Health Education &
Behavior
http://heb.sagepub.com
Mass Media in Health Promotion: An Analysis Using an Extended
Information-Processing Model
Brian R. Flay, Don DiTecco and Ronald P. Schlegel
Health Educ Behav 1980; 7; 127
DOI: 10.1177/109019818000700203
The online version of this article can be found at:
http://heb.sagepub.com/cgi/content/abstract/7/2/127
Published by:
http://www.sagepublications.com
On behalf of:
Society for Public Health Education
Additional services and information for Health Education & Behavior can be found at:
Email Alerts: http://heb.sagepub.com/cgi/alerts
Subscriptions: http://heb.sagepub.com/subscriptions
Reprints: http://www.sagepub.com/journalsReprints.nav
Permissions: http://www.sagepub.com/journalsPermissions.nav
Citations (this article cites 31 articles hosted on the
SAGE Journals Online and HighWire Press platforms):
http://heb.sagepub.com/cgi/content/refs/7/2/127
Downloaded from http://heb.sagepub.com at UNIV OF ILLINOIS AT CHICAGO on August 25, 2007
© 1980 Society for Public Health Education. All rights reserved. Not for commercial use or
unauthorized distribution.
Mass Media in Health Promotion:
An Analysis Using an Extended
Information-Processing Model
Brian R. Flay, D. Phil.
Don DiTecco, M.A.
Ronald P. Schlegel, Ph.D
University of Waterloo
ABSTRACT: The information-processing model of the attitude and
behavior change process was critically examined and extended from six to
12 levels for a better analysis of change due to mass media campaigns.
Findings from social psychology and communications research, and from
evaluations of mass media health promotion programs, were reviewed to
determine how source, message, channel, receiver, and destination
variables affect each of the levels of change of major interest (knowledge,
beliefs, attitudes, intentions and behavior). Factors found to most likely
induce permanent attitude and behavior change (most important in health
promotion) were: presentation and repetition over long time periods, via
multiple sources, at different times (including "prime" or high-exposure
times), by multiple sources, in novel and involving ways, with appeals to
multiple motives, development of social support, and provisions of
appropriate behavioral skills, alternatives, and reinforcement (preferably
in ways that get the active participation of the audience). Suggestions for
evaluation of mass media programs that take account of this complexity
were advanced.
We are increasingly learning about how lifestyles affect
health.’-3 Accordingly, there is a growing consensus regarding the
need to promote positive health behaviors on a large scale basis.
The rising costs of traditional health care increases the need to find
the most effective method of modifying health behaviors. One
approach which has generated much enthusiasm is the use of mass
media campaigns. The last decade has seen an increasing number
of attempts to use mass media campaigns to influence the public
paper was partially supported by a University of Waterloo Research Grant
the first author. We would like to thank Thomas D. Cook for helpful comments on an
earlier version, and Carolyn Edison and Janice Dick for their extensive assistance in library
research.
Address reprint requests to the first author, Health Studies Department, University of
Waterloo, Waterloo, Ontario, Canada, N2L 3G1.
Preparation of this
to
127
Downloaded from http://heb.sagepub.com at UNIV OF ILLINOIS AT CHICAGO on August 25, 2007
© 1980 Society for Public Health Education. All rights reserved. Not for commercial use or
unauthorized distribution.
good in the areas of disease prevention, health
promotion, and public safety. Some of the substantive areas
addressed, together with selected illustrative references and
for their
own
reviews of them
are as
follows.
1. General Health, of which the Stanford Three Community
Heart Disease Prevention Project,4-6 the North Karelia Project/-9 and the &dquo;Feeling Good&dquo; television series produced by
the producers of &dquo;Sesame Street,&dquo; but with a health
2.
3.
4.
5.
6.
7.
promotion focus and targeted to adu Its, 10 are probably the
most well known;
Safety, especially driving,11-14 seat belt use,’ 1.16 and lawnmower safety;&dquo;
Smoking;,&2Z
Alcohol and Drug Abuse;23.25
Family Planning,21-28
Programs in Third World countries;29-33
Miscellaneous areas such as cancer control,34 immunization,35 screening,36 compliance,37 mental health,38 and lung
disease.39
many of these
the
numerous
mass
media health
Of
programs
that
have
been
mounted, only some have
promotion campaigns
been reported in public outlets. Most have been described only in
internal reports not generally available to the public and some
have not been documented at all. Few media campaigns have been
formally evaluated and, of those evaluations undertaken, many
have turned out to be uninterpretable or invalid because of
unresolved methodological, technical, administrative, and/or
political issues .11.40.41 This happens not for want of adequate
methodology. The tools of evaluation research in general are well
established.42-59 The problem seems to be lack of an adequate
appreciation of either a) these tools and methodologies, or b) the
complexity of the attitude/behavior change process. As a result,
the interpretation of most of those evaluations of mass media
programs which have been carried out has been ambiguous or
Unfortunately, assessing the effectiveness of
is difficult.
impossible.
It has proven unusually difficult to develop methods of
influencing the public to change their attitudes, and especially
their behaviors, to improve their health status. Of those media
campaigns successfully evaluated, only a few demonstrated
successful behavior change.4-6.13,18.22 Most have been found to be
unsuccessful in influencing attitudes and behavior for any length
128
Downloaded from http://heb.sagepub.com at UNIV OF ILLINOIS AT CHICAGO on August 25, 2007
© 1980 Society for Public Health Education. All rights reserved. Not for commercial use or
unauthorized distribution.
of time. cf. review i5.2i.27.6M5 Bvp suggest that part of the reason for this
lack of success is the absence of systematic application of known
communication principles in the design and evaluation of mass
media programs.
This paper presents a model of the attitude/behavior change
process which can serve as a guide for assessing the substantive
adequacy of mass media programs as well as having relevance to
evaluation strategies. Initially McGuire’s information processing
model of attitude change is described and then examined in terms
of knowledge from social psychology and communication
research and its potential relevance to health promotion. Finally a
more detailed, extended model of the communication/change
process is suggested.
THE INFORMATION PROCESSING MODEL
The most well developed and researched model of the
is the classic information-processing
model of general attitude and behavior change first developed at
Yale by Hovland66.67 and hence often known as the Yale or Hovland
model. It has been elaborated upon and extensively advocated by
McGuire ’68-71 who has suggested a &dquo;persuasion matrix&dquo; as a way of
conceptualizing the change process and understanding the
complexities of the relationships between outcomes (changes in
knowledge, attitudes, and behavior), and inputs (the persuasive
communication and its properties).
communication process
Communication Factors
The columns of McGuire’s persuasion matrix are factors which
locate, alone or in combination, the independent variables (or
inputs) of most general attitude change studies. These include:
1. Source factors-the attributes of the perceived source of the
message;
2. Message factors-the content, structure and style of the
message;
3. Channel factors-the medium used, and how it is used;
4. Receiver factors-the characteristics of the audience receiv-
ing the
message;
5. Destination factors-the target issue, the target component
of general attitude, and whether the change is long-term or
short-term,
etc.
