ionizing radiation.5 Therapeutic interventions like selective embolization procedure use of high-energy radiation like beta, alpha, electrons and protons are also available in the armamentarium of the physician.6,7 The Field of Molecular Medicine and Surgery (with DNA Scissors) In molecular medicine, we visualize, characterize, quantitatively measure and modify the biological processes at cellular and molecular levels. We use a piece of DNA encoding reporter protein molecule with a readily measurable phenotype and that can easily be distinguished from background molecules (reporter gene) for this purpose. With this, we can also regulate the transcription, post-transcription regulation of gene expression, protein-protein interactions and the trafficking of molecules within the cells. Treating disorders with alpha-particle emitters like radioactive astatine, which causes minimal collateral damage to the surrounding proteins8 is now possible. Cell biologists have also designed laser scissors and tweezers with which they can operate on the molecules and DNA inside the cells in order to understand and manipulate the cell physiology.9,10 The Field of Artificial Intelligence and Nanomedicine The concept of artificial intelligence came into existence in the mid 1950s, and in this we attempt to emulate intelligence in natural 696 Section 22 and artificial environments alike. This helps us to understand the multitude of complex interactions in biology, especially, the processes involved in synthetic and systemic biology. In synthetic biology, we design and construct new biological components and devices in order to improve upon the existing biological system for the benefit of mankind.11 In nanomedicine, particles measuring from 1 nanometer (nm) to 100 nm in length and 5 nm to 50 nm in width (a white blood cell is more than 10,000 times bigger) that can be produced by self assembly and self-organization processes inside the living system or by chemical method, often coupled with the expertise from artificial intelligence. These are essentially nano-sized machines that can be designed to act as transporters, actuators and motors. Therapeutic agents like drugs, proteins, vaccines, plasmids, etc. can be transported to the specific target cells and delivered with a definite purpose using these nanocarriers. We are working on a model to introduce such nanocarriers into the lymphatic system, maneuver them toward the target organ and optimally time the delivery of drugs. These nanoparticles are highly specific to the target tissue, stealthily evade the immune response, nontoxic, highly stable in the physiological milieu, biodegradable and deliver the consignments across the cell barriers. Apart from drug delivery, they are also capable of recognizing the diseased cell, establishing the diagnosis, site and extent of the disease and monitoring the response to treatment. These are the preliminary steps for the evolution of personalized medicine in the future.12 Nanoscale molecular bearings, molecular gears (Figure 1), neon gas powered molecular motors, tubes and propellers have led to the design of self-assembled monolayered mechanical parts from DNA and protein directed assembly lines. NanoRobotics Laboratory of Ecole Polytechnique in Montreal is using an MRI system as a means of propulsion for a microrobot in the blood vessels. This has led to the designing of the artificial mechanical red blood cells “respirocytes” (Figure 2) capable of delivering 236 times more oxygen to the tissues than the RBCs that can keep the tissues adequately oxygenated for at least 4 hours, even in the absence of respiration due to various clinical conditions. “Microbivores” (Figure 3) are artificial mechanical white blood cells that can digest and destroy the harmful pathogens in bloodstream. Telescoping robotic grapples emerge from silos in the device surface to grab and transport the pathogen in front of the digesting port, where the pathogen undergoes enzymatic breakdown into mono-residue amino acids, mononucleotides, glycerol, free fatty acids and simple sugars.13 Alan M Turing aptly sums up the scope as “We can only see a short distance ahead, but we can see plenty there that needs to be done.” The Field of Tissue Engineering and Aerospace Medicine Engineering the tissues and other biological substrates provide an alternative option to repair the conventional healing processes. Such products have three main components: (1) the isolated cells, (2) the extracellular matrix and (3) the signaling proteins (growth factors). They provide the scaffold materials with cell adhesion and proliferation factors that encourage tissue regeneration. They have extensive applications in orthopedics and cardiovascular system. Implantable devices like stents, retinal implants for restoration of vision and hearing, restore bladder and bowel functions in neuronal injuries and brain computer interfaces