129
Downloaded from http://heb.sagepub.com at UNIV OF ILLINOIS AT CHICAGO on August 25, 2007
© 1980 Society for Public Health Education. All rights reserved. Not for commercial use or
unauthorized distribution.
It is suggested here that any review or evaluation of the
potential effectiveness of mass media programs needs to consider
each of the above elements of the communication process. A
comprehensive review of how source, message, channel, receiver
and destination variables affect general attitude change in
laboratory studies has been provided by McGuire,69 and
summarized by Roberts’4 and Zimbardo, Ebbesen, and Maslach. 7S
The Stochastic Change Process
The
rows
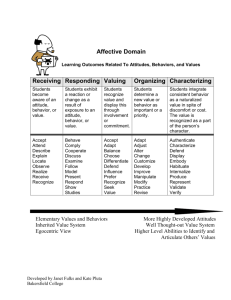
of McGuire’s persuasion matrix represent
common
dependent variables (outcomes) in general attitude change studies
and, according to McGuire,69.71 also constitute six steps in the
stochastic process of general attitude change. The six steps
suggested by McGuire are:
1.
2.
3.
4.
5.
Being presented with the persuasive message (exposure);
Attending to the message (awareness);
Comprehending its content (knowledge);
Yielding to its appeal (beliefs/attitudes);
Retaining this new position (persistence of attitude change;
and
6.
Acting
on
the basis of it (behavior).
The complete
represented
as
information-processing
in
Figure
model may,
therefore, be
1.
FIGURE 1. McGuire’s persuasion matrix.
130
Downloaded from http://heb.sagepub.com at UNIV OF ILLINOIS AT CHICAGO on August 25, 2007
© 1980 Society for Public Health Education. All rights reserved. Not for commercial use or
unauthorized distribution.
generally assumed that belief (cognitive) changes will automatically lead to attitude (affective) and behavior (conative)
changes,&dquo; apparently because of a need for psychological
consistency. This is not the only possible order of change however.
Ray’6 has provided a systematic analysis of the different orders
of change and suggests three basic &dquo;hierarchy of effects&dquo; models
It is
of communication response in terms of cognitive, affective and
conative elements. The appropriateness of each model for a
particular situation is most dependent upon the factors of
involvement, differentiation of alternatives, and communication
source. The three hierarchies are:
The low-involvement hierarchy in which learning new information
leads directly to behavior change which subsequently produces
attitude change (i.e., cognitive-conative-affective). The low
involvement hierarchy would be likely to occur when, as its name
implies, there is a low involvement on the part of the target audience and minimal differences between alternative behaviors. This
would be a typical situation for many consumer choices. For example, an individual is not tremendously concerned about what
brand of soap he buys and if costs are close he should choose that
brand with which he is most familiar (has been exposed to or has
had favourable experiences with). This behavior will then be
followed by positive attitudes if the soap is found satisfactory.
The dissonance-attribution hierarchy in which behavior occurs first
(the consumer is forced to make a choice on the basis of some nonmedia source) leading to attitude change as a function of
dissonance or self-attribution, and then selective learning
consistent with the original behavior (i.e., conative-affectivecognitive). This situation should most likely occur when the target
audience is involved but there is little difference among
alternatives.
The learning hierarchy in which cognitions are altered which leads
change of attitude which then determines the appropriate
behavior (i.e., cognitive-affective-conative). According to Ray,
this hierarchical ordering should most likely occur when the target
audience is involved and there are clear differences between
alternatives.
to a
there
no
doubt exceptions, and the
be structured to affect involvement and
differentiation of alternatives, the learning model (i.e.,
cognitive-affective-conative hierarchy) would seem most
Although
communication itself
are
can
131
Downloaded from http://heb.sagepub.com at UNIV OF ILLINOIS AT CHICAGO on August 25, 2007
© 1980 Society for Public Health Education. All rights reserved. Not for commercial use or
unauthorized distribution.
health promotion campaigns. Changing health
typically involves important adjustments by
individuals and so the alternatives (e.g., quitting vs. continuing
smoking) are highly differentiable. Further, involvement should be
high where the potential importance of the behavior for personal
welfare is known. For these reasons it is suggested that typically
the information-processing model is appropriate for mass media
health promotion programs.
The following briefly presents findings from social psychology
and communications research as they relate to each stage of the
stochastic change process and compares these with findings from
health promotion campaigns. In view of these considerations the
adequacy of McGuire’s model is assessed and an extended version
of the information-processing model is proposed.
appropriate
to
relevant behaviors
KNOWLEDGE FROM SOCIAL PSYCHOLOGY
AND COMMUNICATION RESEARCH
Presentation of the Message
It should be relatively easy to change people’s awareness of
certain issues as long as they can be exposed to information.
Although few evaluations have bothered to measure exposure or
awareness, many health promotion programs have probably failed
because they did not reach their target audience.&dquo; A major
problem here is the potential for selective exposure, that is the
tendency for persuasive appeals not to reach those to whom they
are directed.
For example, a program aimed at increasing
awareness of nutritional requirements may only be watched by
those already interested in nutrition who probably have a
reasonable knowledge of the subject, while those who are
relatively uninformed, and thus uninterested, watch something
else. In the presentation of the message then, although a popular
media (channel) is selected, pre-existing audience (receiver)
factors may preclude exposure. For this reason, one of the basic
techniques of advertising is to insert a message which is novel,
shocking, and/or entertaining (to ensure attention) into a specific
program which is already determined to have a large audience (to
ensure
exposure).
Attention and
Comprehension
In order to change people’s knowledge they have to be
motivated to attend to and to comprehend the information being
132
Downloaded from http://heb.sagepub.com at UNIV OF ILLINOIS AT CHICAGO on August 25, 2007
© 1980 Society for Public Health Education. All rights reserved. Not for commercial use or
unauthorized distribution.
presented
or
else the information has to be repeated
so
many times
that it becomes &dquo;lore.&dquo;
Theories of learning (attention and comprehension in the
present context) and research on instructional media are well
established and have already been thoroughly reviewed
elsewhere.78-86 Although many of the hundreds of studies done with
instructional media are methodologically so poor as to be
uninterpretable,4~ it appears that any media can lead to
improvements in knowledge just as well as face-to-face
instruction, but not necessarily any better, and that no one form of
media is consistently better than another. An important
implication, however, is that media, especially radio, are much
cheaper, and therefore more cost-effective than face-to-face
instruction.86-8’
The above findings are macro-level ones. Micro-level findings
few: a) programs must be directed at a felt need (to ensure
attention); and b) hearing a program in groups and discussing it
afterwards leads to better understanding.
are
Yielding and
Retention
There
both the
vast
literatures on belief and attitude change within
of social psychology and communications research.
A confusing, and sometimes contradictory, array of findings and
theories has been generated.88-95 This confusion was somewhat
reduced when McGuire69 provided a thorough conceptual review
of the area.
For changes due to a health promotion campaign to be
meaningful, they must persist over long periods of time. It has
been suggested that many of the changes in belief and attitude
reported in the literature might have been no more than responses
to immediate situational demands and did not represent
meaningful change at a11.9~98This fundamental issue was addressed
recently when Cook and Flay96 provided a review of the conditions
under which attitude change persisted over time.
The findings from the Cook and Flay96 and McGuire69 reviews,
together with summaries by Roberts’4 and Zimbardo et al. 75 provide the clearest picture of the conditions most conducive to
meaningful and persistent changes in attitude that can be derived
from the social psychological and communications research
literatures. These conditions may be summarized as follows.
A persuasive message has most impact if it:
1.
are
areas
comes from multiple sources of high credibility (i.e., trustworthiness and expertise) and similarity (a property of the
source);
Downloaded from http://heb.sagepub.com at UNIV OF ILLINOIS AT CHICAGO on August 25, 2007
© 1980 Society for Public Health Education. All rights reserved. Not for commercial use or
unauthorized distribution.
133
2. is repeated often and consistently (message);
3. is sent via multiple media at accessible times and locations
(channel);
4.
is accompanied by a high level of a) personal involvement in the issue and b) consistency with related attitude and value structures (receiver);
arouses or
Finally, two other factors which appear to fall outside of
McGuire’s communication variables but which have been found to
be important are:
5. a high level of social support
environment; and
6.
or
acceptance in the receiver’s
opportunities to give expression to the newly formed
titudes, and ongoing reinforcement for doing so.
at-
There are other conditions that appear to be conducive to meaningful and persistent attitude change. Many of these involve interactions between the components of the communication process
(e.g., between message and receiver factors, such as higher fear
arousal being more effective for less anxious receivers, or an explicit conclusion being more effective with a less intelligent, uninformed audience). They are reviewed best by McGuire.69
A cting
Some researchers have relied on expressions of intention as indicators of behavior, while others have assessed only behavior. For
this reason both concepts are treated together here.
The available information on meaningful and long-term
behavior change is much more sparse and scattered than that on
knowledge, belief, and attitude change. Within psychology, researchers have only recently begun to investigate the conditions
necessary for the long-term maintenance of changed behaviors.96
Examples of recent statements regarding health-related behaviors
are Wilson99 for the treatment of obesity, Best18.100 for smoking
cessation, and Marlatt & Gordon101 for various addictive behaviors,
including alcoholism and smoking.
The consensus about the factors that contribute to long-term
change may be summarized as:
1.
2.
specific target behaviors to be changed - a non-specific program cannot effect specific changes;
a desire to change, which most clients in behavior change
programs already have96-for mass media programs to be
successful they must be either targeted at people who
already have this desire or else they must motivate the desire;
134
Downloaded from http://heb.sagepub.com at UNIV OF ILLINOIS AT CHICAGO on August 25, 2007
© 1980 Society for Public Health Education. All rights reserved. Not for commercial use or
unauthorized distribution.
3. the
provision of multiple alternative behaviors
as
coping
re-
sponses in those situations where the undesired behavior
would
be practiced;18.102
with making the social environment supportive;18.103.1o4 and possibly
5. an emphasis on self-management of the behavior change.
4.
a
normally
concern
It is apparent that the above factors do not readily fall into
McGuire’s communication categories. Recall that the assumption
underlying the model was that changing attitude automatically
should produce behavior change. This point shall be considered
further when an extension of the information-processing model is
proposed.
FINDINGS FROM EVALUATED MASS MEDIA PROGRAMS
Despite the limitations of past evaluations, preliminary reviews
of those mass media programs that have been evaluated suggest
some conditions that seem to affect the likelihood of media
campaigns being effective .11.13.1 <;.20-23.60-63.65
Conditions conducive to effective belief or attitude change
appear to be:
1.
2.
3.
arousing involvement
in the issue
and/or
motivation to
change;
much repetition by several sources, via multi-media, over
long periods of time (i.e., years, not weeks or months);
novelty in the way the message is presented (in order to maintain
attention
and
increase
the
chance
of
arousing
involvement);
targeting very specific
issues and providing consistent alternative attitudinal structures; and
5. high quality production of materials (equal to that of commercial mass media production) to ensure attention.
4.
It is encouraging to note that the above factors are very similar to
those derived from the social-psychological and communications
research theories and findings.
Mass media campaigns have been even less successful at
changing behaviors than at changing beliefs or attitudes. At least
this is so for specific target behaviors-there is some question
about the influence of the media on behavior in a more general
way.86 Few of the mass media health promotion campaigns listed
135
Downloaded from http://heb.sagepub.com at UNIV OF ILLINOIS AT CHICAGO on August 25, 2007
© 1980 Society for Public Health Education. All rights reserved. Not for commercial use or
unauthorized distribution.
earlier that have been evaluated have demonstrated 5’successful
behavior change, especially over the long term. Those which have
had success however,4-7.18.101 usually included additional elements in
their overall program which involved identifying alternative
(healthy) behaviors and/or specifying the development of personal
skills necessary to performing these behaviors. These objectives
were pursued in various ways including combinations of the
following:
1.
incorporation of information pertaining to behavioral alterdevelopment within the communication
message itself;
promotion of interaction with the audience (e.g., via
telephone or written materials);
supplementation with face-to-face clinics; and
mobilization or restructuring of community resources (e.g.,
cooperation with the dairy industry to develop low-fat dairy
products in the North Karelia project).
natives and skills
2.
3.
4.
IMPLICATIONS: EXTENSION OF THE
INFORMATION PROCESSING MODEL
Generally McGuire’s model offers a good paradigm for the planning and assessment of mass-communication/health-promotion
campaigns. However, certain deficiencies can be demonstrated
concerning the validity of the assumption that changes in knowledge and beliefs will automatically lead to changes in attitude
and ultimately behavior. This is directly relevant to the appropriateness and comprehensiveness of the model for assessing and
planning health promotion strategies based on mass communication approaches.
Differentiating Concepts
z
We agree with McGuire that the
general attitude change process
several
involving
steps. However, work in social
on
the
attitude-behavior
psychology
consistency problem89would
suggest that the steps involved in changing knowledge and/or
beliefs ought to be differentiated from those involving attitudes,
intentions, and behaviors.