for combating mental retardation. There is a renewed interest in the study of telomeres at the chromosomal ends and studies are emerging that the length of telomeres is directly related to the process of aging and longevity.14 Space medicine understands the biophysical and molecular modeling in zero gravity along with prolonged exposure to high- Section 22 Chapter 159 Quo Vadis Medicine... The Road Ahead for Physicians Figure 3: Artificial phagocytes the “microbivores” can fully eliminate infections and repair tissues in the body within few minutes to hours and help physicians to tackle almost entire range of infections Source: Freitas RA. Microbivores: artificial mechanical phagocytes using digest and discharge protocol. Zyvex. 2001;634-45 preprint. http://www. rfreitas.com/Nano/Microbivores.html. Figure 1: A molecular planetary gear is a mechanical component that might be found in the medical nanorobot. The gear converts shaft power from one annular frequency to another. The casing is a strained silicon shell with predominantly sulfur termination, with each of the nine planet gears attached to the planet carrier by a carbon-carbon single bond. The planetary gear shown here has not been built experimentally but has been modeled computationally Source: © 1995, Institute for Molecular Manufacturing (IMM). and vision loss are commonly encountered challenges. As a consequence, we developed newer biomaterials and prosthesis as well as medical devices like the implantable defibrillators, pace makers, light weight wheel chairs, diabetic foot mapping, walkers, radiological imaging devices and telemedicine facilities. We now can also develop smart medical technologies that are compact, light and energy efficient.15 The Field of Health Care Economics and Telecommunication Figure 2: The artificial red cell—the respirocyte that mimics the functioning of the natural red blood cells. About 5 trillion individual respirocytes suspended in 5 ml of 50% saline suspension when injected intravenously can match the gas carrying capacity of the patient’s entire 5.4 liters of blood Source: Freitas RA. Exploratory design in medical nanotechnology: a mechanical artificial red cell. Artif Cells Blood Substit Immobil Biotechnol. 1998;26(4):411-30. http://www.foresight.org/Nanomedicine/Respirocytes. html. energy cosmic radiation particles from the stars to help in survival during prolonged space missions. Loss of bone density and muscle mass, changes in circadian rhythm, proprioceptive problems, sleep disturbances, cardiovascular changes, immune system depression Rapid population growth in our country, increasing life span and age-related disorders, enhanced health awareness promoted by the media, varying degree of disposable income and literacy parameters, heterogeneous distribution of medical institutions, insurance and medical tourism are beginning to have a significant impact on the current practice of medicine. Unlike the west, more than 80% of the health care expenditure is met “out of pocket” by the patient and relatively minimal contribution comes from the government sources. Significant increase in noncommunicable and lifestyle disorders like diabetes, anemia, hypothyroidism, obesity, cardiovascular disorders and cancer are common nowadays.16 There is increasing Foreign Direct Investments in health care institutions, Mergers of stand-alone practices into corporates, high degree of clinical trials and poor effort in basic medical research, migration of large section of population across the country due to occupational necessities like construction and other developmental works also shake the very foundation of ethics in the current practice of medicine.17 Corporatization of the medical institution brings the best of technology within the reach of the common man. Their accreditation to bodies like the International Organization for Standardization (ISO), National Accreditation Board for Hospitals and Health care Providers (NABH), Joint Commission International (JCI), etc. ensures continuity of quality care to patients. However, there is a possibility of decreasing income and increased administrative expenses for the physicians. There may be pressure on physicians to enhance the use of supportive medical services in the name of evidence-based medicine and the importance to clinical acumen could be slighted. Nonphysician managers who were trained by business gurus, who have no idea of compassion, empathy and human values, are also 697 General REFERENCES likely to deviate health care administration from patient-centric physician driven model to a profit-oriented revenue generating business model. WHY PERSONALIZED MEDICINE? Personalized medicine involves administration of a drug exclusively tailored to the genetic makeup of an individual, so that the drug is delivered with maximum safety and effectiveness to get the best possible clinical outcome. In India, there