Although the distinction between knowledge and belief is not
definitive we may generally discriminate these concepts in the
following way. Knowledge can be defined as factual information,
whereas belief pertains to the degree to which one subjectively
is
a
stochastic
one
136
Downloaded from http://heb.sagepub.com at UNIV OF ILLINOIS AT CHICAGO on August 25, 2007
© 1980 Society for Public Health Education. All rights reserved. Not for commercial use or
unauthorized distribution.
association between some object or behavior (e.g.,
an attribute or consequence (e.g., lung cancer).
smoking)
as a given or universal truism; belief is a
is
taken
Knowledge
of
estimate
subjective probability that reflects varying
personal
of
This
is not to say that a change in knowledge
degrees certainty.
will not lead to a change in beliefs. It clearly sometimes will,89 and
this is what McGuire69 calls acceptance or yielding (changing ones
accepts
an
and
the basis of new knowledge).
According to Fishbein’s89formulation an attitude is conceived of
as an evaluative (affective) response toward some object or act,
and this response is based upon an underlying set of beliefs where
each is weighted by the value placed upon the associated attribute
(viz. an object) or expected outcome (viz. an action). Thus an
attitude reflects the net value (or affect) that is associated with this
underlying set of beliefs. This value-expectancy formulation
underscores the potential complexity of the belief-attitude
connection. For example, an apparently highly relevant belief
change (smoking is carcinogenic) may not lead to the expected
attitude change (smoking is bad for me) if an individual’s personal
expectation for the negative outcome (cancer) is low, of if
expected positive outcomes (smoking relaxes me) are numerous.
Behavioral intentions may be defined as one’s personal estimate
of the subjective probability of performing a certain behavior (or
class of behaviors). According to Fishbein, attitude is only one of
two major factors which will affect an individual’s intention to
engage in a behavior. Beliefs concerning what important others
(e.g., peers, relatives) want us to do will also determine our intenbeliefs
on
tions.
Finally,
acts
it is
which
are
recognized that behavior, the specific act or set of
the focus of concern, will be directly related to in-
tention only in so far as extraneous factors which may interfere
with the behavior are not present.101 Thus, other considerations
such as situational constraints, social support systems, skills, alternative behaviors, etc. may affect the intention-behavior connection.
How does McGuire’s model (Figure 1) match up with the concepts of knowledge, beliefs, attitudes, intentions, and behavior
(KBAIB) identified above? Clearly, attention and comprehension
have to do with knowledge, and action has to do with behavior.
But are yielding and retention concerned with beliefs or attitudes
(affective) or both? From McGuire’s writings it is not altogether
clear. In places it seems as if he would agree with Cartwright77 who
classified beliefs together with knowledge as part of the cognitive
structure, attitudes and values under a motivational structure, and
137
Downloaded from http://heb.sagepub.com at UNIV OF ILLINOIS AT CHICAGO on August 25, 2007
© 1980 Society for Public Health Education. All rights reserved. Not for commercial use or
unauthorized distribution.
intentions, behaviors, and supportive environments as part of the
behavioral structure. In other places, however, he suggests that
yielding leads to attitude change. However, when it comes to
operationalizing measurement of each step, McGuire seems to
think of attitude change as being cognitive as measured by an
&dquo;opinionnaire.&dquo;70,72 What is clear, is that the information-processing model is most appropriately concerned with changes in Cartwright’s&dquo; cognitive structure, especially beliefs. Once changes in
knowledge and beliefs have been brought about, it is assumed that
changes in attitudes, intentions, and behavior will automatically
follow,75 apparently because of a need for consistency. Thus
McGuire’s model does not directly address issues of attitude and
behavior change.
Similarly, although McGuire considers as important the retention of memory of message content or (depending on which source
you read) the new belief, he does not consider the maintenance of
new behavior. 11,96,99.100.102,101, Since maintaining a certain behavior is
often the basic goal of health promotion attempts, it must be an integral aspect of any model in this area.
The above differentiation reveals a hierarchy of potential
change areas. It is generally assumed that changes in beliefs are
usually more difficult to obtain than changes in knowledge,
changes in attitude are probably more difficult to obtain than
changes in belief, and long-term behavior change is usually more
difficult to obtain than attitude and intention change. For example, practically all smokers now know of the association between
smoking and certain diseases (knowledge); most of them, but not
all, accept that smoking causes cancer (belief); fewer, though still a
large proportion, agree that smoking is bad for them personally (attitude) and desire (have intentions) to stop; but a large proportion
of these people still do not stop smoking (behavior).
Extending the Model
Considering the above points we suggest the adaptation of the
information-processing model as shown in Figure 2.
The arrows from one dependent variable to another in Figure 2
suggest
a
casual chain where:
exposure will lead to awareness, but only when the message is
attended to;
awareness will lead to changes in knowledge, but only when the
message is
changes in
comprehended;
knowledge will lead
arguments
and
or
to changes in beliefs, but only if the
conclusions of the message are accepted or yielded to;
138
Downloaded from http://heb.sagepub.com at UNIV OF ILLINOIS AT CHICAGO on August 25, 2007
© 1980 Society for Public Health Education. All rights reserved. Not for commercial use or
unauthorized distribution.
might (hence the dashed arrows) lead to changes
attitude, intentions, and ultimately behavior.
This makes it clear that other factors play a major role in
determining the particular behavior engaged in.
As we have seen from the above reviews, factors relating to the
receiver’s environment, such as social support, opportunity to
express attitudes, and reinforcement for behavior, are important in
translating attitudes or intentions into action. Until now these
changes
in beliefs
in
factors have been given little attention in mass communications,
although it is feasible that they could be addressed. For example, a
persuasive message regarding &dquo;quitting smoking&dquo; could be
targeted towards families or other relevant social groups rather
than individuals; or messages could be aimed at convincing people
to support those who are trying to quit. Furthermore, it is necessary
for the target individual to be given the skills necessary to change a
particular health behavior if his or her intention is to be translated
successfully into action. Although these skills can be thought of as
receiver characteristics, they are typically absent in those to whom
the communication is addressed. However the inclusion of skill
training within the context of a persuasive message has been
attempted infrequently at the mass communication level. Thus
other approaches, such as value-expectancy formulations,107.108the
FIGURE 2. A reconceptualization of the information processing model of
the general attitude change process.
139
Downloaded from http://heb.sagepub.com at UNIV OF ILLINOIS AT CHICAGO on August 25, 2007
© 1980 Society for Public Health Education. All rights reserved. Not for commercial use or
unauthorized distribution.
health belief model9 value self-confrontation procedures,11o.111
Fishbein’s behavior prediction model,89 Cartwright’s motivational
and behavioral structures,&dquo; and social learning theories112.113 that
take into account other factors affecting change (e.g., values,
social support structures, and behavioral skills and alternatives)
appear to be necessary for a comprehensive model of the attitude
and behavior chance process. 114
In considering his model for attitude change, and the empirical
evidence relevant to it, McGuire69 was not certain whether all
levels of change had to occur for meaningful and persistent
attitude change to occur. Consideration of the model in respect of
the five KBAIB concepts, suggests that change is not necessary at
all levels in order for meaningful change to occur in any one of
KBAIB. For example, changes in beliefs or attitudes can occur
without changes in knowledge or behavior. Sometimes changes in
behavior can even occur without accompanying changes in beliefs
or attitude. However, in real-life situations (as opposed to the
laboratory) it seems clear that meaningful and long-term change in
any one element of KBAIB is more likely if there is also
corresponding change in the other four elements. For example, as
would be predicted from the many consistency theories in social
psychology,&dquo;5 changes in beliefs or attitude are more likely to
persist if they are accompanied by corresponding changes in
knowledge and behavior.96 Changes in behavior are more likely to
be maintained if the underlying cognitive and motivational
structures are consistent with the new behavior. Even changes in
knowledge are probably more likely to be retained if other
experiences, as represented by the corresponding beliefs,
attitudes, and behavior, are consistent with it.
Implications for Evaluation
The complexity of the extended information-processing model
implies that a comprehensive mass media program should meet all
the conditions suggested above to maximize effectiveness.
Similarly, a comprehensive evaluation of a mass media program
should measure outcomes, and their antecedent variables, at all
levels of the 12 stage change process. In past evaluations,
interpretation has been especially difficult in those cases when the
program apparently failed. If the major outcome measured was
health status or behavior, then failure could be located at any one
of the other steps in the change process. Did it fail because people
were not exposed to it, did not attend to it, did not understand it,
did not accept or yield to it, etc.? Assessments of behavior and
health status may answer questions of impact, but without answers
140
Downloaded from http://heb.sagepub.com at UNIV OF ILLINOIS AT CHICAGO on August 25, 2007
© 1980 Society for Public Health Education. All rights reserved. Not for commercial use or
unauthorized distribution.
process, questions about why
cannot be answered.48 In
effective
program
addition to the types of questions above, questions of treatment
(the source, the message, and the channel), the receiver (audience),
and the context should also be asked in a comprehensive
evaluation. Finally, it should be emphasized that there needs to be
a correspondence between the mass media content and the
particular outcome measures assessed. In some programs, very
general interventions have been planned and then were evaluated
by very specific outcome criteria. General interventions (e.g., good
nutrition) should be assessed by multiple-act criteria since people
may respond in any number of &dquo;correct&dquo; ways. On the other hand,
if very specific outcomes are desired (e.g., checkups for high blood
pressure), then the intervention content must be appropriately
specific and the corresponding single-act criterion assessed.&dquo;6 As
we have seen, the failure to do methodologically adequate
evaluations means that the findings from mass media campaigns
to date, as opposed to the &dquo;field-wisdom&dquo;, are scarce.
to
a
questions of implementation and
was
or was
not
SUMMARY: A PROFILE FOR SUCCESSFUL
MASS MEDIA PROGRAMS
The ultimate, long-term objective of any health promotion mass
media program must be to change people’s lifestyles (behavior), or
to prevent negative lifestyles, and consequently improve their
long-term health status. Although there is still some question
about whether or not all 12 steps of the persuasion process are
necessary to lead to behavior changes we suspect that they are
necessary if permanent behavior change, and therefore changes in
health status, are to be effected. Thus, any change attempt, mass
mediated or not, should aim to end up with consistency both
within and between cognitive, motivational and behavioral
structures. That is, consistency across knowledge, beliefs,
attitudes, intentions, and behavior must be sought. In addition,
more general values and social norms may also need to be
considered.
For some issues, some of the steps in the persuasion process may
already be consistent with the behavior desired by the health
promoter. In such cases, the consistent knowledge and/or beliefs,
for instance, need only be reinforced and the message can
concentrate on attitudes and behavior. A good example is that
most smokers already know of the association between smoking
and lung cancer, accept (believe) that it is probably a casual link,
141
Downloaded from http://heb.sagepub.com at UNIV OF ILLINOIS AT CHICAGO on August 25, 2007
© 1980 Society for Public Health Education. All rights reserved. Not for commercial use or
unauthorized distribution.
and feel that smoking is bad for their own health and desire to
stop. In that case any (health promotion) change strategy need
only reinforce the consistent knowledge, opinions, attitudes, and
behavioral intentions, and concentrate on changing behavior.
However, in all cases the first requirement is to reach the target
audience. Many programs have probably proved ineffective
because not enough people were exposed to it. Airing spots on
public television or at non-peak hours on commercial television
does not ensure good exposure.&dquo;’ Presentations via multi-media,
at different times, over long periods are necessary simply to get
exposure.
Once exposure is
achieved,
it is
no use
reaching people’s living
if they do not attend to the message. Appeals to multiple
motives (e.g., to improve health, to improve social and/or self
esteem, to decrease cost of living, to improve quality of life); in
novel ways; with repetition across sources, channels, and times;
will help get attention. An expert (who is perceived as credible and
trustworthy), yet similar, source who presents a clearly targeted,
concise, easily understood message will also increase attention, as
well as ensure comprehension.
Acceptance of, or yielding to, the message is also more likely if
the source is credible and similar and presents the message in an
arousing and involving (i.e., motivating) way. Changes in attitudes
and intentions are more likely if that source also offers social
support, and asks for (and gets) active participation (answer a
rooms
questionnaire, keep a diary, etc.). Repetition in many ways,
involvement, active participation, and social support, all together,
also increase the likelihood of persistent changes in attitudes and
intentions. This has been found to be true for the
well
as
in the real world with the
laboratory,96 as
long-term effects of smoking
campaigns.22
Many of the factors mentioned above will
increase the chance
of behavior change consistent with all the other changes. However,
the chances of behavior change are maximized only when explicit
ways to change are provided. This means providing the
appropriate behavioral control and behavioral skills, as well as
appropriate alternative behaviors for those situations where the
old behavior took place. New behaviors will only be maintained
over time if an appropriate social support structure (e.g., spousal
support for persons losing weight) is available and the new
behaviors are positively reinforced at least on a decreasing
random interval basis.
In conclusion, this review has demonstrated that the earlier
pessimism about the effectiveness of mass media in health
142
Downloaded from http://heb.sagepub.com at UNIV OF ILLINOIS AT CHICAGO on August 25, 2007
© 1980 Society for Public Health Education. All rights reserved. Not for commercial use or
unauthorized distribution.
promotion’ 1,11,61-61should now give way to a cautious optimism and
more sophisticated development. Our analysis suggests that the
use
of mass media may sometimes be as successful as
face-to-face interventions if the appropriate components (e.g.,
skill training) are included in the communication. However, an
optimally effective campaign may need to incorporate yet other
approaches to behavior change.