is a vast population of diverse genomic makeup and it requires extraordinary energy and resources from the government and the industry to deliver personalized medicine. It practically involves diverse scientific fields to work together toward a common goal—integrating the progress in the field of information technology, clinical information from individuals, physicians, hospitals, diagnostic centers, pharmacies, research laboratories, insurers and the government. Since it has tremendous industry potential, very soon every institution is going to talk involved in personalized medicine.18 WHERE ARE WE HEADED? We have seen that the road ahead for the physicians is smooth and yet challenging, with the best of technology and talents at our disposal. The Indian government has declared a perennial requirement of physicians for optimum health care delivery, both in urban and rural areas—more in rural areas, despite the mushrooming of medical colleges in recent times.19 Gone will be the days of organ transplantation and infusion of the body with loads of toxic drugs. The medical field will now be focused on prevention of organ failure, organ preservation and regeneration of failed components, with the help of molecular and personalized medicine. More and more basic medical scientists and engineers will get actively involved in the field of medicine. In the pursuit of excellence in medicine, physicians must have rigor and commitment to evidence-based medicine, up-to-date information-management skills, a commitment to lifelong education for themselves, their patients, and their colleagues and trainees and have complete command over the technology. The society sees them as an embodiment of the knowledge and professionalism. The physician’s evolution is built on a very stable platform with a deeprooted foundation of ethics.20 Commercialization of health care and market driven economy is likely to divert our vision and create an illusion of prosperity. Due diligence has to be exercised while balancing the art of clinical medicine and the science of modern technology. “Water flows in the river, but the river cannot drink it. It is for the humanity. Cow yields milk, but it cannot drink it. It is for the humanity. Tree yields fruits, but it cannot eat it. It is for the humanity.” ~ Bhagwan Sri Sathya Sai Baba’s comments on Medicine to Physicians 698 Section 22 1. The future of medicine in India. Br Med J. 1924;2(3334):966-77. 2. Fletcher RH, Fletcher SW. What is the future of internal medicine? Ann Intern Med. 1993;119(11):1144-5. 3. Pfeffer J, Sutton RI. Evidence-based management. Harv Bus Rev. 2006;84:62-74. 4. Rahmim A, Ziadi H. PET versus SPECT: strengths, limitations and challenges. Nucl Med Commun. 2008;29:193-207. 5. Vasquez KO, Casavant C, Peterson JD. Quantitative whole body biodistribution of fluorescent-labeled agents by non-invasive tomographic imaging. PLoS One. 2011;6(6):e20594. 6. Pozzi OR, Zalutsky MR. Radiopharmaceutical chemistry of targeted radiotherapeutics, Part 3: alpha-particle-induced radiolytic effects on the chemical behavior of (211)At. J Nucl Med. 2007;48:1190-6. 7. Fukumitsu N. Particle beam therapy for cancer of the skull base, nasal cavity, and paranasal sinus. ISRN Otolaryngology. 2012;ID 965204:1-6. 8. Mahdi E, Fariba K. Molecular scissors: new tools in biotechnology and genome surgery. Ann Biol Res. 2012;3(1):638-44. 9. Berns MW. Laser scissors and tweezers. Sci Am. 1998;278:62-7. 10. Zaremba M, Siksnys V. Molecular scissors under light control. Proc Natl Acad Sci U S A. 2010;107(4):1259-60. 11. Berrar D, Sato N, Schuster A. Artificial intelligence in neuro­science and systems biology: lessons learnt, open problems, and the road ahead. Advances in Artificial Intelligence. 2010;578309:1-12. 12. Roszek B, de Jong WH, Geertsma RE. Nanotechnology in medical applications: state-of-the-art in materials and devices. RIVM report 265001001, 2005. 13. Freitas RA. Current status of nanomedicine and medical nanorobotics. J Comput Theor Nanosci. 2005;2(1):1-25. 14. Aubert G, Lansdrop PM. Telomeres and aging. Physiol Rev. 2008;88:55779. 15. Losch A. Nanomedicine and space: discursive orders of mediating innovations. In: Baird D, Nordmann A, Schummer J (Eds). Discovering the Nanoscale. Amsterdam: IOS Press; 2004.pp.193-202. 16. Annual Report to the People on Health, 2010, Department of Health and Family Welfare, Government of India. 17. Healthcare Special, India Business Equity Foundation Brochure, 2010, Confederation of Indian Industries, New Delhi. 18. Gupta R, Kim JP, Spiegel J, et al. Developing products for personalized medicine: NIH Research Tools Policy applications, Personalized Med. 2004;1(1):115-24. 19. Report of the National Commission on Macroeconomics and Health, Ministry of Health and Family Welfare, Govern-ment of India. 2005. 20. Souba WW. The being of leadership. Philosophy, Ethics, and Humanities in Medicine. 2011;6:1-11.