REFERENCES
1.
2.
3.
4.
5.
6.
7.
8.
Belloc NB, and Breslow L: Relationship of physical health status and health practices. Prev Med 1: 409-421, 1972.
Lalonde M: A new perspective on the health of Canadians: A working document.
Ottawa: National Health and Welfare, 1974.
McKeown T: Determinants of health. Hum Nature: April, 60-67, 1978.
Farguhar JW, Maccoby N, Wood PD, Alexander JK, Breitrose H, Brown BW, Jr,
Haskell WL, McAlister AL, Meyer AJ, Nash JD, and Stern MP: Community education
for cardiovascular health. Lancet, June: 1192-1195, 1977.
Maccoby N, and Alexander J: Use of media in lifestyle programs. In Davidson P (Ed):
Behavioral Medicine: Changing Health Lifestyles. New York: Brunner/Mazel, 1979.
Maccoby N, and Farquhar JW: Communication for health: Unselling heart disease.
J Communication 25: 114-126, 1975.
Koskela K, Puska P, and Tuomilehto J: The North Karelia project: A first evaluation.
Int J Health Educ 19: 59-66, 1976.
McAlister A, Puska P, Koskela K, Pallonen U, and Maccoby N: Psychology in action:
Mass communication and community organization for public health. Am Psychol
35:4, 375-379, 1980.
9.
10.
11.
12.
13.
14.
15.
16.
17.
18.
Tuomilehto J, Koskela K, Puska P, Biorkqvist S, and Salonen J: A community antismoking programme: Interim evaluation of the North Karelia project. InterJ Health
Educ, supplement to vol. 21: 4, 1-15, 1978.
Mielke KW, and Swinehart JW: Evaluation of the "Feeling Good" television series.
New York: Children’s Television Workshop, 1976.
Haskins JB: Evaluative research on the effects of mass communication safety cam-
paigns : A methodological critique.J Safety Res 2: 86-96, 1978.
Mendelsohn H: Mass communication for safety: A critical review and a proposed
theory. Chicago: National Safety Council, 1963.
Mendelsohn H: Some reasons why information campaigns can succeed. Public Opinion Q 37: 50-61, 1973.
Williams RA, Cousins LS, and Wilde, GJS: Communications, media, and audience effects upon attitude change with regard to automobile safety responsibility. Behav Res
Highway Safety 1:3, 155-171, 1970.
Robertson LS: The great seat belt campaign flop. J Communication 26: 4, 41-45, 1976.
Robertson LS, Kelley AB, O’Neill B, Wixom, CW, Eisworth RS, and Haddon W, Jr: A
controlled study of the effect of television messages on safety belt use. Am J Public
Heal 64: 1071-1080, 1974.
Kerpelman LC, Fax GE, and Nunes D: Evaluation of the effectiveness of outdoor
power equipment information and education programs. Contract report, U.S. Consumer Product Safety Commission. Cambridge, Mass: Abt Associates, Inc., 1978.
Best JA: Mass media, self-management, and smoking modification. In PO Davidson
and SM Davidson (Eds.) Behavioral Medicine: Changing Health Life Styles. New York:
Brunner/Mazel, 1980.
19.
Dubren R: Evaluation of
1977.
a
televised stop
smoking clinic. Public Heal Rep
92: 81-84,
143
Downloaded from http://heb.sagepub.com at UNIV OF ILLINOIS AT CHICAGO on August 25, 2007
© 1980 Society for Public Health Education. All rights reserved. Not for commercial use or
unauthorized distribution.
Green P: The mass media anti-smoking campaign around the world. Proceedings of
3rd World Conference on Smoking and Health (Vol. II), 245-253, 1975.
21. O’Keefe MT: The anti-smoking commercials: A study of television’s impact on behavior. Public Opinion Q 35: 2, 242-248, 1971.
22. Warner KE: The effects of the anti-smoking campaign on cigarette consumption. Am
J Public Heal 67: 645-650, 1977.
23 Blane HT, and Hewitt LC: Mass media, public education and alcohol: A state-of-art
review. Prepared for the National Institute on Alcohol Abuse and Alcoholism,
Alcohol, Drug Abuse and Mental Health Administration, 1977
24. Kline FG: Evaluation of a multimedia drug education program. J Drug Educ 2: 3,
229-239, 1972.
25. Plant MA, Pirie F, and Kreitman N: Evaluation of the Scottish Health Education Units
1976 Campaign on Alcoholism. J Soc Psychiat 14:1, 11-24, 1979.
26. Planned Parenthood Federation of Canada. An assessment of the mass media campaign for family planning, 1973.
27. Udry JR, Clark LJ, Chase CL, and Levy M: Can mass media advertising increase contraceptive use? Fam Plann Perspect 4: 3, 37-44, 1972.
28. Young MC: Review of research and studies on the health education and related aspects of family planning (1967-1971): Communication, program planning, and evaluation. Health Educ Monogr 35: whole issue, 1973.
29. Barrett H: MTU NI AFYA - Health Education by radio in Tanzania. Combread (London), 21: 37-38, 1973.
30. Cooke TM, and Ronweber ST: Radio, advertising techniques, and nutrition education:
A summary of a field experiment in the Phillipines and Nicaragua. Washington, D.C.:
20.
AID, 1977.
31.
32.
33.
34.
35.
36.
37.
38.
39.
40.
41.
42.
43.
44.
45.
Hall B, and Zikambona C: An evaluation of the 1973 mass health education campaign in Tanzania (Studies in Adult Education, No. 12). Dar es Salaam: Institute of
Adult Education, 1974.
Ramadasmurthy V, Hanumantha RD, Clarence ID, and Balasubramanian SC: Nutrition education and SITE telecasts. Int J Health Educ 21: 3, 168-173, 1978.
Zaltman G, Hingson R, and Allwood J: The impact of education and of mass media
exposure on child feeding in Costa Rica. IntJ Health Educ 13: 3, 103-112, 1970.
Butler M, and Paisley W: Communicating cancer control to the public. Health Educ
Monogr 5: 5-24, 1977.
Hingson R: Obtaining optimal attendance at mass immunization programs. Health
Serv Rep 89: 53-64, 1974.
Salzer JE, Marshall CL, and Glazer ER: The use of cable television as a tool in health
education of the elderly: Screening. Health Educ Monogr 5: 363-378, 1977.
SerVass B, and Weinberger MH: Use of multi-media motivation in enhancing compliance of hypertensives discovered at a screening operation. AmJ Public Health 69:
382-388, 1979.
Sundal M, and Schanie CF: Community mental health and mass media preventive education : The alternatives project. Soc Serv Rev June: 297-306, 1978.
Worden JK, Sweeney RR, and Waller JA: Audience interest in mass media messages
about lung disease in Vermont. Am J Public Health 68: 378-382, 1978.
Flay BR, Edison CN, and Dick J: Mass media in health safety and promotion: An annotated bibliography. Canada: University of Waterloo, 1980.
Stickell DW: A critical review of the methodology and results of research comparing
televised and face-to-face instruction. Doctoral dissertation, Pennsylvania State
University, 1963.
Abt CC (Ed.): The evaluation of social programs. Beverly Hills: Sage, 1976.
Campbell DT: Reforms as experiments. Am Psychol 24: 409-429, 1969. Also in F.G.
Caro (Ed.) Readings in Evaluation Research. New York: Russell Sage Foundation,
233-261, 1971.
Campbell DT, and Stanley JC: Experimental and quasi-experimental designs for research. Chicago: Rand-McNally, 1966.
Cook TD, Del Rosario ML, Hennigan KM, Mark M, and Trachim WMK (Eds): Evaluation Studies Review Annual (Vol. 3). Beverly Hills: Sage, 1978.
144
Downloaded from http://heb.sagepub.com at UNIV OF ILLINOIS AT CHICAGO on August 25, 2007
© 1980 Society for Public Health Education. All rights reserved. Not for commercial use or
unauthorized distribution.
46.
DT: The design and conduct of true experiments and quasisettings. In M.D. Dunnette (Ed.) Handbook of Industrial and Organizational Psychology. Chicago: Rand-McNally, 1976.
Cook TD, and Campbell DT: Quasi-Experimentation: Design and Analysis Issues.
Cook TD, and
experiments
47.
48.
49.
50.
51.
52.
53.
54.
55.
Campbell
in field
Chicago: Rand-McNally, 1979.
Flay BR, and Best JA: Design problems in the evaluation of health behavior change
programs. Preprint, Canada: University of Waterloo, 1980.
Glass GV, (Ed): Evaluation Studies Review Annual (Vol. 1). Beverly Hills: Sage, 1976.
Guttentag M (Ed): Evaluation studies review annual (Vol. 2) Beverly Hills: Sage, 1977.
Guttentag M, and Struening EL: Handbook of Evaluation Research (Vol. 2). Beverly
Hills: Sage, 1975.
Hennigan KM, Flay BR, and Haag RA: Clarification of terms and concepts commonly
used in evaluative research. In RE Klein, MS Read, HW Riecken, JA Brown, A
Peradelli, and CH Daza (Eds.): Evaluating the Impact of Nutrition and Health
Programs. New York: Plenum, 1979.
Klein RE, Read MS, Riecken, HW, Brown JA, Peradelli A, and Daza CH (Eds): Evaluating the Impact of Nutrition and Health Programs. New York: Plenum, 1979.
Riecken HW, and Boruch RF, et al. Social Experimentation: A Method For Planning
and Evaluating Social Interventions. New York: Academic Press, 1974.
Rutman L (Ed): Evaluation Research Methods: A Basic Guide. Beverly Hills: Sage,
1977.
56.
Shortell SM, and Richardson WC: Health Program Evaluation. St. Louis: C.V. Mosby,
1978.
61.
Streuning EL, and Guttentag M: Handbook of Evaluation Research (Vol. 1). Beverly
Hills: Sage, 1975.
Suchman EA: Evaluative research: principles and practice in public service and social
action programs. New York: Russell Sage Foundation, 1967.
Weiss CH: Evaluation Research: Methods of Assessing Program Effectiveness. Englewood Cliffs, N.J.: Prentice-Hall, 1972.
Atkin CK: Research evidence on mass mediated health communication campaigns.
Communication Yearbook 3, New Brunswick, New Jersey: Transaction, 1979.
Bauer R: The obstinate audience: The influence process from the point of view of so-
62.
cial communications. Am Psychol
19: 319, 1964.
Griffiths W, and Knutson AL: The role of mass media in public health. Am J Public
57.
58.
59.
60.
63.
64.
65.
66.
67.
68.
69.
70.
71.
72.
73.
Health 50: 515-523, 1960.
Hymann H, and Sheatsley P: Some reasons why information campaigns fail. Public
Opinion Q 11: 412-423, 1947.
Katz E, and Lazarsfeld PF: Personal Influence. New York: Free Press, 1955.
Klapper JL: The Effects of Mass Communication. Glencoe, III.: Free Press, 1960.
Hovland CI, Janis IL, and Kelley HH: Communication and Persuasion. New Haven:
Yale Press, 1953.
Hovland CI, Lumsdaine AA, and Sheffield FD: Experiments on Mass Communication.
Princeton, N.J.: Princeton University Press, 1949.
McGuire WJ: Personality and susceptibility to social influence. In EF Borgatta, WW
Lambert (Eds.), Handbook of Personality Theory and Research. Chicago:
Rand-Mc-Nally, 1968.
McGuire WJ: The nature of attitudes and attitude change. In G Lindzey and E
Aronson (Eds): The Handbook of Social Psychology (2nd ed.) (Vol. 3). Reading, Mass.:
Addison-Wesley, 1969.
McGuire WJ: Attitude change: The information processing paradigm. In CG McClintock (Ed): Experimental Social Psychology. New York: Holt, Rinehart, & Winston, 1972.
McGuire WJ: Persuasion, resistance, and attitude change. InI deSola Pool, W
Schramm, et al., (Eds,): Handbook of Communication. Chicago: Rand-McNally, 1973.
McGuire WJ: The concepts of attitude and their relations to behaviors. In SH Wallace
and LA Broedling (Eds): Perspectives on Attitude Assessment. Washington, D.C.:
Smithsonian Institute, 1975.
McGuire WJ: An information-processing model of advertising effectiveness. In HL
Davis and AJ Silk (Eds): Behavioral and Management Science in Marketing. New York:
Wiley, 1978.
145
Downloaded from http://heb.sagepub.com at UNIV OF ILLINOIS AT CHICAGO on August 25, 2007
© 1980 Society for Public Health Education. All rights reserved. Not for commercial use or
unauthorized distribution.
74.
75.
76.
77.
78.
79.
80.
81.
82.
83.
84.
Roberts DF: Attitude change and the motivation of health practices. In AJ Enelow
andJB Henderson, Applying behavioral science to cardiovascular risk: Proceedings of
a conference (Seattle, Washington, June 1976). American Heart Association, Inc.,
1975.
Zimbardo PG, Ebbesen EB, and Maslach C: Influencing Attitudes and Changing
Behavior (Second Edition). Reading, Mass.: Addison-Wesley, 1977.
Ray ML: Marketing communication and the hierarchy-of-effects. In IP Clarke (Ed):
New Models for Mass Communication Research. Beverly Hills: Sage, 1973.
Cartwright D: Some principles of mass persuasion: Selected findings of research on
the sale of United States War Bonds. Hum Relat 11: 253-267, 1949.
Allen, WH: Media stimulus and types of learning Audio-Visual Instr 12: 27-31, 1967.
Bloom BS, Engelhart MD, Furst EJ, Will WH, and Krathwohl DR: Taxonomy of Education Objectives. Handbook I: Cognitive Domain. New York: McKay, 1956.
Briggs LJ: Handbook of Procedures for the Design of Instruction. Pittsburgh, Pa.:
American Institutes for Research, 1970.
Briggs LJ, Campeau, PL, Gagne RM, and May MA: Instructional Media. Pittsburgh,
Pa.: American Institutes for Research, 1967.
Campeau PL: Selective review of the results of research on the use of audio-visual
media to teach adults. AV Commun Rev 22: 5-40, 1974.
Gagne RM, and Briggs LJ: Principles of Instructional Design. New York: Holt, Rinehart,
& Winston, 1974.
Jamison DT, and McAnany EG: Radio for Education and Development. Beverly Hills:
Sage, 1978.
85.
86.
87.
88.
Salomon G, and Clark RE: Reexamining the methodology of research on media and
technology in education. Re Educ Res 47: 99-120, 1977
Schramm W: Big Media Little Media: Tools and Technologies for Instruction. Beverly
Hills: Sage, 1977.
Jamison DT, Kleas, SJ, and Wells SJ: The Costs of Educational Media: Guidelines for
Planning and Evaluation. Beverly Hills: Sage, 1978.
Fishbein M (Ed): Readings in Attitude Theory and Measurement. New York: Wiley,
1967.
89.
Fishbein M, and Ajzen I: Belief, Attitude, Intention, and Behavior. Reading, Mass.:
90.
Addison-Wesley, 1975.
Flay BR: Catastrophe theory
91.
92.
93.
94.
95.
96.
97.
98.
99.
in psychology: Some applications to attitudes and social
behavior. Beha Sci 23. 335-350, 1978.
Greenwald AG, Brock TC, and Ostrom TM (Eds): Psychological Foundations of Attitudes. New York: Academic Press, 1968.
Hovland CI, and Rosenberg M (Eds): Attitude Organization and Change. New Haven:
Yale University Press, 1960.
Kiesler CA, Collins BE, and Miller N: Attitude Change. New York: Wiley, 1969.
Oskamp S: Attitudes and Opinions. Englewood Cliffs, N.J.: Prentice-Hall, 1977.
Triandis HC: Attitudes and Attitude Change. New York: Wiley, 1971.
Cook TD, and Flay BR: The persistence of experimentally induced attitude change. In
L Berkowitz (Ed): Advances in Experimental Social Psychology (Vol. 11). New York:
Academic Press, 1978.
Hass RG, and Mann RW: Anticipatory belief change: Persuasion or impression management? J Per Soc Psycho 34: 105-111, 1976
NuttinJM, Jr.: The Illusion of Attitude Change: Toward A Response Contagion Theory
of Persuasion. New York: Academic Press, 1975.
Wilson GT: Behavioral treatment of obesity: Maintenance strategies and long-term
efficacy. Preprint, Graduate School of Applied and Professional Psychology, New
Brunswick,
100.
101.
New Jersey, 1978.
Best JA, and Bloch M: Compliance in the control of cigarette smoking. In RB Haynes,
DW Tayler, and DL Sackett (Eds): Compliance with Therapeutic and Preventive
Regimens. Baltimore: Johns Hopkins University, 1979.
McAlister A: Television as a medium for delivering behavior therapy: A pilot
study of a televised smoking cessation program. Paper presented at the Association
for the Advancement of Behavior Therapy, 10th Annual Convention, New York, 1976.
146
Downloaded from http://heb.sagepub.com at UNIV OF ILLINOIS AT CHICAGO on August 25, 2007
© 1980 Society for Public Health Education. All rights reserved. Not for commercial use or
unauthorized distribution.
102.
modification programmes for health lifeRJ Lauzon (Ed): Seminar on the Evaluation of Health Education
and Behaviour Modification Programs. Ottawa: Canadian Health Education Society,
Best JA, and Flay BR:
intervention. In
Evaluating behaviour
styles
1978.
103.
Brownell KD, Herckerman CL, Westlake RJ, Hayes SC, and Monti PM: The effect of
in the behavioral treatment of obesity.
Behav Res Ther 16: 323-333, 1978.
Lichtenstein E, Antonuccio DO, and Rainwater G: Unkicking the habit: The resumption of cigarette smoking. Paper presented at the annual meeting of the Western
Psychological Association, Seattle, 1977.
Wicker AW: An examination of the "other variables" explanation of attitude-behavior inconsistency. J Per Soc Psychol
19: 18-30, 1971.
Marlatt GA, and Gordon JR: Determinants of relapse: Implications for the maintenance of behavior change. In PO Davidson (Ed): Behavioral Medicine: Changing
Health Lifestyles. New York: Brunner/Mazel, 1979.
Feather NT: Subjective probability and decision under uncertainty. Psychol Rev 66:
couples training and partner cooperativeness
104.
105.
106.
107.
150-164, 1959.
Maiman LA, and Becker MH: The health belief model: Origins and correlates in psychological theory. In MH Becker (Ed): The Health Belief Model and Personal Health
Behavior. Thorofare, N.J.: C.B. Slack, 1974.
109. Becker MH (Ed): The Health Belief Model and Personal Health Behavior. Thorofare,
N.J.: C.B. Slack, Inc., 1974.
110. Rokeach M: Beliefs, Attitudes, and Values: A Theory of Organization and Change.
San Francisco: Jossey-Bass, 1968.
111. Rokeach M: The Nature of Human Values. New York: Free Press, 1973.
112. Bandura A: Social Learning Theory. Morristown, N.J.: General Learning Press, 1971.
113. Bandura A: The self system in reciprocal determinism. Am Psychol 33: 344-358, 1978.
114.
Flay BR: An integrative model of the attitude and behavior change process in health
promotion. Preprint, Canada: University of Waterloo, 1980.
115. Abelson RP, Aronson E, McGuire WJ, Newcomb TM, Rosenberg MJ, and Tannenbaum
PH (Eds): Theories of Cognitive Consistency: A Sourcebook. Chicago: Rand-McNally,
108.
1969.
116.
117.
Fishbein M, Ajzen I: Attitudes toward objects as predictors of single and multiple behavioral criteria. Psychol Rev 81: 59-74, 1974.
Hanneman G, McEwen W, and Coyne S: Public service advertising on television. J
Broadcasting 17: 387-404, 1973.
147
Downloaded from http://heb.sagepub.com at UNIV OF ILLINOIS AT CHICAGO on August 25, 2007
© 1980 Society for Public Health Education. All rights reserved. Not for commercial use or
unauthorized distribution.